Download as pptx, pdf, or txt
You might also like
- Exercise in The Prevention and Treatment of Type 2 Diabetes: Didactic SynopsisDocument27 pagesExercise in The Prevention and Treatment of Type 2 Diabetes: Didactic SynopsisLic. Monica Bamonde NutricionistaNo ratings yet
- Fluids and Electrolytes Pathophysiology NursingDocument16 pagesFluids and Electrolytes Pathophysiology Nursinggrad_nurse_2015100% (3)
- Laporan Kasus KADDocument43 pagesLaporan Kasus KADharasthaNo ratings yet
- Terapi Cairan: Dr. M Zulkarnain B Mked (An), SpanDocument70 pagesTerapi Cairan: Dr. M Zulkarnain B Mked (An), SpanMerdianing Ika MahendraNo ratings yet
- 1 Fluid and ElectrolyteDocument51 pages1 Fluid and ElectrolyteSanjiv SharmaNo ratings yet
- Terapi Cairan Pada AnakDocument48 pagesTerapi Cairan Pada AnakAstri Novia RizqiNo ratings yet
- 1 Fluid and ElectrolyteDocument51 pages1 Fluid and ElectrolyteSanjiv SharmaNo ratings yet
- Body Fluid Compartment SlidesDocument18 pagesBody Fluid Compartment SlidesAkanbi FavourNo ratings yet
- Balance Cairan Final.Document41 pagesBalance Cairan Final.Niqko Bayu PrakarsaNo ratings yet
- Aspect To Consider in Fluid TherapyDocument34 pagesAspect To Consider in Fluid TherapyhanifahNo ratings yet
- Fluids and ElectrolytesDocument70 pagesFluids and ElectrolytesCesar MellaNo ratings yet
- Potassium Metabolism MainDocument59 pagesPotassium Metabolism MainPrincewill SeiyefaNo ratings yet
- Morning ReportDocument22 pagesMorning ReportNiinna AwliaNo ratings yet
- TutorialDocument29 pagesTutorialVilza maharaniNo ratings yet
- Management Terapi CairanDocument60 pagesManagement Terapi CairanHayat Hamzah DawiNo ratings yet
- Physiology of Body FluidsDocument23 pagesPhysiology of Body FluidsRamadan Physiology100% (1)
- Fluid & Electrolytes SaurabhDocument88 pagesFluid & Electrolytes Saurabhunknownsince1986No ratings yet
- Fluid Acid CaseDocument29 pagesFluid Acid CaseOviNo ratings yet
- Gangguan Keseimbangan Cairan Dan ElektrolitDocument45 pagesGangguan Keseimbangan Cairan Dan Elektrolitmulyo utomoNo ratings yet
- Intravenous Fluids: Composition & UsesDocument41 pagesIntravenous Fluids: Composition & UsesFathima BanuzNo ratings yet
- Perioperative Fluid ManagementDocument27 pagesPerioperative Fluid ManagementridhoardiNo ratings yet
- Cairan Biologi: I Gaa. SuartiniDocument52 pagesCairan Biologi: I Gaa. SuartiniAlif Ilham100% (1)
- Body FluidsDocument44 pagesBody FluidsTriza JeremiahNo ratings yet
- 3.body FluidsDocument57 pages3.body Fluids234820No ratings yet
- Kuliah Infant Periopeative FluidDocument27 pagesKuliah Infant Periopeative FluidMohammad SutamiNo ratings yet
- RH3 CairanDocument19 pagesRH3 CairanRifqiEkaBudiantaNo ratings yet
- Chapter 3. Preoperative Consideration of The Surgical PatientDocument2 pagesChapter 3. Preoperative Consideration of The Surgical PatientDumapis RichardNo ratings yet
- Fluid Therapy (Ali Haedar)Document25 pagesFluid Therapy (Ali Haedar)Atika LuqyanaNo ratings yet
- Terapi Cairain Dan ElektrolitDocument39 pagesTerapi Cairain Dan ElektrolityulyaNo ratings yet
- Management Terapi CairanDocument60 pagesManagement Terapi Cairanpeter singalNo ratings yet
- FluidDocument31 pagesFluidZainab BasimNo ratings yet
- Fluid and ElectrolytesDocument23 pagesFluid and ElectrolytesNanaNo ratings yet
- Fluid TherapyDocument25 pagesFluid TherapyHafidz YahyaNo ratings yet
- DR - Sabah Noori 1Document26 pagesDR - Sabah Noori 1Mighty AbodyNo ratings yet
- Body FluidsDocument34 pagesBody Fluidsdkphyhd99fNo ratings yet
- Body Fluids: DR Sheetal C NDocument34 pagesBody Fluids: DR Sheetal C Nmus zaharaNo ratings yet
- Roumilla Mendoza, M.D. Roumilla Mendoza, M.D. Pediatric Gastroenterologist Pediatric GastroenterologistDocument59 pagesRoumilla Mendoza, M.D. Roumilla Mendoza, M.D. Pediatric Gastroenterologist Pediatric GastroenterologistYenyen DelgadoNo ratings yet
- Dasar - Dasar Terapi: Cairan Dan ElektrolitDocument60 pagesDasar - Dasar Terapi: Cairan Dan ElektrolitdedeNo ratings yet
- Fluid & Electrolyte ImbalancesDocument212 pagesFluid & Electrolyte ImbalancesLane Mae Magpatoc NoerrotNo ratings yet
- Body Fluids and ElectrolytesDocument42 pagesBody Fluids and ElectrolytesQusaiBadr100% (1)
- Tatalaksana Syok Hipovolemik & HipoglikemiaDocument40 pagesTatalaksana Syok Hipovolemik & HipoglikemiaMuhammad Daviq0% (1)
- Dokumen - Tips Fluid and Electrolyte Therapy Vydehi Institute of If Ecfv Falls 1 byDocument56 pagesDokumen - Tips Fluid and Electrolyte Therapy Vydehi Institute of If Ecfv Falls 1 bykuruva gayathriNo ratings yet
- Body FluidsDocument46 pagesBody FluidsSidharth BhardwajNo ratings yet
- Fisiologi Sel Dan Cairan Tubuh: M.Ihwan KusumaDocument20 pagesFisiologi Sel Dan Cairan Tubuh: M.Ihwan KusumaHenny AprianiNo ratings yet
- Fluid & Electrolytes - LebbieDocument109 pagesFluid & Electrolytes - LebbieMohamed KamaraNo ratings yet
- Body Fluids and Blood - HUMAN PHYSIOLOGYDocument29 pagesBody Fluids and Blood - HUMAN PHYSIOLOGYSodeinde SimeonNo ratings yet
- Morning ReportDocument27 pagesMorning ReportDody PrasetyaNo ratings yet
- IMBALANCE ofDocument21 pagesIMBALANCE ofapi-19916399No ratings yet
- Body Fluid CompartmenBDSDocument17 pagesBody Fluid CompartmenBDSHimani JhaNo ratings yet
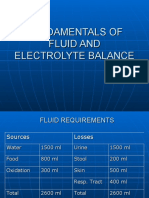
- Fundamentals of Fluid and Electrolyte BalanceDocument46 pagesFundamentals of Fluid and Electrolyte BalanceMelia Eka Rosita PharmacistNo ratings yet
- MR Akinola Ao Blood and Body Fluid Physiologyoer1579668Document24 pagesMR Akinola Ao Blood and Body Fluid Physiologyoer1579668Joshua NyazonNo ratings yet
- CKD + Kejang SuyonoDocument15 pagesCKD + Kejang Suyonodevi_pramulawatiNo ratings yet
- Morning Report: June 2022 Physician in ChargeDocument24 pagesMorning Report: June 2022 Physician in ChargeIka AyuNo ratings yet
- Morning Report: Date: 25-07-2019Document30 pagesMorning Report: Date: 25-07-2019Aryo SupodoNo ratings yet
- MD-4 Body Fluid Compartments PlasmaaDocument24 pagesMD-4 Body Fluid Compartments PlasmaavincenzoNo ratings yet
- Fisiologi Cairan MikDocument18 pagesFisiologi Cairan MikRezky Prilya WidyastutiNo ratings yet
- MR Belakang 24022021 RAM Ca Buli EDITDocument25 pagesMR Belakang 24022021 RAM Ca Buli EDITWilujeng AnggrainiNo ratings yet
- Gangguan Keseimbangan Cairan Dan Elektrolit Pada PGKDocument89 pagesGangguan Keseimbangan Cairan Dan Elektrolit Pada PGKfransiska wijoyoNo ratings yet
- Metabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentFrom EverandMetabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentCarole IchaiNo ratings yet
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Peran Pemeriksaan Kesehatan Awal, Berkala Dan Khusus: DR - Mariaman Tjendera, M.KesDocument34 pagesPeran Pemeriksaan Kesehatan Awal, Berkala Dan Khusus: DR - Mariaman Tjendera, M.KesEdo eaNo ratings yet
- Jl. Raya Lawu No. 11 Tawangmangu, Jawa Tengah, IndonesiaDocument10 pagesJl. Raya Lawu No. 11 Tawangmangu, Jawa Tengah, IndonesiaEdo eaNo ratings yet
- Comparison of Safety and Efficacy of Intramuscular and Intravenous Regime of Magnesium Sulfate in Eclampsia and Severe PreeclampsiaDocument5 pagesComparison of Safety and Efficacy of Intramuscular and Intravenous Regime of Magnesium Sulfate in Eclampsia and Severe PreeclampsiaEdo eaNo ratings yet
- The Role of Giving High Dose Calcium For Preventing PreeclampsiaDocument9 pagesThe Role of Giving High Dose Calcium For Preventing PreeclampsiaEdo eaNo ratings yet
- Ebook - Scientific Insights Into Natural Therapies For Reversing Chronic and Autoimmune DiseasesDocument75 pagesEbook - Scientific Insights Into Natural Therapies For Reversing Chronic and Autoimmune DiseasesKen NanNo ratings yet
- Free THYROXINE (fT4) : Enzyme Immunoassay Test Kit Catalog Number: 10306Document4 pagesFree THYROXINE (fT4) : Enzyme Immunoassay Test Kit Catalog Number: 10306Yousra Zeidan100% (1)
- Notes - Human Body Form and FunctionDocument14 pagesNotes - Human Body Form and FunctionVisalakshi VenkatNo ratings yet
- Thyroxine and OxytocinDocument53 pagesThyroxine and OxytocinUshna SiddiquiNo ratings yet
- Week 15 16 Module Biochem Lec EndocrinologyDocument19 pagesWeek 15 16 Module Biochem Lec EndocrinologyLy xyNo ratings yet
- Why Does Glucometer Reading Is High Compared To Lab Test Reading - QuoraDocument42 pagesWhy Does Glucometer Reading Is High Compared To Lab Test Reading - QuoraSrinivasan ChidambaramNo ratings yet
- Cholinergic AntagonistDocument17 pagesCholinergic AntagonistShahid HameedNo ratings yet
- CAPE Biology 2004 U2 P1Document20 pagesCAPE Biology 2004 U2 P1Sheniqua Greaves100% (1)
- FRCEM ExamPrep GITDocument30 pagesFRCEM ExamPrep GITsk100% (1)
- 3 Ke 6 T 76 PIu 1 V J1 QQB WFGSWK OGdohkiuoiDocument4 pages3 Ke 6 T 76 PIu 1 V J1 QQB WFGSWK OGdohkiuoirizwan.arya085No ratings yet
- FGF21 Activates AMPK Signaling: Impact On Metabolic Regulation and The Aging ProcessDocument9 pagesFGF21 Activates AMPK Signaling: Impact On Metabolic Regulation and The Aging ProcessaginaNo ratings yet
- Opportunities and Challenges in The Therapeutic Activation of Human Energy Expenditure and Thermogenesis To Manage ObesityDocument17 pagesOpportunities and Challenges in The Therapeutic Activation of Human Energy Expenditure and Thermogenesis To Manage ObesityJosé Manuel Mendez MorenoNo ratings yet
- 1000 MCQs Food NutritionDocument153 pages1000 MCQs Food NutritionSaba ChaudhryNo ratings yet
- Treatment of Maternal Hypergalactia: Invited ReviewDocument3 pagesTreatment of Maternal Hypergalactia: Invited ReviewMaria ChristodoulouNo ratings yet
- Ebook Anatomy and Physiology 2Nd Edition Unknown Online PDF All ChapterDocument69 pagesEbook Anatomy and Physiology 2Nd Edition Unknown Online PDF All Chapterroy.burleson154100% (11)
- Hormones in Food As A Potential Risk For Human RepDocument16 pagesHormones in Food As A Potential Risk For Human RepRitu ShewaniNo ratings yet
- Toxi NotesDocument69 pagesToxi NotesJan Marc Ilagan100% (1)
- Lp-PLA2 MaglumiDocument6 pagesLp-PLA2 MaglumiLaboratoire Dr Mansouri Reghaia AlgerNo ratings yet
- DXN Spirulina PresentationDocument30 pagesDXN Spirulina PresentationHamza JawadNo ratings yet
- Metabolism (Ncm-216)Document10 pagesMetabolism (Ncm-216)Sofronio OmboyNo ratings yet
- Dianafood Prebiocran Brochure 23 500kbDocument12 pagesDianafood Prebiocran Brochure 23 500kbtrlaboNo ratings yet
- Heterophilic Antibody Interference Affecting Multiple Hormone Assays: Is It Due To Rheumatoid Factor?Document4 pagesHeterophilic Antibody Interference Affecting Multiple Hormone Assays: Is It Due To Rheumatoid Factor?mayra almaNo ratings yet
- Inborn Errors of Metabolismiem Lecture 1Document32 pagesInborn Errors of Metabolismiem Lecture 1EMMANUEL ABEL IMAH100% (1)
- Pathophysiology and Management of Diabetes Mellitus GppqeDocument60 pagesPathophysiology and Management of Diabetes Mellitus GppqeOlivia OliverNo ratings yet
- Hidradenitis Suppurativa DietDocument3 pagesHidradenitis Suppurativa DietJosse RiverNo ratings yet
- Test Bank For Lehnes Pharmacology For Nursing Care Burchum 9th EditionDocument20 pagesTest Bank For Lehnes Pharmacology For Nursing Care Burchum 9th EditionLily Rector100% (45)
- PBL Case Outline and Facilitator Guide: Students Should Be Able ToDocument3 pagesPBL Case Outline and Facilitator Guide: Students Should Be Able ToJoe ByntineNo ratings yet
- Breast - Mammary GlandDocument16 pagesBreast - Mammary GlandEniola DaramolaNo ratings yet
- ADS ADEA ANZCA NZSSD - DKA - SGLT2i - Alert - Ver July 2022Document3 pagesADS ADEA ANZCA NZSSD - DKA - SGLT2i - Alert - Ver July 2022tom.condon.02No ratings yet