Download as pptx, pdf, or txt
You might also like
- Circulatory System Revision WorksheetDocument4 pagesCirculatory System Revision WorksheetPoulomi Sengupta100% (1)
- Abnormal Heart Sounds: First Heart Sound (S)Document4 pagesAbnormal Heart Sounds: First Heart Sound (S)Faris Mufid MadyaputraNo ratings yet
- Heart SoundDocument2 pagesHeart SounddamarisapNo ratings yet
- Extra Systolic Heart SoundDocument23 pagesExtra Systolic Heart SoundAtmaja R. SirupangNo ratings yet
- MURMURDocument21 pagesMURMURtoyyibNo ratings yet
- HEART AND LUNG SOUNDS: Reading For IVMS Heart and Lung Auscultation PageDocument87 pagesHEART AND LUNG SOUNDS: Reading For IVMS Heart and Lung Auscultation PageMarc Imhotep Cray, M.D.100% (4)
- Principles Auscultatory Areas: ND NDDocument5 pagesPrinciples Auscultatory Areas: ND NDPinay YaunNo ratings yet
- Mid-Systolic Ejection: Time Condition DescriptionDocument3 pagesMid-Systolic Ejection: Time Condition DescriptionZahrosofi AhmadahNo ratings yet
- IVMS Heart and Lung Auscultation Sounds NotesDocument7 pagesIVMS Heart and Lung Auscultation Sounds NotesMarc Imhotep Cray, M.D.No ratings yet
- Heart SoundsDocument17 pagesHeart SoundsAlfrin Antony100% (3)
- 09 - Mastering First Heart SoundDocument10 pages09 - Mastering First Heart SoundSharan MurugaboopathyNo ratings yet
- Heart Sounds: Mitral Regurgitation Congestive Heart FailureDocument6 pagesHeart Sounds: Mitral Regurgitation Congestive Heart FailurecindyNo ratings yet
- Heart SoundDocument16 pagesHeart SoundAnggraeni Prameswari PutriNo ratings yet
- AuscultationDocument41 pagesAuscultationAnonymous ZUaUz1wwNo ratings yet
- Tutorial 8 Cardiac ExamDocument14 pagesTutorial 8 Cardiac Examcindy100% (1)
- Prof. Maharlika Levi Sumilang: Heart Assessment NCM112 MS RLE 8/7/21Document6 pagesProf. Maharlika Levi Sumilang: Heart Assessment NCM112 MS RLE 8/7/21Yman Gio BumanglagNo ratings yet
- Heart SoundsDocument21 pagesHeart SoundsasakingofhNo ratings yet
- Heart SoundsDocument56 pagesHeart SoundsBetsy Babilonia100% (1)
- 7 Heart Sounds LectureDocument27 pages7 Heart Sounds LecturebvkjtzrvnyNo ratings yet
- Heart Sounds and Arteriovenous Pulses: DR Chandana HewageDocument48 pagesHeart Sounds and Arteriovenous Pulses: DR Chandana HewagePrasad HewawasamNo ratings yet
- Cvs ExaminationDocument50 pagesCvs ExaminationBanmeetNo ratings yet
- CVS1 - K18 - Cardiac AbnormalitiesDocument21 pagesCVS1 - K18 - Cardiac AbnormalitiesKassatria HiaNo ratings yet
- 7th Heart Sounds and MurmursDocument6 pages7th Heart Sounds and MurmursbabibubeboNo ratings yet
- Cardio 2Document2 pagesCardio 2Erika De JesusNo ratings yet
- The Myth of The HabandurasoDocument15 pagesThe Myth of The HabandurasoAlrick GonzalezNo ratings yet
- Atrial, Jugular Pressures and Heart SoundDocument11 pagesAtrial, Jugular Pressures and Heart Soundtehillahkabwe100No ratings yet
- Cardiac Cycle - Atrial Contraction (Phase 1)Document10 pagesCardiac Cycle - Atrial Contraction (Phase 1)Fatima KhanNo ratings yet
- Shched Vii Admission 142 Spring 2021Document21 pagesShched Vii Admission 142 Spring 2021AKANKSHA RANANo ratings yet
- Heart Sounds and MurmursDocument38 pagesHeart Sounds and MurmursLaura Moise100% (5)
- HeartDocument25 pagesHeartdeepmazumderNo ratings yet
- Cardiac MurmursDocument53 pagesCardiac MurmursdrgashokNo ratings yet
- Valves Part 2Document2 pagesValves Part 2AIKA BAYANo ratings yet
- Heart Murmurs Topic Review - From Description To AuscultationDocument15 pagesHeart Murmurs Topic Review - From Description To AuscultationRapmle PrasadNo ratings yet
- S1 and S2: Valves) at The Start of The Systolic Contraction of The VentriclesDocument10 pagesS1 and S2: Valves) at The Start of The Systolic Contraction of The VentriclesCHARIEMAE CA�AZARESNo ratings yet
- Heart Sounds PDFDocument38 pagesHeart Sounds PDFZennon Blaze ArceusNo ratings yet
- Auscultatia CardiacaDocument9 pagesAuscultatia CardiacaMh MhNo ratings yet
- Apical Pulse AssessmentDocument9 pagesApical Pulse AssessmentmscastrogelacastroNo ratings yet
- Lecture 13 Heart SoundsDocument36 pagesLecture 13 Heart SoundsMooma fatima100% (1)
- Cardiac Cycle - Atrial Contraction (Phase 1) : A-V Valves Open Semilunar Valves ClosedDocument10 pagesCardiac Cycle - Atrial Contraction (Phase 1) : A-V Valves Open Semilunar Valves ClosedFatima KhanNo ratings yet
- CVS Examination EditedDocument134 pagesCVS Examination EditedThilak JayalathNo ratings yet
- Angelina A Joho MSC in Critical Care and TraumaDocument50 pagesAngelina A Joho MSC in Critical Care and TraumaZabron LuhendeNo ratings yet
- Heart & Neck Vessels Assessment: Kousar Perveen Assistant Professor The University of LahoreDocument46 pagesHeart & Neck Vessels Assessment: Kousar Perveen Assistant Professor The University of LahoreChenii RoyNo ratings yet
- Cardiac Cycle: Heart Murmurs: Mary Beth Fontana MDDocument43 pagesCardiac Cycle: Heart Murmurs: Mary Beth Fontana MDlessank12No ratings yet
- Week 5 1Document6 pagesWeek 5 1deanNo ratings yet
- Cardiac PhysiologyDocument12 pagesCardiac PhysiologyJoezer Gumangan VeranoNo ratings yet
- 4 4 14 Cardiac Cycle and Heart Sounds Parts I II Fontana 3Document32 pages4 4 14 Cardiac Cycle and Heart Sounds Parts I II Fontana 3lessank12No ratings yet
- Mitral StenosisDocument15 pagesMitral StenosisAshwin Aby ThomasNo ratings yet
- The Cardiac CycleDocument19 pagesThe Cardiac CycleRebi NesroNo ratings yet
- Aortic Stenosis Differential DiagnosisDocument12 pagesAortic Stenosis Differential DiagnosisCristina PorfireNo ratings yet
- Suara JantungDocument12 pagesSuara JantungTesis Maruli Tua SianiparNo ratings yet
- 347 Heart Sounds & MurmursDocument9 pages347 Heart Sounds & MurmursAbcdNo ratings yet
- Heart MurmursDocument13 pagesHeart MurmursChen BrionesNo ratings yet
- S and S: Presenter: Guidance and ModerationDocument60 pagesS and S: Presenter: Guidance and ModerationCatherine PaulNo ratings yet
- Acyanotic Heart DiseaseDocument18 pagesAcyanotic Heart DiseaseShishir ShresthaNo ratings yet
- 5 Cardiac Cycle & Heart SoundsDocument32 pages5 Cardiac Cycle & Heart SoundsDisha SuvarnaNo ratings yet
- Cardiovascular Physiology: Lawrence A. Olatunji ReaderDocument46 pagesCardiovascular Physiology: Lawrence A. Olatunji ReaderMaryam Ogunade0% (1)
- Heart Sounds - PracticalDocument7 pagesHeart Sounds - Practicalshadapaaak100% (1)
- Bookshelf NBK341Document4 pagesBookshelf NBK341RidlaAchmadNo ratings yet
- Cardiovascular Physical ExaminationDocument28 pagesCardiovascular Physical ExaminationYusrina AdaniNo ratings yet
- Differential Diagnosis of The Diseases With Systolic MurmursDocument2 pagesDifferential Diagnosis of The Diseases With Systolic MurmursXiang Yun TanNo ratings yet
- The New Ropanasuri Journal of Surgery The New Ropanasuri Journal of SurgeryDocument6 pagesThe New Ropanasuri Journal of Surgery The New Ropanasuri Journal of SurgeryMeiriyani LembangNo ratings yet
- Ameloblastoma: Current Etiopathological Concepts and ManagementDocument11 pagesAmeloblastoma: Current Etiopathological Concepts and ManagementMeiriyani LembangNo ratings yet
- Neonatal Respiratory Distress Syndrome: Chest X-Ray or Lung Ultrasound? A Systematic ReviewDocument13 pagesNeonatal Respiratory Distress Syndrome: Chest X-Ray or Lung Ultrasound? A Systematic ReviewMeiriyani LembangNo ratings yet
- Neonatal Lung Disorders: Pattern Recognition Approach To DiagnosisDocument12 pagesNeonatal Lung Disorders: Pattern Recognition Approach To DiagnosisMeiriyani LembangNo ratings yet
- Unit 1 Molecules, Diet, Transport and HealthDocument9 pagesUnit 1 Molecules, Diet, Transport and HealthNandiNo ratings yet
- Anatomy and Physiology of The Heart: Dr. N. PraveenDocument56 pagesAnatomy and Physiology of The Heart: Dr. N. Praveenamjad khan100% (1)
- Laporan Echo (Achmad Firdaus, TN.)Document1 pageLaporan Echo (Achmad Firdaus, TN.)radiologi vaniaNo ratings yet
- The Cardiac Cycle and The Physiologic Basis of Left Ventricular Contraction, Ejection, Relaxation, and FillingDocument13 pagesThe Cardiac Cycle and The Physiologic Basis of Left Ventricular Contraction, Ejection, Relaxation, and FillingFanindya HadamuNo ratings yet
- RV Dysfunction - Assessment by EchocardiographyDocument52 pagesRV Dysfunction - Assessment by EchocardiographyNag Mallesh RaoNo ratings yet
- Tsktccts 8800 Plus EngDocument13 pagesTsktccts 8800 Plus EngRandom ProjectNo ratings yet
- 18 The Cardiovascular System - The Heart PDFDocument33 pages18 The Cardiovascular System - The Heart PDFDaniel DanielNo ratings yet
- CBD Dr. Saugi - Robby GunawanDocument159 pagesCBD Dr. Saugi - Robby GunawanRobby GumawanNo ratings yet
- Cardio Notes 2Document11 pagesCardio Notes 2AngieNo ratings yet
- Unit 2 notes-ME..Document23 pagesUnit 2 notes-ME..Kowsi MathiNo ratings yet
- Cardiovascular System: The Heart: Chapter 19 - Lecture NotesDocument73 pagesCardiovascular System: The Heart: Chapter 19 - Lecture Noteshersheys72002No ratings yet
- Tif31Document41 pagesTif31HCX dghhqNo ratings yet
- Hemodynamic Assessment in The Contemporary ICUDocument33 pagesHemodynamic Assessment in The Contemporary ICUnacxit6No ratings yet
- 515Document972 pages515solecitodelmarazul100% (6)
- CHN Ncm112b Rle RequirementDocument27 pagesCHN Ncm112b Rle RequirementPatricia VasquezNo ratings yet
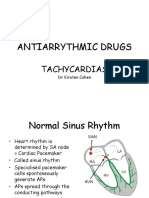
- Antiarrythmic Drugs: TachycardiasDocument36 pagesAntiarrythmic Drugs: TachycardiasDrDeepak PawarNo ratings yet
- Pulse DiagnosesDocument454 pagesPulse DiagnosesSean C InselbergNo ratings yet
- First Description of TVD in Basset HoundDocument4 pagesFirst Description of TVD in Basset HoundFlorencia SeneseNo ratings yet
- KD Pda DanielDocument38 pagesKD Pda DanielDavid JonathanNo ratings yet
- Heart PathophysiologyDocument20 pagesHeart PathophysiologyDoctorDrapion100% (2)
- Mitral Valve ProlapseDocument3 pagesMitral Valve ProlapseKristine CastilloNo ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument69 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNo ratings yet
- IJGMP - RV Function Assessment Pre and Post PTMC in Patients With Severe - AutosavedDocument8 pagesIJGMP - RV Function Assessment Pre and Post PTMC in Patients With Severe - AutosavedImpact JournalsNo ratings yet
- Human HeartDocument2 pagesHuman HearthaniimanNo ratings yet
- Physiology PDFDocument14 pagesPhysiology PDFBalaji Kumar PanigrahiNo ratings yet
- Lin 2009Document7 pagesLin 2009Nur Syamsiah MNo ratings yet
- Human Physiology 14th Edition Fox Solutions ManualDocument16 pagesHuman Physiology 14th Edition Fox Solutions Manualoraliemaximusp474w3100% (31)
- Cardiac Cycle ExplainedDocument5 pagesCardiac Cycle ExplainedCai Peng FeiNo ratings yet
- Wigger's Diagram WorksheetDocument6 pagesWigger's Diagram WorksheetYina BambinaNo ratings yet