Download as pptx, pdf, or txt
You might also like
- امتحان مهم كاردياك سيرجاريDocument15 pagesامتحان مهم كاردياك سيرجاريIbrahim Barham50% (2)
- FCEM (SA) - Part - I - Past - Papers 1 PDFDocument2 pagesFCEM (SA) - Part - I - Past - Papers 1 PDFmatentenNo ratings yet
- EthambutolDocument1 pageEthambutolSibel ErtuğrulNo ratings yet
- 35.anti TB Drugs BDS 2021 For StudentsDocument8 pages35.anti TB Drugs BDS 2021 For StudentsireneNo ratings yet
- Lec 3 Anti Inflammatory DrugsDocument16 pagesLec 3 Anti Inflammatory DrugsXajepoxNo ratings yet
- The Immunosuppression 2021Document10 pagesThe Immunosuppression 2021Muhammad AliNo ratings yet
- Rheumatoid ArthritisDocument49 pagesRheumatoid ArthritisDr.U.P.Rathnakar.MD.DIH.PGDHM100% (4)
- Pharmaco Logy Imm Une Syste M Drugs: Julia Leonor Huaringa Lagomarsino, RN February 13, 2009Document12 pagesPharmaco Logy Imm Une Syste M Drugs: Julia Leonor Huaringa Lagomarsino, RN February 13, 2009julialeoNo ratings yet
- Tuberculosis TreatmentDocument44 pagesTuberculosis TreatmentAndie PerezNo ratings yet
- Drug Therapy of TB, 2015Document44 pagesDrug Therapy of TB, 2015FongChanyipNo ratings yet
- Unit-4 - PHARMACOLOGY IIIDocument37 pagesUnit-4 - PHARMACOLOGY IIIShantanu RewatkarNo ratings yet
- Antimicrobial Agents 2021Document82 pagesAntimicrobial Agents 2021Aprilene Angel Balaque ZunegaNo ratings yet
- 2020 Drugs On Pain (Analgesics) - DENTISTRYDocument28 pages2020 Drugs On Pain (Analgesics) - DENTISTRYVisayan Alliah GailNo ratings yet
- Teachng DemoDocument32 pagesTeachng DemoNom NomNo ratings yet
- Antimalarial Drugs: Presenter Basil Mupita Rgn/BscneDocument35 pagesAntimalarial Drugs: Presenter Basil Mupita Rgn/BscneTapiwaNo ratings yet
- CaptoprilDocument2 pagesCaptoprilVina Jane P Laurel100% (2)
- Anti Tubercular AgentsDocument22 pagesAnti Tubercular AgentsKakai Ablanque LopozNo ratings yet
- Gastrointestinal DrugDocument29 pagesGastrointestinal DrugJeneyse Ajap BalcenaNo ratings yet
- Anti-Tuberculosis DrugsDocument12 pagesAnti-Tuberculosis DrugsAkashNo ratings yet
- Additional Pharma CardsDocument21 pagesAdditional Pharma CardsBrilie Karl Viray100% (1)
- BPHM4149 - Chemotherapy-Induced Nausea Vomiting - 22jan2018Document42 pagesBPHM4149 - Chemotherapy-Induced Nausea Vomiting - 22jan2018kkyyyhNo ratings yet
- Drug - Nephrotoxicity - Dec - 2013.ppt FinalDocument27 pagesDrug - Nephrotoxicity - Dec - 2013.ppt FinalMaydhista PoetriNo ratings yet
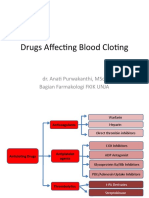
- Drugs Affecting Blood Cloting 2019Document39 pagesDrugs Affecting Blood Cloting 2019Mutiara RizkiNo ratings yet
- Non Steroid Antiinflammatory Drugs & Drugs Use in The Treatment of GoutDocument28 pagesNon Steroid Antiinflammatory Drugs & Drugs Use in The Treatment of GoutVevi VarcetyNo ratings yet
- Chemotherapeutic Agents CorrectedDocument66 pagesChemotherapeutic Agents CorrectedAlamgir Hossain ShemulNo ratings yet
- Prescribing in Patients With Liver Disease: Rakesh K TandonDocument4 pagesPrescribing in Patients With Liver Disease: Rakesh K Tandonjoydeep chakrabortyNo ratings yet
- DS - TB SeminarDocument68 pagesDS - TB SeminarpraveenNo ratings yet
- Antineoplastic AgentsDocument83 pagesAntineoplastic AgentsDwynwen Aleaume GumapacNo ratings yet
- Rational Use of AntibioticsDocument47 pagesRational Use of AntibioticsNurlela bustamNo ratings yet
- Week 9 - Course Task - Case Analysis Renal DisordersDocument4 pagesWeek 9 - Course Task - Case Analysis Renal DisordersJohnmarkLorenzanaRoveroNo ratings yet
- Rheumatology Diseases Group CDocument73 pagesRheumatology Diseases Group CDiana NurulNo ratings yet
- AminoglycosidesDocument20 pagesAminoglycosidesHassan.shehri100% (5)
- Antitubercular Drug: Dr. Deepak K GuptaDocument46 pagesAntitubercular Drug: Dr. Deepak K Guptasandeepv08No ratings yet
- DILIDocument40 pagesDILIYunik YuliapsariNo ratings yet
- DR TariqDocument43 pagesDR Tariqdrakram18No ratings yet
- Pulmonary Tuberculosis HanifDocument24 pagesPulmonary Tuberculosis HanifHanif GandohNo ratings yet
- Drug Study TBDocument5 pagesDrug Study TBSanvar Mal SoniNo ratings yet
- CCC GRP 6Document61 pagesCCC GRP 6Stacy JumaNo ratings yet
- Adverse Drug Reaction: Muhammad Faisal NadeemDocument65 pagesAdverse Drug Reaction: Muhammad Faisal NadeemfaisalnadeemNo ratings yet
- Rheumatoid Arthristis Tanghinan TombigaDocument19 pagesRheumatoid Arthristis Tanghinan TombigaDawn SanchezNo ratings yet
- M&N MGMTDocument3 pagesM&N MGMTMark Jefferson LunaNo ratings yet
- Tuberculosis: PGI: Mikhail Jude L. OpayDocument45 pagesTuberculosis: PGI: Mikhail Jude L. OpayMikkoOpayNo ratings yet
- Drug StudyDocument17 pagesDrug StudyAbigail BascoNo ratings yet
- Safety ReportingDocument13 pagesSafety ReportingAvinash AviNo ratings yet
- Nursing Pharmacology: Anti-Neoplastic Chemotherapeutic DrugsDocument42 pagesNursing Pharmacology: Anti-Neoplastic Chemotherapeutic DrugswokorowNo ratings yet
- Clinical Pharmacy The KidnyDocument34 pagesClinical Pharmacy The KidnyAta07No ratings yet
- Antiviral TherapyDocument19 pagesAntiviral TherapyMalueth AnguiNo ratings yet
- Camuso OtcDocument15 pagesCamuso Otcapi-548307464No ratings yet
- Lecture 22. Drugs Used in Renal and Urinary Tract DisordersDocument38 pagesLecture 22. Drugs Used in Renal and Urinary Tract DisorderskrisnadewirahadiNo ratings yet
- PyrazinamideDocument1 pagePyrazinamideMary-Lyne LausNo ratings yet
- Gastrointestinal and Gastrointestinal and Antiemetic Drugs Antiemetic DrugsDocument34 pagesGastrointestinal and Gastrointestinal and Antiemetic Drugs Antiemetic DrugsZakir UllahNo ratings yet
- LekemiaDocument9 pagesLekemiashamaamo19No ratings yet
- Cefixime: Suprax Class and CategoryDocument3 pagesCefixime: Suprax Class and CategoryArianne Joy SalvadorNo ratings yet
- Drug Induced Liver DiseaseDocument35 pagesDrug Induced Liver DiseaseKris Sharine Batalla OderoNo ratings yet
- Pharmacotherapy of TuberculosisDocument31 pagesPharmacotherapy of TuberculosisjabirNo ratings yet
- Antimetabolities: Route Onset Peak DurationDocument12 pagesAntimetabolities: Route Onset Peak DurationRichlle CortesNo ratings yet
- Antimycobacterials - ReyesDocument22 pagesAntimycobacterials - ReyesVivian CaballeroNo ratings yet
- Detection and Prevention of AKIDocument16 pagesDetection and Prevention of AKImjcatherine907No ratings yet
- XIV. Antimicrobial Drugs (D, E, F, G), ZI-WA, AY18-19Document64 pagesXIV. Antimicrobial Drugs (D, E, F, G), ZI-WA, AY18-19Hala Al-siyabiNo ratings yet
- Aplastic Anemia Drug Drug Category Mechanism of ActionDocument21 pagesAplastic Anemia Drug Drug Category Mechanism of ActionRea Dominique CabanillaNo ratings yet
- Lecture 16 AntimycobacterialsDocument43 pagesLecture 16 Antimycobacterialssaqlain18148No ratings yet
- The Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesFrom EverandThe Perfect Neutropenic Diet Cookbook; The Complete Nutrition Guide To Reinstating Overall Health For General Wellness With Delectable And Nourishing RecipesNo ratings yet
- Anemias RBC Morphology Approach To DiagnosisDocument24 pagesAnemias RBC Morphology Approach To DiagnosisAyessa VillacorteNo ratings yet
- Conversion DisorderDocument49 pagesConversion DisorderSonali SawaleNo ratings yet
- Pharyngitis: Approach To Diagnosis and TreatmentDocument7 pagesPharyngitis: Approach To Diagnosis and TreatmentVio LatteireNo ratings yet
- Legal Medicine 2020 2021Document4 pagesLegal Medicine 2020 2021Zie DammiNo ratings yet
- Micropara LabDocument8 pagesMicropara LabFatima KateNo ratings yet
- Steroid Injections: Read This If You Are Planning On Having A Steroid InjectionDocument3 pagesSteroid Injections: Read This If You Are Planning On Having A Steroid InjectionyudhaNo ratings yet
- Iso 13485 Iso 9001Document56 pagesIso 13485 Iso 9001Juliamm MartNo ratings yet
- Meeting Briefing DocumentDocument53 pagesMeeting Briefing DocumentErin O'BrienNo ratings yet
- Evaluasi Penatalaksanaan Irigasi Kandung Kemih Karena Retensi Bekuan Darah Pada Pasien Gangguan Perkemihan: Systematic ReviewDocument13 pagesEvaluasi Penatalaksanaan Irigasi Kandung Kemih Karena Retensi Bekuan Darah Pada Pasien Gangguan Perkemihan: Systematic ReviewMuhammad Fajrul Falah KholifaturrahmanNo ratings yet
- Factors Affecting Intestinal Health in PoultryDocument12 pagesFactors Affecting Intestinal Health in PoultryRezaNo ratings yet
- Midwifery CareDocument15 pagesMidwifery CarefinaNo ratings yet
- Oxygen ToxicityDocument4 pagesOxygen ToxicityRicard ClainkweeNo ratings yet
- Jurnal Anemia Bahasa InggrisDocument9 pagesJurnal Anemia Bahasa InggrisonyourmargotNo ratings yet
- Allergic RhinitisDocument10 pagesAllergic Rhinitisanamuj8No ratings yet
- Nexus ConnectionsDocument2 pagesNexus ConnectionsBarry RoginskiNo ratings yet
- Community-Acquired Pneumonia in Children: Clinical Features and Diagnosis - UpToDateDocument62 pagesCommunity-Acquired Pneumonia in Children: Clinical Features and Diagnosis - UpToDateYeidhy Karin Cayo CoñezNo ratings yet
- PhysioEx Exercise 4 Activity 4 - Balamad, Maria Karla M.Document3 pagesPhysioEx Exercise 4 Activity 4 - Balamad, Maria Karla M.Maria Karla BalamadNo ratings yet
- Protect What You Treasure Most: HealthDocument7 pagesProtect What You Treasure Most: HealthNelly HNo ratings yet
- Textbook Ebook Diagnostic Ultrasound For Sonographers Aya Kamaya All Chapter PDFDocument43 pagesTextbook Ebook Diagnostic Ultrasound For Sonographers Aya Kamaya All Chapter PDFolivia.anderson705100% (9)
- Idiopathic Linear Leukoplakia of Gingiva: A Rare Case ReportDocument3 pagesIdiopathic Linear Leukoplakia of Gingiva: A Rare Case ReportDeasireeNo ratings yet
- Wound InfectionDocument30 pagesWound InfectionIbrahim SultanNo ratings yet
- ABLE - NUS IRB Information Sheet and Consent-081222Document20 pagesABLE - NUS IRB Information Sheet and Consent-081222yu enNo ratings yet
- Cauti Prevention Qi ProjectDocument9 pagesCauti Prevention Qi Projectapi-596656815No ratings yet
- Stool Specimen CollectionDocument8 pagesStool Specimen CollectionPraveen KumarNo ratings yet
- The Plague of Athens and The Cult of Asclepius: A Case Study of Collective Behavior and A Social MovementDocument7 pagesThe Plague of Athens and The Cult of Asclepius: A Case Study of Collective Behavior and A Social MovementSamuel JeffriesNo ratings yet
- Diagnosis and Management of Ureteric Injury: An Evidence-Based AnalysisDocument13 pagesDiagnosis and Management of Ureteric Injury: An Evidence-Based AnalysisqalbiNo ratings yet
- Consolidated Guidelines OnDocument594 pagesConsolidated Guidelines OnRICHARD EDUARDO FERNANDEZ SAENZNo ratings yet
- Developmental Dysplasia of The HipDocument331 pagesDevelopmental Dysplasia of The HipIHDIonline100% (14)