
Corynebacterium and Listeria
Corynebacterium and Listeria
You might also like
- Sale Contract (Sample)Document4 pagesSale Contract (Sample)Hoàng Nam29No ratings yet
- Microbial Disease of The Nervous SystemDocument41 pagesMicrobial Disease of The Nervous SystemPreciousNo ratings yet
- TetanusDocument32 pagesTetanusVinotheran MichaelNo ratings yet
- The Immunology of Human ReproductionDocument171 pagesThe Immunology of Human ReproductionEkanita Desiani100% (1)
- FB70 Customer InvoiceDocument21 pagesFB70 Customer Invoiceksravi0% (1)
- ClostridiumDocument20 pagesClostridiumNuura jeylani KasimNo ratings yet
- 1.4 - ClostridiumDocument45 pages1.4 - Clostridiumsajad abasNo ratings yet
- Meningitis in Children 2008: Sileshi Mulatu (BSC N, MSC N)Document81 pagesMeningitis in Children 2008: Sileshi Mulatu (BSC N, MSC N)yohanes100% (1)
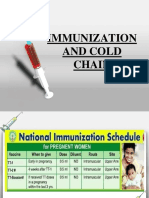
- Immunization and Cold ChainDocument26 pagesImmunization and Cold ChainnNo ratings yet
- UW Infectious Diseases + Microbiology Educational Objectives PDFDocument75 pagesUW Infectious Diseases + Microbiology Educational Objectives PDFDrbee10No ratings yet
- PSM Exam NotesDocument250 pagesPSM Exam Notesjf65ky8f8tNo ratings yet
- Lec4 Clostridium 2Document6 pagesLec4 Clostridium 2hindaoda90100% (1)
- DPT Hib 2015Document42 pagesDPT Hib 2015Hannan AliNo ratings yet
- White Blood Cells and The Immune ResponseDocument22 pagesWhite Blood Cells and The Immune ResponsehhhhhhhhhhhhhhNo ratings yet
- Lecture 1Document52 pagesLecture 1Emmanuel Thon MadingNo ratings yet
- General Anatomy of The Immune SystemDocument29 pagesGeneral Anatomy of The Immune Systemrambabs369100% (2)
- Types of VaccinesDocument21 pagesTypes of VaccinesAtoillah IsvandiaryNo ratings yet
- 099 - VaccinesDocument4 pages099 - VaccinesArjan LallNo ratings yet
- Aerobes Chapter 12Document6 pagesAerobes Chapter 12Kristine BoholstNo ratings yet
- B. AnthracisDocument14 pagesB. AnthracisSahil KumarNo ratings yet
- MMG 301 Lec. 32 Bacterial Infections Questions For TodayDocument13 pagesMMG 301 Lec. 32 Bacterial Infections Questions For TodayActress VeriyanNo ratings yet
- Immunology Notes WJEC 2022 SLJ 3Document37 pagesImmunology Notes WJEC 2022 SLJ 3zainpaNo ratings yet
- My Co BacteriaDocument20 pagesMy Co BacteriaAnzo SimonNo ratings yet
- C. Tetani FinalDocument3 pagesC. Tetani FinalSajjad Hossain ShuvoNo ratings yet
- Vaccine: - Chhabi Acharya Binod Rasaili Rupesh K.C Hope Int'l CollegeDocument21 pagesVaccine: - Chhabi Acharya Binod Rasaili Rupesh K.C Hope Int'l CollegeScott Domes100% (1)
- The Clostridium Specis.Document38 pagesThe Clostridium Specis.علي عبد الكريم عاصيNo ratings yet
- Biologics: by DR TanginaDocument41 pagesBiologics: by DR TanginaAnam AbidNo ratings yet
- By: Catherine M. Souribio, R.NDocument40 pagesBy: Catherine M. Souribio, R.NIsrael AgrisNo ratings yet
- Immunitization and VaccinationDocument46 pagesImmunitization and VaccinationMazhar RehmanNo ratings yet
- Public Health Officers C1: TetanusDocument64 pagesPublic Health Officers C1: Tetanusmamaru bantieNo ratings yet
- Binder 1Document29 pagesBinder 1Narasimha MurthyNo ratings yet
- Vaccine Chapter-4Document64 pagesVaccine Chapter-4jihovajayraNo ratings yet
- Bilal Hassan M.Phil. PharmaceuticsDocument49 pagesBilal Hassan M.Phil. PharmaceuticsMoazama FayyazNo ratings yet
- VaccinationDocument35 pagesVaccinationmuneebazmat1123No ratings yet
- Bacillus PDFDocument28 pagesBacillus PDFMustafa SaßerNo ratings yet
- Morphology & Identification: Clostridium SpeciesDocument14 pagesMorphology & Identification: Clostridium Specieshussain AltaherNo ratings yet
- Bacterial VacciensDocument18 pagesBacterial VacciensSamNo ratings yet
- Abdelfattah Monged Selim - Tetanus 2Document25 pagesAbdelfattah Monged Selim - Tetanus 2Saja MaraqaNo ratings yet
- Why Do We Have An Immune System?Document4 pagesWhy Do We Have An Immune System?Rumaisa ChowdhuryNo ratings yet
- Short Intro To Micro BioDocument9 pagesShort Intro To Micro BioJun Kaizer Arabaca MuycoNo ratings yet
- VaccinesDocument17 pagesVaccinesYOGANANTH mscasNo ratings yet
- Basic Principles of Immunology and Immune SystemsDocument18 pagesBasic Principles of Immunology and Immune SystemsVictoria &BeautifulPeopleNo ratings yet
- Topic 10. Diseases and ImmunityDocument53 pagesTopic 10. Diseases and ImmunityC BNo ratings yet
- ImmunologyDocument36 pagesImmunologyمروه عماد عيسى100% (1)
- 13 ImmunizationDocument18 pages13 ImmunizationMunazzaNo ratings yet
- The Immune SystemDocument4 pagesThe Immune SystemSseguya Lubega YaqubNo ratings yet
- Listeria Monocytogenes: Case Study 2009Document22 pagesListeria Monocytogenes: Case Study 2009Glenn Asuncion PagaduanNo ratings yet
- Ing GrisDocument20 pagesIng GrisAlvianita PutriNo ratings yet
- The Immune SystemDocument49 pagesThe Immune SystemUmer YasirNo ratings yet
- CORYNEBACTERIUMDocument22 pagesCORYNEBACTERIUMHamidreza RahmaniNo ratings yet
- IGCSE BIOLOGY: Disease & ImmunityDocument40 pagesIGCSE BIOLOGY: Disease & ImmunityAliya ShukriNo ratings yet
- Innate ImmunityDocument32 pagesInnate ImmunityYik sNo ratings yet
- Vaccines1 03Document41 pagesVaccines1 03Aasim HabibNo ratings yet
- Topic 4 - Immune SystemDocument5 pagesTopic 4 - Immune SystemYara Jeah Ingay BaliliNo ratings yet
- Presentation 1Document49 pagesPresentation 1Dessie DessieNo ratings yet
- Disease and Immunity 22-23Document6 pagesDisease and Immunity 22-23hiNo ratings yet
- Ch-10 Diseases and ImmunityDocument17 pagesCh-10 Diseases and ImmunityHaziq Khan100% (1)
- Biofilm: DR JyotiDocument34 pagesBiofilm: DR Jyotimadhumitha srinivasNo ratings yet
- DiphtheriaDocument25 pagesDiphtheriaRohan TejaNo ratings yet
- Meningitis Final VersionDocument28 pagesMeningitis Final Versiontooba hussainNo ratings yet
- Non-inflammatory immunology: An introduction to the immune system and its pathologiesFrom EverandNon-inflammatory immunology: An introduction to the immune system and its pathologiesNo ratings yet
- Vaccination: How Millions of Lives Have Been Saved - Perhaps YoursFrom EverandVaccination: How Millions of Lives Have Been Saved - Perhaps YoursNo ratings yet
- A Possible Framework For Your WorkDocument2 pagesA Possible Framework For Your Workkn7m2dnwvkNo ratings yet
- Sigmund Freud: Psychosexual DevelopmentDocument6 pagesSigmund Freud: Psychosexual DevelopmentKarlo Gil ConcepcionNo ratings yet
- Achieving Marketing Success in A Cookieless WorldDocument16 pagesAchieving Marketing Success in A Cookieless WorldKim HoldenNo ratings yet
- Efe Unit 1 MergedDocument210 pagesEfe Unit 1 MergedSiddhant SinghaniaNo ratings yet
- Wilbur Smith Books: Yea R Title Timeframe SeriesDocument3 pagesWilbur Smith Books: Yea R Title Timeframe SeriesAamirShabbir100% (2)
- Math 1050 Mortgage ProjectDocument5 pagesMath 1050 Mortgage Projectapi-2740249620% (1)
- Lower Division ClerkDocument5 pagesLower Division Clerkkola0123No ratings yet
- Price List: Airconditioning SystemsDocument72 pagesPrice List: Airconditioning Systemsbstan_1No ratings yet
- Case Digests of Selected Ponencias of Justice Caguioa Updated 10.12.22Document184 pagesCase Digests of Selected Ponencias of Justice Caguioa Updated 10.12.22Gee BerdinNo ratings yet
- The Pagan ChristDocument42 pagesThe Pagan ChristJason LambNo ratings yet
- President CEO COO EVP Construction in Boca Raton FL Resume Martin DriscollDocument2 pagesPresident CEO COO EVP Construction in Boca Raton FL Resume Martin DriscollMartinDriscollNo ratings yet
- Student ResumeDocument8 pagesStudent Resumegt2bxphv100% (1)
- Instrumental CausalityDocument14 pagesInstrumental Causalitysbob255No ratings yet
- Difference B/W Financial Creditor and Operational Creditor Under IBC, 2016Document5 pagesDifference B/W Financial Creditor and Operational Creditor Under IBC, 2016Ezhil KaviyaNo ratings yet
- Auditing Problems You Can UseDocument51 pagesAuditing Problems You Can UseChinita VirayNo ratings yet
- Managing Diversity Toward A Globally Inclusive Workplace 4Th Edition Barak Test Bank Full Chapter PDFDocument36 pagesManaging Diversity Toward A Globally Inclusive Workplace 4Th Edition Barak Test Bank Full Chapter PDFphanagneslr9h55100% (15)
- Champion (2000) - American Women Writers PDFDocument422 pagesChampion (2000) - American Women Writers PDFfernanda100% (1)
- Family Office Vs Private BanksDocument59 pagesFamily Office Vs Private Banksdsrkim100% (3)
- CIF - Aedit AbdullahDocument21 pagesCIF - Aedit Abdullahjason maoNo ratings yet
- Ex Nihilo CreationDocument3 pagesEx Nihilo CreationAnonymous b7ccvQSQpNo ratings yet
- ATP 108 Commercial Transactions Course Outline 2023 - 2024Document5 pagesATP 108 Commercial Transactions Course Outline 2023 - 2024Topz TrendzNo ratings yet
- Constituencies of CRMDocument3 pagesConstituencies of CRMnikitha sNo ratings yet
- Percieved Social Media Influence On The Choice of National Candidates in 2022 Philippine Elections Senior High School StudentsDocument25 pagesPercieved Social Media Influence On The Choice of National Candidates in 2022 Philippine Elections Senior High School StudentsDan Gela Mæ MaYoNo ratings yet
- Project Proposals AWAIS FAYAZDocument6 pagesProject Proposals AWAIS FAYAZaashhadaliiNo ratings yet
- DRK New GamesDocument17 pagesDRK New Gamesala eddine henchiriNo ratings yet
- Crimes (Sentencing Procedure) Act 1999 No 92 Section 21ADocument4 pagesCrimes (Sentencing Procedure) Act 1999 No 92 Section 21AReza PatriaNo ratings yet
- Impact of Dividend Policy On Share PricesDocument16 pagesImpact of Dividend Policy On Share PricesAli JarralNo ratings yet
- 5 Reasons Why Self-Awareness Is ImportantDocument1 page5 Reasons Why Self-Awareness Is Importantkate doNo ratings yet























































































Download as pptx, pdf, or txt
You might also like
- Sale Contract (Sample)Document4 pagesSale Contract (Sample)Hoàng Nam29No ratings yet
- Microbial Disease of The Nervous SystemDocument41 pagesMicrobial Disease of The Nervous SystemPreciousNo ratings yet
- TetanusDocument32 pagesTetanusVinotheran MichaelNo ratings yet
- The Immunology of Human ReproductionDocument171 pagesThe Immunology of Human ReproductionEkanita Desiani100% (1)
- FB70 Customer InvoiceDocument21 pagesFB70 Customer Invoiceksravi0% (1)
- ClostridiumDocument20 pagesClostridiumNuura jeylani KasimNo ratings yet
- 1.4 - ClostridiumDocument45 pages1.4 - Clostridiumsajad abasNo ratings yet
- Meningitis in Children 2008: Sileshi Mulatu (BSC N, MSC N)Document81 pagesMeningitis in Children 2008: Sileshi Mulatu (BSC N, MSC N)yohanes100% (1)
- Immunization and Cold ChainDocument26 pagesImmunization and Cold ChainnNo ratings yet
- UW Infectious Diseases + Microbiology Educational Objectives PDFDocument75 pagesUW Infectious Diseases + Microbiology Educational Objectives PDFDrbee10No ratings yet
- PSM Exam NotesDocument250 pagesPSM Exam Notesjf65ky8f8tNo ratings yet
- Lec4 Clostridium 2Document6 pagesLec4 Clostridium 2hindaoda90100% (1)
- DPT Hib 2015Document42 pagesDPT Hib 2015Hannan AliNo ratings yet
- White Blood Cells and The Immune ResponseDocument22 pagesWhite Blood Cells and The Immune ResponsehhhhhhhhhhhhhhNo ratings yet
- Lecture 1Document52 pagesLecture 1Emmanuel Thon MadingNo ratings yet
- General Anatomy of The Immune SystemDocument29 pagesGeneral Anatomy of The Immune Systemrambabs369100% (2)
- Types of VaccinesDocument21 pagesTypes of VaccinesAtoillah IsvandiaryNo ratings yet
- 099 - VaccinesDocument4 pages099 - VaccinesArjan LallNo ratings yet
- Aerobes Chapter 12Document6 pagesAerobes Chapter 12Kristine BoholstNo ratings yet
- B. AnthracisDocument14 pagesB. AnthracisSahil KumarNo ratings yet
- MMG 301 Lec. 32 Bacterial Infections Questions For TodayDocument13 pagesMMG 301 Lec. 32 Bacterial Infections Questions For TodayActress VeriyanNo ratings yet
- Immunology Notes WJEC 2022 SLJ 3Document37 pagesImmunology Notes WJEC 2022 SLJ 3zainpaNo ratings yet
- My Co BacteriaDocument20 pagesMy Co BacteriaAnzo SimonNo ratings yet
- C. Tetani FinalDocument3 pagesC. Tetani FinalSajjad Hossain ShuvoNo ratings yet
- Vaccine: - Chhabi Acharya Binod Rasaili Rupesh K.C Hope Int'l CollegeDocument21 pagesVaccine: - Chhabi Acharya Binod Rasaili Rupesh K.C Hope Int'l CollegeScott Domes100% (1)
- The Clostridium Specis.Document38 pagesThe Clostridium Specis.علي عبد الكريم عاصيNo ratings yet
- Biologics: by DR TanginaDocument41 pagesBiologics: by DR TanginaAnam AbidNo ratings yet
- By: Catherine M. Souribio, R.NDocument40 pagesBy: Catherine M. Souribio, R.NIsrael AgrisNo ratings yet
- Immunitization and VaccinationDocument46 pagesImmunitization and VaccinationMazhar RehmanNo ratings yet
- Public Health Officers C1: TetanusDocument64 pagesPublic Health Officers C1: Tetanusmamaru bantieNo ratings yet
- Binder 1Document29 pagesBinder 1Narasimha MurthyNo ratings yet
- Vaccine Chapter-4Document64 pagesVaccine Chapter-4jihovajayraNo ratings yet
- Bilal Hassan M.Phil. PharmaceuticsDocument49 pagesBilal Hassan M.Phil. PharmaceuticsMoazama FayyazNo ratings yet
- VaccinationDocument35 pagesVaccinationmuneebazmat1123No ratings yet
- Bacillus PDFDocument28 pagesBacillus PDFMustafa SaßerNo ratings yet
- Morphology & Identification: Clostridium SpeciesDocument14 pagesMorphology & Identification: Clostridium Specieshussain AltaherNo ratings yet
- Bacterial VacciensDocument18 pagesBacterial VacciensSamNo ratings yet
- Abdelfattah Monged Selim - Tetanus 2Document25 pagesAbdelfattah Monged Selim - Tetanus 2Saja MaraqaNo ratings yet
- Why Do We Have An Immune System?Document4 pagesWhy Do We Have An Immune System?Rumaisa ChowdhuryNo ratings yet
- Short Intro To Micro BioDocument9 pagesShort Intro To Micro BioJun Kaizer Arabaca MuycoNo ratings yet
- VaccinesDocument17 pagesVaccinesYOGANANTH mscasNo ratings yet
- Basic Principles of Immunology and Immune SystemsDocument18 pagesBasic Principles of Immunology and Immune SystemsVictoria &BeautifulPeopleNo ratings yet
- Topic 10. Diseases and ImmunityDocument53 pagesTopic 10. Diseases and ImmunityC BNo ratings yet
- ImmunologyDocument36 pagesImmunologyمروه عماد عيسى100% (1)
- 13 ImmunizationDocument18 pages13 ImmunizationMunazzaNo ratings yet
- The Immune SystemDocument4 pagesThe Immune SystemSseguya Lubega YaqubNo ratings yet
- Listeria Monocytogenes: Case Study 2009Document22 pagesListeria Monocytogenes: Case Study 2009Glenn Asuncion PagaduanNo ratings yet
- Ing GrisDocument20 pagesIng GrisAlvianita PutriNo ratings yet
- The Immune SystemDocument49 pagesThe Immune SystemUmer YasirNo ratings yet
- CORYNEBACTERIUMDocument22 pagesCORYNEBACTERIUMHamidreza RahmaniNo ratings yet
- IGCSE BIOLOGY: Disease & ImmunityDocument40 pagesIGCSE BIOLOGY: Disease & ImmunityAliya ShukriNo ratings yet
- Innate ImmunityDocument32 pagesInnate ImmunityYik sNo ratings yet
- Vaccines1 03Document41 pagesVaccines1 03Aasim HabibNo ratings yet
- Topic 4 - Immune SystemDocument5 pagesTopic 4 - Immune SystemYara Jeah Ingay BaliliNo ratings yet
- Presentation 1Document49 pagesPresentation 1Dessie DessieNo ratings yet
- Disease and Immunity 22-23Document6 pagesDisease and Immunity 22-23hiNo ratings yet
- Ch-10 Diseases and ImmunityDocument17 pagesCh-10 Diseases and ImmunityHaziq Khan100% (1)
- Biofilm: DR JyotiDocument34 pagesBiofilm: DR Jyotimadhumitha srinivasNo ratings yet
- DiphtheriaDocument25 pagesDiphtheriaRohan TejaNo ratings yet
- Meningitis Final VersionDocument28 pagesMeningitis Final Versiontooba hussainNo ratings yet
- Non-inflammatory immunology: An introduction to the immune system and its pathologiesFrom EverandNon-inflammatory immunology: An introduction to the immune system and its pathologiesNo ratings yet
- Vaccination: How Millions of Lives Have Been Saved - Perhaps YoursFrom EverandVaccination: How Millions of Lives Have Been Saved - Perhaps YoursNo ratings yet
- A Possible Framework For Your WorkDocument2 pagesA Possible Framework For Your Workkn7m2dnwvkNo ratings yet
- Sigmund Freud: Psychosexual DevelopmentDocument6 pagesSigmund Freud: Psychosexual DevelopmentKarlo Gil ConcepcionNo ratings yet
- Achieving Marketing Success in A Cookieless WorldDocument16 pagesAchieving Marketing Success in A Cookieless WorldKim HoldenNo ratings yet
- Efe Unit 1 MergedDocument210 pagesEfe Unit 1 MergedSiddhant SinghaniaNo ratings yet
- Wilbur Smith Books: Yea R Title Timeframe SeriesDocument3 pagesWilbur Smith Books: Yea R Title Timeframe SeriesAamirShabbir100% (2)
- Math 1050 Mortgage ProjectDocument5 pagesMath 1050 Mortgage Projectapi-2740249620% (1)
- Lower Division ClerkDocument5 pagesLower Division Clerkkola0123No ratings yet
- Price List: Airconditioning SystemsDocument72 pagesPrice List: Airconditioning Systemsbstan_1No ratings yet
- Case Digests of Selected Ponencias of Justice Caguioa Updated 10.12.22Document184 pagesCase Digests of Selected Ponencias of Justice Caguioa Updated 10.12.22Gee BerdinNo ratings yet
- The Pagan ChristDocument42 pagesThe Pagan ChristJason LambNo ratings yet
- President CEO COO EVP Construction in Boca Raton FL Resume Martin DriscollDocument2 pagesPresident CEO COO EVP Construction in Boca Raton FL Resume Martin DriscollMartinDriscollNo ratings yet
- Student ResumeDocument8 pagesStudent Resumegt2bxphv100% (1)
- Instrumental CausalityDocument14 pagesInstrumental Causalitysbob255No ratings yet
- Difference B/W Financial Creditor and Operational Creditor Under IBC, 2016Document5 pagesDifference B/W Financial Creditor and Operational Creditor Under IBC, 2016Ezhil KaviyaNo ratings yet
- Auditing Problems You Can UseDocument51 pagesAuditing Problems You Can UseChinita VirayNo ratings yet
- Managing Diversity Toward A Globally Inclusive Workplace 4Th Edition Barak Test Bank Full Chapter PDFDocument36 pagesManaging Diversity Toward A Globally Inclusive Workplace 4Th Edition Barak Test Bank Full Chapter PDFphanagneslr9h55100% (15)
- Champion (2000) - American Women Writers PDFDocument422 pagesChampion (2000) - American Women Writers PDFfernanda100% (1)
- Family Office Vs Private BanksDocument59 pagesFamily Office Vs Private Banksdsrkim100% (3)
- CIF - Aedit AbdullahDocument21 pagesCIF - Aedit Abdullahjason maoNo ratings yet
- Ex Nihilo CreationDocument3 pagesEx Nihilo CreationAnonymous b7ccvQSQpNo ratings yet
- ATP 108 Commercial Transactions Course Outline 2023 - 2024Document5 pagesATP 108 Commercial Transactions Course Outline 2023 - 2024Topz TrendzNo ratings yet
- Constituencies of CRMDocument3 pagesConstituencies of CRMnikitha sNo ratings yet
- Percieved Social Media Influence On The Choice of National Candidates in 2022 Philippine Elections Senior High School StudentsDocument25 pagesPercieved Social Media Influence On The Choice of National Candidates in 2022 Philippine Elections Senior High School StudentsDan Gela Mæ MaYoNo ratings yet
- Project Proposals AWAIS FAYAZDocument6 pagesProject Proposals AWAIS FAYAZaashhadaliiNo ratings yet
- DRK New GamesDocument17 pagesDRK New Gamesala eddine henchiriNo ratings yet
- Crimes (Sentencing Procedure) Act 1999 No 92 Section 21ADocument4 pagesCrimes (Sentencing Procedure) Act 1999 No 92 Section 21AReza PatriaNo ratings yet
- Impact of Dividend Policy On Share PricesDocument16 pagesImpact of Dividend Policy On Share PricesAli JarralNo ratings yet
- 5 Reasons Why Self-Awareness Is ImportantDocument1 page5 Reasons Why Self-Awareness Is Importantkate doNo ratings yet