Download as pptx, pdf, or txt
You might also like
- TLA On Diabetes MellitusDocument3 pagesTLA On Diabetes MellitusJULIANNE BAYHON100% (1)
- Hypoglycemia Treatment ProtocolDocument1 pageHypoglycemia Treatment ProtocolCherryBeeNo ratings yet
- Dka and HHSDocument25 pagesDka and HHSMouhammad Dawoud100% (2)
- 01b. ACUTE COMPLICATIONS (KAD & HONK)Document42 pages01b. ACUTE COMPLICATIONS (KAD & HONK)febriNo ratings yet
- DKA Presentasi DR - Leonardo RevisiDocument34 pagesDKA Presentasi DR - Leonardo RevisiLeonardo LiswojoNo ratings yet
- Hyperglycemic CrisisDocument25 pagesHyperglycemic CrisisVentya Edita Madelyn SimamoraNo ratings yet
- Hyperglycemic Crises in Diabetes Mellitus: Yoshiaki Uda ICU TrainingDocument22 pagesHyperglycemic Crises in Diabetes Mellitus: Yoshiaki Uda ICU TrainingyoshiudaNo ratings yet
- Diabeticum Ketoacidosis: Ach. Najich RF, DRDocument16 pagesDiabeticum Ketoacidosis: Ach. Najich RF, DRAch Najich RfNo ratings yet
- Diabetic Coma: Kabera René, MD PGY III Resident Family and Community Medicine National University of RwandaDocument25 pagesDiabetic Coma: Kabera René, MD PGY III Resident Family and Community Medicine National University of RwandaKABERA RENENo ratings yet
- Diabetes KetoacidosisDocument27 pagesDiabetes Ketoacidosisyose rizal sinagaNo ratings yet
- Diabetes KetoacidosisDocument35 pagesDiabetes KetoacidosisdaniejayanandNo ratings yet
- Diabetic Ketoacidosis and Hyperglycaemic Hyperosmolar StateDocument4 pagesDiabetic Ketoacidosis and Hyperglycaemic Hyperosmolar StatemuhammadridhwanNo ratings yet
- Acute Complication of DMDocument41 pagesAcute Complication of DMWhite Crime100% (1)
- Diabetic Ketoacidosis (Dka) & Hyperosmolar Hyperglycemic Syndrome (HHS)Document54 pagesDiabetic Ketoacidosis (Dka) & Hyperosmolar Hyperglycemic Syndrome (HHS)Beyene FelekeNo ratings yet
- Hiperosmolar Non KetotikDocument24 pagesHiperosmolar Non KetotikMunawwar AweNo ratings yet
- Diabetic Ketoacidosis Hyperglycemic Hyperosmolar State: Dka Dan HhsDocument20 pagesDiabetic Ketoacidosis Hyperglycemic Hyperosmolar State: Dka Dan HhsRashellya RasyidaNo ratings yet
- Metabolic EmergenciesDocument53 pagesMetabolic EmergenciesWengel Redkiss100% (1)
- Diabetes Ketoacidosis: January 2014Document27 pagesDiabetes Ketoacidosis: January 2014Lydia nmesomaNo ratings yet
- Diabetes KetoacidosisDocument27 pagesDiabetes KetoacidosisLydia nmesomaNo ratings yet
- DKA For PEMDocument26 pagesDKA For PEMTemesgen AyanaNo ratings yet
- Kuliah Komplikasi Akut DiabetesDocument52 pagesKuliah Komplikasi Akut DiabetessatyasanthiniNo ratings yet
- Dka NewDocument37 pagesDka NewMuhammad FurqanNo ratings yet
- DM Acute & Chronic RXDocument67 pagesDM Acute & Chronic RXDrDeerren MatadeenNo ratings yet
- Dka Vs Hhs Edit 1Document25 pagesDka Vs Hhs Edit 1Razeen RiyasatNo ratings yet
- Penurunan Kesadaran 2. Sepsis 3. Gangguan Asam Basa 4. PatfisDocument111 pagesPenurunan Kesadaran 2. Sepsis 3. Gangguan Asam Basa 4. PatfisRosemary FebrianiNo ratings yet
- DKAPPTxDocument34 pagesDKAPPTxMuhammad FurqanNo ratings yet
- Hyperglycemia Syndromes: Diabetic Ketoacidosis Ketoacidosis-Hypersomolar ComaDocument35 pagesHyperglycemia Syndromes: Diabetic Ketoacidosis Ketoacidosis-Hypersomolar ComaPriyanka ChampanerkarNo ratings yet
- Acute Diabetes ComplicationsDocument7 pagesAcute Diabetes ComplicationsHala Salah IbrahimNo ratings yet
- Dks HhsDocument16 pagesDks HhsDebora Putri Fernanda SaragihNo ratings yet
- Diabetic Ketoacidosis (Dka)Document18 pagesDiabetic Ketoacidosis (Dka)dr.Bobi Ahmad Sahid, S.Kep100% (2)
- Diabetic Ketoacidosis Management: Heidi Chamberlain Shea, MDDocument29 pagesDiabetic Ketoacidosis Management: Heidi Chamberlain Shea, MDSiti RahmahNo ratings yet
- Shelly DKADocument18 pagesShelly DKARizkyastari OnnyNo ratings yet
- DM Acute CxnsDocument130 pagesDM Acute CxnsMohammed KedirNo ratings yet
- Dr. Mohamed Ali Hamedh - DKA - 2023Document25 pagesDr. Mohamed Ali Hamedh - DKA - 2023ÁýáFáŕőúgNo ratings yet
- W02 - Diabetic Emergencies in CCDocument36 pagesW02 - Diabetic Emergencies in CCHelene AlawamiNo ratings yet
- New Format MasterDocument34 pagesNew Format MasterMuhammad FurqanNo ratings yet
- Red Eye by DR MainuddinDocument38 pagesRed Eye by DR MainuddinMainuddin HasanNo ratings yet
- DKA and HHS The Washington Manual of Critical CareDocument6 pagesDKA and HHS The Washington Manual of Critical Careمحمد عقيلي100% (1)
- Diabetes Mellitus and Its Emergencies 1Document35 pagesDiabetes Mellitus and Its Emergencies 1Varun R'MenonNo ratings yet
- Seminar Presentation On Management of Diabetic Ketoacidosis BY:Kelil Kedir (CII)Document34 pagesSeminar Presentation On Management of Diabetic Ketoacidosis BY:Kelil Kedir (CII)Meraol HusseinNo ratings yet
- Acute DM ComplicationsDocument34 pagesAcute DM ComplicationsHillary RabinNo ratings yet
- (Tamtam) Hiperglikemia, Hipoglikemia, Hiperosmolar Asidosis Non KetotikDocument23 pages(Tamtam) Hiperglikemia, Hipoglikemia, Hiperosmolar Asidosis Non KetotikkynatroemanNo ratings yet
- Emd166 Slide Acute Complication of DiabetesDocument78 pagesEmd166 Slide Acute Complication of DiabetesSukma WicaturatmashudiNo ratings yet
- Diabetic Ketoacidosis: Michele Ritter, M.D. Argy Resident - February, 2007Document18 pagesDiabetic Ketoacidosis: Michele Ritter, M.D. Argy Resident - February, 2007poktaviantiNo ratings yet
- Hyperglycemic Emergencies: Boston University School of Medicine July, 2013 Marie Mcdonnell, MDDocument62 pagesHyperglycemic Emergencies: Boston University School of Medicine July, 2013 Marie Mcdonnell, MDBeyene FelekeNo ratings yet
- Diabetic KetoacidosisDocument5 pagesDiabetic KetoacidosisJill Catherine Cabana100% (3)
- Diabetic EmergencyDocument28 pagesDiabetic Emergencychandrima pattadarNo ratings yet
- Kad HHS 2019Document35 pagesKad HHS 2019Friska RamadayantiNo ratings yet
- Acute Complication of Diabetes Mellitus: Laksmi SasiariniDocument43 pagesAcute Complication of Diabetes Mellitus: Laksmi SasiariniClararida RiawanNo ratings yet
- EMERGENCIES IN DM (KAD Dan HHS)Document26 pagesEMERGENCIES IN DM (KAD Dan HHS)ozNo ratings yet
- TCA Suppression and DM1Document22 pagesTCA Suppression and DM1Rubyrose TagumNo ratings yet
- Diabetic Ketoacidosis IntanDocument60 pagesDiabetic Ketoacidosis Intandesi susantiNo ratings yet
- Diabetes Case StudyDocument2 pagesDiabetes Case StudyRhina FutrellNo ratings yet
- Komplikasi Akut Pada DMDocument28 pagesKomplikasi Akut Pada DMmodrsbmNo ratings yet
- DKA, HHS, HYPOGLYCEMIA MKDocument42 pagesDKA, HHS, HYPOGLYCEMIA MKSol Gat ChupataNo ratings yet
- Diabetic Ketoacidosis (DKA) : Cindy, Chelsea, Kim, JessaDocument11 pagesDiabetic Ketoacidosis (DKA) : Cindy, Chelsea, Kim, JessaChelsea RuthrauffNo ratings yet
- Diabetes Mellitus: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaDocument46 pagesDiabetes Mellitus: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaAbdulkarim Mohamed AbdallaNo ratings yet
- Diabetic Emergencies and ManagementDocument41 pagesDiabetic Emergencies and ManagementNali peterNo ratings yet
- Diabetic Ketoacidosis: Presented by NG YHDocument32 pagesDiabetic Ketoacidosis: Presented by NG YHYuki NgNo ratings yet
- Diabetic Recipes for One and TwoFrom EverandDiabetic Recipes for One and TwoRating: 3 out of 5 stars3/5 (1)
- Low Blood Sugar: The Nutritional Plan to Overcome Hypoglycaemia, with 60 RecipesFrom EverandLow Blood Sugar: The Nutritional Plan to Overcome Hypoglycaemia, with 60 RecipesNo ratings yet
- Soluzioni al Diabete e all'Ipoglicemia - Come prevenire e disfarsene naturalmente e senza medicineFrom EverandSoluzioni al Diabete e all'Ipoglicemia - Come prevenire e disfarsene naturalmente e senza medicineNo ratings yet
- Eating Disorders: DR Jibril Handuleh Amoud UniversityDocument11 pagesEating Disorders: DR Jibril Handuleh Amoud UniversityOmar AbdillahiNo ratings yet
- Anxiety Disorders: DR Jibril Handuleh, MD MPHDocument39 pagesAnxiety Disorders: DR Jibril Handuleh, MD MPHOmar AbdillahiNo ratings yet
- Mood Disorders: DR Jibril Handuleh Amoud UniversityDocument73 pagesMood Disorders: DR Jibril Handuleh Amoud UniversityOmar AbdillahiNo ratings yet
- Psychiatric Signs and SymptomsDocument19 pagesPsychiatric Signs and SymptomsOmar Abdillahi100% (1)
- Psychiatry CourseDocument29 pagesPsychiatry CourseOmar AbdillahiNo ratings yet
- DVT and PeDocument25 pagesDVT and PeOmar AbdillahiNo ratings yet
- Hypertensive Emergency: Group ThreeDocument11 pagesHypertensive Emergency: Group ThreeOmar AbdillahiNo ratings yet
- Approach To Abdominal PainDocument22 pagesApproach To Abdominal PainOmar AbdillahiNo ratings yet
- ENDO... ElectrolyteDocument44 pagesENDO... ElectrolyteOmar AbdillahiNo ratings yet
- Chronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredDocument25 pagesChronic Obstructive Lung Disease (COPD) : Is An Obstructive Lung Diseases in Which Irreversible Lung Damage Has OccuredOmar AbdillahiNo ratings yet
- DVT and PeDocument25 pagesDVT and PeOmar AbdillahiNo ratings yet
- Acute Kidney Injury (AKI)Document50 pagesAcute Kidney Injury (AKI)Omar AbdillahiNo ratings yet
- السكر والبوتاسيومDocument2 pagesالسكر والبوتاسيومdr.Hamsa FaridNo ratings yet
- Working Your Way Through Adas t2d Treatment AlgorithmDocument61 pagesWorking Your Way Through Adas t2d Treatment AlgorithmNgọc BíchNo ratings yet
- Dietary Management of Diabetes Kelompok 4Document17 pagesDietary Management of Diabetes Kelompok 4NuhitaNo ratings yet
- Dapus AbrorDocument2 pagesDapus AbrorZulfitrawatiNo ratings yet
- Carla J. Greenbaum Leonard C. HarrisonDocument21 pagesCarla J. Greenbaum Leonard C. HarrisoncristinaiorgutNo ratings yet
- Type 2 Diabetes InfographicDocument1 pageType 2 Diabetes Infographicwwd2195No ratings yet
- Report 1690018110488Document2 pagesReport 1690018110488Krishna ChaitanyaNo ratings yet
- Drug StudyDocument4 pagesDrug StudyAilah Mae Dela Cruz0% (1)
- FOSSENCEDocument15 pagesFOSSENCEocombdNo ratings yet
- Occupational Management of Workers With Diabetes MellitusDocument11 pagesOccupational Management of Workers With Diabetes Mellitusari gunawanNo ratings yet
- General Principles of Insulin Therapy in Diabetes Mellitus - UpToDateDocument25 pagesGeneral Principles of Insulin Therapy in Diabetes Mellitus - UpToDateNeider 1111No ratings yet
- Insulin Pump - Google SearchDocument1 pageInsulin Pump - Google SearchMuhammad Irham syahNo ratings yet
- Teknik Penyuntikan Insulin ITCDocument14 pagesTeknik Penyuntikan Insulin ITCFina Ahmad FitrianaNo ratings yet
- Persuasive Essay CesDocument3 pagesPersuasive Essay Cesapi-273582752100% (1)
- Diabetic MedicationsDocument2 pagesDiabetic Medicationsapi-288062111No ratings yet
- Fasting in The Treatment of Diabetes and High Blood PressureDocument2 pagesFasting in The Treatment of Diabetes and High Blood PressureTrueNorth Health Center100% (1)
- L Tiple Choice Questions: Pyetje-Davidson'sDocument15 pagesL Tiple Choice Questions: Pyetje-Davidson'sNreca TokjonaNo ratings yet
- Gestational Diabetes MellitusDocument11 pagesGestational Diabetes Mellitusjohn jumborockNo ratings yet
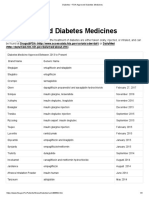
- Diabetes - FDA-Approved Diabetes MedicinesDocument3 pagesDiabetes - FDA-Approved Diabetes MedicinesArunNo ratings yet
- Clinical Practice Guidelines: Management of Type 2 Diabetes Mellitus (5 Edition) 2015Document13 pagesClinical Practice Guidelines: Management of Type 2 Diabetes Mellitus (5 Edition) 2015Azim Abd Razak100% (1)
- Drug Study of Antidiabetic DrugsDocument6 pagesDrug Study of Antidiabetic DrugsLorina Lynne ApelacioNo ratings yet
- 0507 Villela Diabetes Type 2Document59 pages0507 Villela Diabetes Type 2alex_christian1992No ratings yet
- Satuan Acara Penyuluhan Diabetes Melitus: Mata Kuliah: Keperawatan Komunitas IIDocument10 pagesSatuan Acara Penyuluhan Diabetes Melitus: Mata Kuliah: Keperawatan Komunitas IIJusmanNo ratings yet
- 01 Serpentina Presentation PDFDocument27 pages01 Serpentina Presentation PDFabcNo ratings yet
- Management of Diabetes Patients in SurgeryDocument28 pagesManagement of Diabetes Patients in Surgerylow_sernNo ratings yet
- Diabetes Management SystemDocument3 pagesDiabetes Management Systembeth2042No ratings yet
- Pathophysiology of Type II Diabetes MellitusDocument7 pagesPathophysiology of Type II Diabetes Mellituschinthaka18389021No ratings yet
- Know Your Numbers: Blood SugarDocument4 pagesKnow Your Numbers: Blood SugarMuhammad DaltonNo ratings yet