Download as ppt, pdf, or txt
You might also like
- Caterpillar 627g Wheel Trator Scraper Operation and Maintenance ManualDocument3 pagesCaterpillar 627g Wheel Trator Scraper Operation and Maintenance Manualcornelia100% (47)
- Pathophysiology of FractureDocument2 pagesPathophysiology of FractureAnne Lorraine Bringas93% (27)
- Brain CTDocument83 pagesBrain CTArvind Jha100% (2)
- (Mantap) Slide Materi Bedah-1 Batch 3 2018 PDFDocument93 pages(Mantap) Slide Materi Bedah-1 Batch 3 2018 PDFKomang Sudiase67% (3)
- Pelvic TiltingDocument28 pagesPelvic Tiltingvenkata ramakrishnaiahNo ratings yet
- Massachusetts - Protocols - 04.05.2019 - Cu Bookmarks PDFDocument557 pagesMassachusetts - Protocols - 04.05.2019 - Cu Bookmarks PDFMarius AlexandrescuNo ratings yet
- CT Scans of The Head: A Neurologist's Perspective: Lara Cooke January 15, 2009Document111 pagesCT Scans of The Head: A Neurologist's Perspective: Lara Cooke January 15, 2009adrian100% (1)
- Neuroimaging For Medical Residents: Kanokwan Boonyapisit, M.D. Department of Medicine Siriraj HospitalDocument106 pagesNeuroimaging For Medical Residents: Kanokwan Boonyapisit, M.D. Department of Medicine Siriraj HospitalRapid Medicine100% (5)
- Chapter 2 Intro To Brain ImagingDocument49 pagesChapter 2 Intro To Brain ImagingJellie MendozaNo ratings yet
- NeurologyDocument37 pagesNeurologyDevangkumar PatelNo ratings yet
- Neuroradiology Sah and StrokeDocument81 pagesNeuroradiology Sah and StrokeJujhar BoparaiNo ratings yet
- How To Read A Head CT: DR Mohamed El Safwany. MDDocument60 pagesHow To Read A Head CT: DR Mohamed El Safwany. MDYusuf BrilliantNo ratings yet
- Introduction To Clinical Medicine (ICM) : Case Studies Neurologic DisordersDocument142 pagesIntroduction To Clinical Medicine (ICM) : Case Studies Neurologic DisordersomarNo ratings yet
- Head InjuryDocument50 pagesHead InjuryThiagarajah RaviNo ratings yet
- Anesthetic Management of Intracranial Aneurysms R-MasriDocument66 pagesAnesthetic Management of Intracranial Aneurysms R-MasriadheNo ratings yet
- Brain InjuryDocument35 pagesBrain InjuryAkhil Adhithyan Ram100% (1)
- Cara Membaca CTDocument61 pagesCara Membaca CTDio Alexander100% (1)
- Intracranial HemorrhageDocument75 pagesIntracranial HemorrhageDea DNo ratings yet
- Pedia SGD NICUDocument62 pagesPedia SGD NICUJAIRISH YZABELLE SALVADORNo ratings yet
- Self-Study - 18 - NeuropsychiatricDocument137 pagesSelf-Study - 18 - NeuropsychiatricAdeyemi OlusolaNo ratings yet
- DR HJ Asmah Yusuf SP - Rad DR Evo Elidar HRP SP - RadDocument86 pagesDR HJ Asmah Yusuf SP - Rad DR Evo Elidar HRP SP - RadnikiNo ratings yet
- StrokeDocument74 pagesStrokeDonnaBells Hermo Labaniego100% (2)
- How To Read A Head CT ScanDocument34 pagesHow To Read A Head CT ScanBoby ArisofianNo ratings yet
- Neuro BN All PDFDocument50 pagesNeuro BN All PDFDokki ScanNo ratings yet
- Stroke: Health Education HFT 201 By: Sophia Kol, MDDocument16 pagesStroke: Health Education HFT 201 By: Sophia Kol, MDTith SeavmeyNo ratings yet
- Head CT Scan PDFDocument89 pagesHead CT Scan PDFLiri AndiyaniNo ratings yet
- Review To CNS Radiology Including SSDocument52 pagesReview To CNS Radiology Including SSBisher Al-halabiNo ratings yet
- Head InjuryDocument64 pagesHead Injurybuttashly125No ratings yet
- 5.radiologi Terapan CT Scan MriDocument87 pages5.radiologi Terapan CT Scan MriAde CahyaningtyasNo ratings yet
- Media 221736 enDocument58 pagesMedia 221736 ensamNo ratings yet
- Head Injuries 2015Document41 pagesHead Injuries 2015jimmyNo ratings yet
- CSF and MeningesDocument45 pagesCSF and MeningesdemondodyNo ratings yet
- Intracranial AneurysmDocument4 pagesIntracranial AneurysmJayson CinenseNo ratings yet
- Case PresDocument44 pagesCase PresPhilia FeliceNo ratings yet
- Cerebellar Abscess: Ade SofiyanDocument31 pagesCerebellar Abscess: Ade SofiyanRenzo DavindraNo ratings yet
- Ntroduction To The Physical ExaminationDocument4 pagesNtroduction To The Physical ExaminationAngelica NenitaNo ratings yet
- Basic CTDocument71 pagesBasic CTRapid Medicine100% (2)
- Micro and MacrocephalyDocument27 pagesMicro and MacrocephalyAbdullah GadNo ratings yet
- Kuliah 3 - Tumor OtakDocument150 pagesKuliah 3 - Tumor Otaktutorial. aNo ratings yet
- Brain Imaging 2004-5finalDocument72 pagesBrain Imaging 2004-5finalCzar GrabNo ratings yet
- Nur 400 Neuro PP 2014Document84 pagesNur 400 Neuro PP 2014JoelVargheseNo ratings yet
- Head Injury AnesDocument42 pagesHead Injury Aneskenbon kenbonNo ratings yet
- Neurosurgery: UnprotectedDocument39 pagesNeurosurgery: UnprotectedMaulana Taufik100% (2)
- Neurologic Trauma: Traumatic Brain InjuryDocument18 pagesNeurologic Trauma: Traumatic Brain InjuryPearl Raiza Hadani100% (1)
- 4th Problem Emergency Medicine Group 1Document82 pages4th Problem Emergency Medicine Group 1Jonathan TandajuNo ratings yet
- Cerebral Aneurysm: By: Cristi Ne Reyes Al-Sundal, RN, MN NCM 118 InstuctorDocument21 pagesCerebral Aneurysm: By: Cristi Ne Reyes Al-Sundal, RN, MN NCM 118 InstuctorVhince Norben PiscoNo ratings yet
- Brain Herniation SyndromeDocument28 pagesBrain Herniation SyndromeSarahScandy100% (4)
- Stroke: Dr. Alberto CampodónicoDocument17 pagesStroke: Dr. Alberto CampodónicoJohn Domínguez MedinaNo ratings yet
- Instruments - Prof. ABM AbdullahDocument27 pagesInstruments - Prof. ABM Abdullahduniyajhaan19No ratings yet
- Care of Mother Child at Risk or With ProblemsDocument121 pagesCare of Mother Child at Risk or With ProblemsReena BuenaventuraNo ratings yet
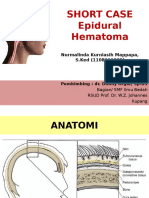
- SHORT CASE 1 Epidural HematomaDocument30 pagesSHORT CASE 1 Epidural HematomaNurmalinda MappapaNo ratings yet
- Brain-Attack or Stroke or Cerebrovascular-AccidentDocument29 pagesBrain-Attack or Stroke or Cerebrovascular-AccidentMission JupiterNo ratings yet
- CT Scan BasicsDocument28 pagesCT Scan BasicsPauline BurgosNo ratings yet
- Basic Approch To CT BrainDocument62 pagesBasic Approch To CT BrainS B SayedNo ratings yet
- Stroke by Dr. AM IyagbaDocument44 pagesStroke by Dr. AM IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- k10 - Kuliah Fk-Usu Nervous SystemDocument99 pagesk10 - Kuliah Fk-Usu Nervous SystemwlmhfpNo ratings yet
- Cerebrovascular Accident (CVA) "Stroke": Ma. Tosca Cybil A. Torres, RN, MANDocument53 pagesCerebrovascular Accident (CVA) "Stroke": Ma. Tosca Cybil A. Torres, RN, MANMa Tosca Cybil TorresNo ratings yet
- How To Approach To Normal MRI BrainDocument26 pagesHow To Approach To Normal MRI BraintiaraNo ratings yet
- CT ScanDocument84 pagesCT ScanHafiz Wajid SadiqNo ratings yet
- Head Injury 5Document68 pagesHead Injury 5drvishal bhattNo ratings yet
- Academic Group OF Internal Medicine - Revision Note of CVA-2010Document88 pagesAcademic Group OF Internal Medicine - Revision Note of CVA-2010abdallhNo ratings yet
- CT Scan (Brain) : DR Sana Rehman House Officer Medical Unit IDocument37 pagesCT Scan (Brain) : DR Sana Rehman House Officer Medical Unit ISana RehmanNo ratings yet
- The Ideal Heart Healthy Diet Cookbook; The Superb Diet Guide To Lower Your Blood Pressure And Cholesterol Levels With Nutritious Low Sodium Low Fat RecipesFrom EverandThe Ideal Heart Healthy Diet Cookbook; The Superb Diet Guide To Lower Your Blood Pressure And Cholesterol Levels With Nutritious Low Sodium Low Fat RecipesNo ratings yet
- The "Completely Randomised" and The "Randomised Block" Are The Only Experimental Designs Suitable For Widespread Use in Pre Clinical ResearchDocument5 pagesThe "Completely Randomised" and The "Randomised Block" Are The Only Experimental Designs Suitable For Widespread Use in Pre Clinical ResearchChris LeeNo ratings yet
- Cochrane Handbook 212019Document24 pagesCochrane Handbook 212019Chris LeeNo ratings yet
- Nursing Reflective Practice - An Empirical Literature ReviewDocument10 pagesNursing Reflective Practice - An Empirical Literature ReviewChris LeeNo ratings yet
- Sullivan Et Al 2018 - Should Multiple Imputation Be The Method of Choice For Handling Missing Data in Randomized TrialsDocument17 pagesSullivan Et Al 2018 - Should Multiple Imputation Be The Method of Choice For Handling Missing Data in Randomized TrialsChris LeeNo ratings yet
- Reflective Learning in Higher Education - A Comparative AnalysisDocument8 pagesReflective Learning in Higher Education - A Comparative AnalysisChris LeeNo ratings yet
- Reflections in LearningDocument17 pagesReflections in LearningChris LeeNo ratings yet
- Chemotherapy of Tuberculosis in Hong KongDocument17 pagesChemotherapy of Tuberculosis in Hong KongChris LeeNo ratings yet
- Reflection in and On Nursing Practices - How NursesDocument7 pagesReflection in and On Nursing Practices - How NursesChris LeeNo ratings yet
- RESmart - CPAP, Auto - User ManualDocument40 pagesRESmart - CPAP, Auto - User ManualChris LeeNo ratings yet
- Adult Cardiac Arrest Circular Algorithm: Monitor CPR QualityDocument1 pageAdult Cardiac Arrest Circular Algorithm: Monitor CPR QualityChris LeeNo ratings yet
- How To Read A Head CTDocument90 pagesHow To Read A Head CTChris LeeNo ratings yet
- Acute Stroke Management Resource:: Types of Stroke & Anatomy and Physiology of Acute StrokeDocument52 pagesAcute Stroke Management Resource:: Types of Stroke & Anatomy and Physiology of Acute StrokeChris LeeNo ratings yet
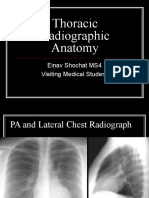
- Thoracic Radiographic Anatomy: Einav Shochat MS4 Visiting Medical StudentDocument81 pagesThoracic Radiographic Anatomy: Einav Shochat MS4 Visiting Medical StudentChris LeeNo ratings yet
- Nursing Tools Psychotherapy PDFDocument1 pageNursing Tools Psychotherapy PDFChris LeeNo ratings yet
- Pneumonia, Atelectasis & EffusionsDocument38 pagesPneumonia, Atelectasis & EffusionsChris LeeNo ratings yet
- CT Head and Ischemic Cva: What To Look For On The Early Scan??Document19 pagesCT Head and Ischemic Cva: What To Look For On The Early Scan??Chris LeeNo ratings yet
- CAPD - StaySafe Training Manual PDFDocument16 pagesCAPD - StaySafe Training Manual PDFChris LeeNo ratings yet
- Tagle vs. Anglo Eastern Crew Management Phils. Inc. Case DigestDocument2 pagesTagle vs. Anglo Eastern Crew Management Phils. Inc. Case DigestPAMELA PARCE100% (1)
- Horner'S Syndrome - : Far Eastern University - Nicanor Reyes Medical FoundationDocument3 pagesHorner'S Syndrome - : Far Eastern University - Nicanor Reyes Medical FoundationVictorija Evania Lucille DeldioNo ratings yet
- Cable Dray ATRDocument3 pagesCable Dray ATRferielvpkNo ratings yet
- Bones of The FootDocument23 pagesBones of The FootZaid AbdulqadirNo ratings yet
- 06.a Burn Injury-Dr Phillip BMC 1Document116 pages06.a Burn Injury-Dr Phillip BMC 1Erasto MwanganikaniNo ratings yet
- Sinclair Declaration UNREDACTED With ExhibitsDocument51 pagesSinclair Declaration UNREDACTED With ExhibitsCeleste FremonNo ratings yet
- Bracing Algorithm From CSMDocument6 pagesBracing Algorithm From CSMaustin packNo ratings yet
- Module Pe 9 Q1 W5 W6 AcDocument55 pagesModule Pe 9 Q1 W5 W6 AcNicole Faye RamosNo ratings yet
- Morning Report OrthopaediDocument28 pagesMorning Report OrthopaeditaniamaulaniNo ratings yet
- Liver TraumaDocument24 pagesLiver TraumaNununkNo ratings yet
- Management of Incarcerating Pincer-Type Femoroacetabular Impingement With Hip Arthroscopy - Arthroscopy TechniquesDocument1 pageManagement of Incarcerating Pincer-Type Femoroacetabular Impingement With Hip Arthroscopy - Arthroscopy TechniquesNica ReyesNo ratings yet
- Frog MusclesDocument2 pagesFrog MusclesPamela YusophNo ratings yet
- DROPS QuestionnaireDocument3 pagesDROPS QuestionnairePrimelift Safety Resources LimitedNo ratings yet
- Waiver For Plant TourDocument1 pageWaiver For Plant TourJuan Paulo FeliciaNo ratings yet
- Skeletal SystemDocument64 pagesSkeletal SystemGem Rose UretaNo ratings yet
- Comprehensive Summary of Anastomoses Between Median and Ulnar Nerve in The Forearm and HandDocument5 pagesComprehensive Summary of Anastomoses Between Median and Ulnar Nerve in The Forearm and HandMuhammad Imran MirzaNo ratings yet
- CLG612H Operation and Maintenance ManualDocument136 pagesCLG612H Operation and Maintenance Manualمهند احمدNo ratings yet
- Ch. 8 Student Packet (ANP)Document5 pagesCh. 8 Student Packet (ANP)Alex ZhangNo ratings yet
- Surgery (UWorld Step 2)Document39 pagesSurgery (UWorld Step 2)Nishok VSNo ratings yet
- Assessment of New BornDocument58 pagesAssessment of New BornEllen Angel100% (1)
- Care of Patients With Traction TractionDocument5 pagesCare of Patients With Traction TractionMOHAMMAD JABBER M. PAUDACJRNo ratings yet
- BOSH - OSH Situationer - As of Feb 2016 PDFDocument36 pagesBOSH - OSH Situationer - As of Feb 2016 PDFAganon AristotleNo ratings yet
- Lateral EpicondylitisDocument12 pagesLateral EpicondylitisIshitaNo ratings yet
- First Aid For Common Unintentional InjuriesDocument13 pagesFirst Aid For Common Unintentional InjuriesORENJI ORENJI ORENJINo ratings yet
- Pleural CavityDocument19 pagesPleural CavityAnigha PrasadNo ratings yet
- Chapter 9 - ArticulationsDocument25 pagesChapter 9 - ArticulationsCarolina HerasmeNo ratings yet