Download as ppt, pdf, or txt
You might also like
- Handbook of Healthcare in The Arab World 2021 PDFDocument3,568 pagesHandbook of Healthcare in The Arab World 2021 PDFJose LozanoNo ratings yet
- Atozet Slide Deck New-PresentationDocument49 pagesAtozet Slide Deck New-PresentationMustafa JaradatNo ratings yet
- WCLC2021 Abstract Book - Final 16310719983133277Document1,066 pagesWCLC2021 Abstract Book - Final 16310719983133277Shawn Gaurav Jha100% (1)
- GOLD Report 2015Document115 pagesGOLD Report 2015Ana M Gomez ANo ratings yet
- Choosing The Right DPP-4i: Translating Evidence To PracticeDocument33 pagesChoosing The Right DPP-4i: Translating Evidence To PracticeRohit ThanageNo ratings yet
- Cardiovascular Physiology MCQsDocument24 pagesCardiovascular Physiology MCQsKlarens Affana63% (8)
- Aha GuidlineDocument7 pagesAha GuidlineMidyan AjiarsoNo ratings yet
- Sample of Chapter 3 Learning OutcomeDocument6 pagesSample of Chapter 3 Learning Outcomejacob adornaNo ratings yet
- Gold 2017Document139 pagesGold 2017reza tryasNo ratings yet
- Biomarker Copd PDFDocument35 pagesBiomarker Copd PDFManoj KumarNo ratings yet
- Food Eponyms in Pathology PDFDocument6 pagesFood Eponyms in Pathology PDFJose PhilipeNo ratings yet
- 4-Key Findings From CaprieDocument30 pages4-Key Findings From CaprieMuhammad Yolandi SumadioNo ratings yet
- GOLD Pocket 2010mar31Document30 pagesGOLD Pocket 2010mar31Fatimah Az-zahraNo ratings yet
- Emerg'ng MRKTDocument22 pagesEmerg'ng MRKTCanan KamışlıNo ratings yet
- Ankle Fracture EponymsDocument7 pagesAnkle Fracture Eponymsyarianna2No ratings yet
- EvaluatePharma World Preview 2020 - 0Document32 pagesEvaluatePharma World Preview 2020 - 0solej100% (1)
- Alcoholic Liver Disease BrochureDocument3 pagesAlcoholic Liver Disease Brochureapi-344630051No ratings yet
- Pearls and Pitfalls of Cardiac ImagingDocument4 pagesPearls and Pitfalls of Cardiac ImagingGordana PuzovicNo ratings yet
- Agility SMB Playbook v3 enGBDocument12 pagesAgility SMB Playbook v3 enGBMonika KravetzNo ratings yet
- SAVOR TIMI 53 Presentation SlidesDocument29 pagesSAVOR TIMI 53 Presentation SlidesSheila ZivanaNo ratings yet
- GOLD 2019 v1.7 FINAL 14nov2018 WMS DikonversiDocument155 pagesGOLD 2019 v1.7 FINAL 14nov2018 WMS DikonversiDomianus NamuwaliNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesWee DaliNo ratings yet
- Updates On Metformin JDM2019 DTDocument37 pagesUpdates On Metformin JDM2019 DTLaurentius JohanNo ratings yet
- Approved Training CentersDocument1 pageApproved Training Centersdehata9928No ratings yet
- Action Plan For Q3Document29 pagesAction Plan For Q3Shah Faisal99No ratings yet
- Hypertension Guidelines Slides - VFDocument23 pagesHypertension Guidelines Slides - VFNazmul Hasan MahmudNo ratings yet
- GOLDReport07 0108 PDFDocument109 pagesGOLDReport07 0108 PDFZaady Garcés ZulleymánNo ratings yet
- Competitive Intelligence and Analytics: © 2015 Indegene. All Rights ReservedDocument33 pagesCompetitive Intelligence and Analytics: © 2015 Indegene. All Rights Reservedpratk2No ratings yet
- Marketing Plan (Larith)Document65 pagesMarketing Plan (Larith)aamirNo ratings yet
- PriceDocument5 pagesPriceMubarak MHNo ratings yet
- Final CRM PharmaDocument16 pagesFinal CRM PharmaSachin A KhochareNo ratings yet
- Lokesh Patil (22) - Madhura Jagtap (10) - Animesh Amal (01) - Vishal Mehta (16) - Khushbu MascarenhasDocument44 pagesLokesh Patil (22) - Madhura Jagtap (10) - Animesh Amal (01) - Vishal Mehta (16) - Khushbu MascarenhasAnonymous 75aETJ8ONo ratings yet
- Telfast Product PresentationDocument32 pagesTelfast Product PresentationDewi Sri NuritaNo ratings yet
- Augmentin EffectsDocument39 pagesAugmentin EffectsJasmeen SutariyaNo ratings yet
- Drug Delivery Research AdvancesDocument270 pagesDrug Delivery Research AdvancesParina Fernandes100% (1)
- Stratanalysis Document: AZ S Brilinta Reports Favorable Trial III ResultsDocument7 pagesStratanalysis Document: AZ S Brilinta Reports Favorable Trial III ResultsJaweed SheikhNo ratings yet
- Product Overview Product Overview: Difficile Associated DiarrheaDocument2 pagesProduct Overview Product Overview: Difficile Associated Diarrheamichael bundalianNo ratings yet
- NeoFansidar Business PlanDocument65 pagesNeoFansidar Business PlanMuhammad SalmanNo ratings yet
- Glevo RespicareDocument58 pagesGlevo RespicarekurutalaNo ratings yet
- Diola: Introductory Training CourseDocument36 pagesDiola: Introductory Training CourseDastogir AlamNo ratings yet
- Pharma HCPEngagement Report - vs01Document49 pagesPharma HCPEngagement Report - vs01Abhishek SoniNo ratings yet
- Johnson & Johnson: "Caring For You From The Beginning, To The Very End!"Document18 pagesJohnson & Johnson: "Caring For You From The Beginning, To The Very End!"Kaushik BalachandarNo ratings yet
- Trauma Care - Medical Devices - Blue Ocean - Developing Countries - Value For Money Segmentation ReportDocument116 pagesTrauma Care - Medical Devices - Blue Ocean - Developing Countries - Value For Money Segmentation ReportEinsteinAlbertKesiNo ratings yet
- VWQECQWEWQDocument39 pagesVWQECQWEWQEdward Roy “Ying” AyingNo ratings yet
- Zykast MKTDocument25 pagesZykast MKTkhanhquphamNo ratings yet
- HBR Zeneration TimeDocument43 pagesHBR Zeneration TimeIqbal FirdausNo ratings yet
- Avalox in Aecb: PP-AVE-JO-0006-1Document160 pagesAvalox in Aecb: PP-AVE-JO-0006-1Mustafa JaradatNo ratings yet
- Atorva Final PDFDocument19 pagesAtorva Final PDFKshama ShahNo ratings yet
- AnxolamDocument38 pagesAnxolammanjitdeshmukh2No ratings yet
- Investor Presentation (Shalby Hospitals)Document42 pagesInvestor Presentation (Shalby Hospitals)misfitmedicoNo ratings yet
- Materi Narasumber 2 - Halal Pharmaceutical From The Perspectives of Industry (IAI Webinar) FINALDocument27 pagesMateri Narasumber 2 - Halal Pharmaceutical From The Perspectives of Industry (IAI Webinar) FINALTini SyamsuddinNo ratings yet
- Pharmaceutical Sector ProfileDocument3 pagesPharmaceutical Sector ProfileḾiroIacovlevNo ratings yet
- Empagliflozin and Linagliptin 2020 Sept FinalDocument65 pagesEmpagliflozin and Linagliptin 2020 Sept FinalJenny Calapati TorrijosNo ratings yet
- Sales Excellence in The Pharma IndustryDocument4 pagesSales Excellence in The Pharma IndustryKushal AgrawalNo ratings yet
- Group 1 - LowprazoleDocument32 pagesGroup 1 - LowprazoleAhmed AlaaNo ratings yet
- Antiplatelet Pada ACSDocument22 pagesAntiplatelet Pada ACSRidyah Ning TyasNo ratings yet
- Antiplatelet Therapy September 2013Document31 pagesAntiplatelet Therapy September 2013Randilufti SantosoNo ratings yet
- Adalat CC (Nifedipine) Extended Release Tablets: For Oral UseDocument15 pagesAdalat CC (Nifedipine) Extended Release Tablets: For Oral UseRiska AuliahNo ratings yet
- Possible Impact of Nitric Oxide On The Antihypertensive Effect of Captopril and ZaprinastDocument6 pagesPossible Impact of Nitric Oxide On The Antihypertensive Effect of Captopril and ZaprinastdeddyNo ratings yet
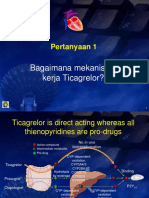
- Pertanyaan ACS TicagrelorDocument5 pagesPertanyaan ACS TicagrelorwhitecoatNo ratings yet
- Pengaruh Simulasi Tindakan Resusitasi Jantung Paru (RJP) Terhadap Tingkat Motivasi Siswa Menolong Korban Henti Jantung Di Sma Negeri 9 Binsus ManadoDocument11 pagesPengaruh Simulasi Tindakan Resusitasi Jantung Paru (RJP) Terhadap Tingkat Motivasi Siswa Menolong Korban Henti Jantung Di Sma Negeri 9 Binsus ManadoWist Eria SyndromeNo ratings yet
- Ecg Utah EduDocument87 pagesEcg Utah EduMos Viorel DanutNo ratings yet
- Electrocardiography On Congenital Heart DiseaseDocument31 pagesElectrocardiography On Congenital Heart DiseasedavitlieNo ratings yet
- Cardioversion and DefibrillationDocument18 pagesCardioversion and DefibrillationJannah Marie A. Dimaporo100% (4)
- Case 1 KCSDocument16 pagesCase 1 KCSswaleh breik misfirNo ratings yet
- Vascular Survival GuideDocument8 pagesVascular Survival GuideJames OyeniyiNo ratings yet
- Pre Board 2Document32 pagesPre Board 2S.N. SwamiNo ratings yet
- Consenso Siben HTPPDocument14 pagesConsenso Siben HTPPCristinaNo ratings yet
- 10 1016@j Amjcard 2018 03 369Document21 pages10 1016@j Amjcard 2018 03 369Martin De Santiago ValenzuelaNo ratings yet
- Exercise Based Cardiac Rehabilitation For Coronary Heart Disease 2021Document266 pagesExercise Based Cardiac Rehabilitation For Coronary Heart Disease 2021Josemi Del Castillo MolinaNo ratings yet
- The Effect of Ergonomic Exercise On Changes in Blood Pressure in Patients With HypertensionDocument11 pagesThe Effect of Ergonomic Exercise On Changes in Blood Pressure in Patients With HypertensionRizky MocinNo ratings yet
- Cath Lab PlanningDocument20 pagesCath Lab PlanningJune Karki100% (1)
- Diet 1Document4 pagesDiet 1Nouman Safdar AliNo ratings yet
- Omron HEM-650 ManualDocument36 pagesOmron HEM-650 ManualWayne S CooperNo ratings yet
- Literature Review: Terapi Relaksasi Otot Progresif Terhadap Penurunan Tekanan Darah Pada Pasien HipertensiDocument8 pagesLiterature Review: Terapi Relaksasi Otot Progresif Terhadap Penurunan Tekanan Darah Pada Pasien Hipertensinadia hanifaNo ratings yet
- Contoh Soal Hipertensi + PTO HT +HL 02Document39 pagesContoh Soal Hipertensi + PTO HT +HL 02Arif RahmanNo ratings yet
- JACC Volume 78, Issue 11 SeptemberDocument122 pagesJACC Volume 78, Issue 11 SeptemberFareesha KhanNo ratings yet
- Procedure: Ankle Brachial Index (ABI) in Adults Using A Handheld DopplerDocument8 pagesProcedure: Ankle Brachial Index (ABI) in Adults Using A Handheld DopplerFachril ismailNo ratings yet
- New Concept For CTO Guidewire Manipulation Importance of Penetration Plane View (PPV)Document27 pagesNew Concept For CTO Guidewire Manipulation Importance of Penetration Plane View (PPV)MuMoMaNo ratings yet
- Heart AnatomyDocument11 pagesHeart AnatomyJohn FisherNo ratings yet
- Manajemen Perioperatif Operasi Arterial Switch PadaDocument12 pagesManajemen Perioperatif Operasi Arterial Switch Padacomiza92No ratings yet
- Atow 459 00Document9 pagesAtow 459 00Javier Fernando Cabezas MeloNo ratings yet
- Announcement IACA 2024.3Document16 pagesAnnouncement IACA 2024.3alimufisNo ratings yet
- Basic Life SupportDocument2 pagesBasic Life SupportDaphne SanchaNo ratings yet
- ElectrocardiogramDocument2 pagesElectrocardiogramPAG-A, Daily Joy LNo ratings yet
- Basic ECG For Refresher Course 2014Document116 pagesBasic ECG For Refresher Course 2014Winz DolleteNo ratings yet
- Cardiac SurgeryDocument25 pagesCardiac SurgeryMohamed HamdyNo ratings yet
- ESH-IP 2010 Validation of Nissei DSK-1031Document3 pagesESH-IP 2010 Validation of Nissei DSK-1031Pub PleNo ratings yet
- ECG InterpretationDocument5 pagesECG InterpretationjenNo ratings yet