Download as pptx, pdf, or txt
You might also like
- Nursing Care Plan Urinary Tract Infection (UTI)Document2 pagesNursing Care Plan Urinary Tract Infection (UTI)deric95% (99)
- Chronic Kidney DiseaseDocument40 pagesChronic Kidney DiseasePaul SinsNo ratings yet
- SGD Case OrbitDocument2 pagesSGD Case OrbitJewelNo ratings yet
- Noel A. Villanueva, MD, FPCP, FPSNDocument62 pagesNoel A. Villanueva, MD, FPCP, FPSNagilNo ratings yet
- Ngaji Arrythmia Cordis 3Document122 pagesNgaji Arrythmia Cordis 3Dhita Dwi NandaNo ratings yet
- Integrated Therapeutics IiDocument165 pagesIntegrated Therapeutics IiSalahadinNo ratings yet
- ICU Scoring Systems: Telemed - Shams.edu - Eg/moodleDocument56 pagesICU Scoring Systems: Telemed - Shams.edu - Eg/moodlealfian sinaga100% (1)
- Inter'Medic CKDDocument31 pagesInter'Medic CKDMAHEJS HD100% (1)
- Cirrhosis of LiverDocument106 pagesCirrhosis of LiveraahadNo ratings yet
- Hemant Mahanand (201941103034) Case StudyDocument50 pagesHemant Mahanand (201941103034) Case StudyHemiNo ratings yet
- Acute Kidney InjuryDocument60 pagesAcute Kidney InjuryAbegail Fermanejo-GeneraoNo ratings yet
- Hypertension LecturesDocument65 pagesHypertension LecturesAdebisiNo ratings yet
- AAH v2 Acute AsthmaDocument81 pagesAAH v2 Acute AsthmaEssa SmjNo ratings yet
- Study of Joundice 1Document38 pagesStudy of Joundice 1omsai cyber cafeNo ratings yet
- Vaman Virechan Dravyas in KalpasthanaDocument10 pagesVaman Virechan Dravyas in KalpasthanaShreyans DoshiNo ratings yet
- Chronic Kidney Disease: For The Primary Care PhysicianDocument54 pagesChronic Kidney Disease: For The Primary Care PhysicianFlavia PolodeanuNo ratings yet
- High Altitude IllnessDocument9 pagesHigh Altitude Illnesswana_iswaraNo ratings yet
- Doze IECA - SartaniDocument2 pagesDoze IECA - SartaniAlexandraNo ratings yet
- RA Management UpdateDocument43 pagesRA Management UpdateFaheem Ul HasanNo ratings yet
- Ecart MedicationsDocument39 pagesEcart Medicationsanon_140774008No ratings yet
- Management of Heart Failure: DR Ambakederemo TE Consultant Physician/cardiologist NduthDocument71 pagesManagement of Heart Failure: DR Ambakederemo TE Consultant Physician/cardiologist NduthPrincewill SeiyefaNo ratings yet
- Yuvan Pidika Acne EtiologyDocument8 pagesYuvan Pidika Acne EtiologyMSKCNo ratings yet
- Adhf 2023Document25 pagesAdhf 2023Mahamed Wefkey OmranNo ratings yet
- Fluid Electrolyte Imbalance n132 160210135651Document100 pagesFluid Electrolyte Imbalance n132 160210135651Shahan FarooqNo ratings yet
- Amavata KCDocument45 pagesAmavata KCBarsha Meher100% (1)
- Anemia Prevention and Management Program Implementation GuideDocument60 pagesAnemia Prevention and Management Program Implementation GuideIchlasul MadriddistaNo ratings yet
- Candidiasis Kandidiasis/Kandidosis: Dr. Messia Paramita / RSUD SLEMANDocument11 pagesCandidiasis Kandidiasis/Kandidosis: Dr. Messia Paramita / RSUD SLEMANAulya ArchuletaNo ratings yet
- Final GIT Case PresentationDocument53 pagesFinal GIT Case PresentationRovan100% (1)
- Clostridium Difficile: Dr.T.V.Rao MDocument67 pagesClostridium Difficile: Dr.T.V.Rao Mtummalapalli venkateswara raoNo ratings yet
- Management of Severe Hypertension, Hypertension in Special ConditionDocument43 pagesManagement of Severe Hypertension, Hypertension in Special Conditionabhandlung100% (3)
- Chronic Kidney Disease - UnhaluDocument57 pagesChronic Kidney Disease - UnhaluRahmawati HamudiNo ratings yet
- How To Position Finerenone in The Treatment Algorithm For Type 2 Diabetes With Renal Complication - GPMPDocument27 pagesHow To Position Finerenone in The Treatment Algorithm For Type 2 Diabetes With Renal Complication - GPMPTaufiqurrokhman RofiiNo ratings yet
- Azathioprine DrugDocument18 pagesAzathioprine DrugteritohahaNo ratings yet
- Computation of Drips: Marla Aurora JacobaDocument18 pagesComputation of Drips: Marla Aurora JacobaAnne Lorraine Bringas100% (1)
- Atypical PneumoniaDocument30 pagesAtypical PneumoniachandanNo ratings yet
- Physiology Rapid RevisionDocument41 pagesPhysiology Rapid RevisionAsif MohammedNo ratings yet
- Ton Mitral Valve ReplacementDocument3 pagesTon Mitral Valve ReplacementSony TonNo ratings yet
- STEP HPEF Trial NEJm 2023Document16 pagesSTEP HPEF Trial NEJm 2023felipeNo ratings yet
- Department of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Document51 pagesDepartment of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12No ratings yet
- Diabetes Mellitus DR Moses KazeevuDocument81 pagesDiabetes Mellitus DR Moses KazeevuMoses Jr KazevuNo ratings yet
- Nephrotic Syndrome 2016Document45 pagesNephrotic Syndrome 2016alaaNo ratings yet
- Pain Management PDFDocument38 pagesPain Management PDFYulia Fransisca PurbaNo ratings yet
- Lekhana VastiDocument7 pagesLekhana VastiDrMohamed RifasNo ratings yet
- National Guideline For Dengue 2018 PDFDocument96 pagesNational Guideline For Dengue 2018 PDFTapash GopeNo ratings yet
- Urinary Tract DisorderDocument63 pagesUrinary Tract DisorderShivaranjan KsNo ratings yet
- GrahaniDocument7 pagesGrahanishreyanka raoNo ratings yet
- Acute Kidney Injury DR Moses KazevuDocument52 pagesAcute Kidney Injury DR Moses KazevuMoses Jr KazevuNo ratings yet
- Acute Pulmonary Embolism Final YearDocument52 pagesAcute Pulmonary Embolism Final YearUzma BanoNo ratings yet
- Vatavyadhi - 5Document1 pageVatavyadhi - 5Thala ThalapatyNo ratings yet
- Copd 2022Document45 pagesCopd 2022Mubassir NisarNo ratings yet
- Pulmonary EmbolismDocument61 pagesPulmonary Embolismjhk0428No ratings yet
- Cardiovascular Safety of Anti-Diabetic Drugs - KarklinDocument42 pagesCardiovascular Safety of Anti-Diabetic Drugs - KarklinCharles SaputraNo ratings yet
- Ecg BasicsDocument25 pagesEcg BasicsKailas Nath100% (1)
- Hypokalaemia and HyperkalaemiaDocument39 pagesHypokalaemia and HyperkalaemiaRZ NgNo ratings yet
- General Central and Peripheral Nertvous SystemDocument5 pagesGeneral Central and Peripheral Nertvous SystemSubramaniam KrishnamoorthiNo ratings yet
- Vidconf Diuretic Antidiuretic 2014Document51 pagesVidconf Diuretic Antidiuretic 2014naltrisilvianNo ratings yet
- HyperlipidemiaDocument38 pagesHyperlipidemiaAadhan ArveeNo ratings yet
- List of Causative AgentDocument26 pagesList of Causative AgentMe2 ModhNo ratings yet
- Treatment of GoutDocument21 pagesTreatment of GoutAlbertoBeltránRojasNo ratings yet
- Malaria Treatment UpdateDocument45 pagesMalaria Treatment UpdateGyabaah Yeboah AndrewsNo ratings yet
- Endocrine HTNDocument32 pagesEndocrine HTNatik mayasariNo ratings yet
- 12a. Kuliah Aki 2017Document36 pages12a. Kuliah Aki 2017yussikafernandaNo ratings yet
- SGD Case Bustamante Patricia MaricDocument30 pagesSGD Case Bustamante Patricia MaricJewelNo ratings yet
- Vertebral Column and ContentsDocument5 pagesVertebral Column and ContentsJewelNo ratings yet
- Medical Books: Department of PathologyDocument6 pagesMedical Books: Department of PathologyJewelNo ratings yet
- Family PlanningDocument12 pagesFamily Planningeriska yunita sariNo ratings yet
- Kidney DiseasesDocument22 pagesKidney Diseasesphoto copyhemnNo ratings yet
- Republic of The Philippines Department of Health Regional Office-1 RHMPP 2018 Monthly Accomplishment Report For The Month o F JANUARY 2018Document2 pagesRepublic of The Philippines Department of Health Regional Office-1 RHMPP 2018 Monthly Accomplishment Report For The Month o F JANUARY 2018Rosendo BernabeNo ratings yet
- Perineal Urethrostomy PUDocument2 pagesPerineal Urethrostomy PUclara FNo ratings yet
- SurgeryDocument6 pagesSurgeryMuhammad Saad100% (1)
- Differential Diagnosis UrolithiasisDocument10 pagesDifferential Diagnosis UrolithiasisAldila Rc X ManiaNo ratings yet
- Etiology and Pathophysiology of Acute Kidney InjuryDocument4 pagesEtiology and Pathophysiology of Acute Kidney InjuryVictor TayoNo ratings yet
- Micturition 2022Document20 pagesMicturition 2022Mohammad zreadNo ratings yet
- Nursing Care Plan For Overflow Urinary Incontinence NCPDocument2 pagesNursing Care Plan For Overflow Urinary Incontinence NCPderic71% (7)
- Urine Culture Manual MT - SINAI PDFDocument15 pagesUrine Culture Manual MT - SINAI PDFAvi VermaNo ratings yet
- Extracorporeal Shock Wave Lithotripsy (ESWL) vs. Ureterorenoscopic (URS) Manipulation in Proximal Ureteric StoneDocument5 pagesExtracorporeal Shock Wave Lithotripsy (ESWL) vs. Ureterorenoscopic (URS) Manipulation in Proximal Ureteric Stonealifah hainunNo ratings yet
- RICHARD WOLF Mega Stone LaserDocument12 pagesRICHARD WOLF Mega Stone Laserhassan MOHACHINo ratings yet
- To Promote Good Hygiene and Physical Comfort.: Coli (E. Coli), NormallyDocument2 pagesTo Promote Good Hygiene and Physical Comfort.: Coli (E. Coli), NormallyFran LanNo ratings yet
- Patent US6447462Document15 pagesPatent US6447462Yodi SoebadiNo ratings yet
- List of Medical Facilities in India: Prepared by British High Commission New DelhiDocument82 pagesList of Medical Facilities in India: Prepared by British High Commission New DelhiKRISHNA RAJ JNo ratings yet
- From Better Sex To Mindblowing AdventureDocument16 pagesFrom Better Sex To Mindblowing AdventureAdriana OrtegaNo ratings yet
- Sistem EkskresiDocument8 pagesSistem EkskresiNatasyaNo ratings yet
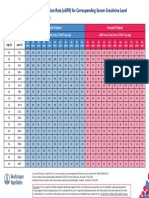
- Egfr ChartDocument1 pageEgfr ChartMahesh DoshiNo ratings yet
- Vesicaria Communis John Henry Clarke: 21 Homeopathic Medicines Dr. Shah FaisalDocument3 pagesVesicaria Communis John Henry Clarke: 21 Homeopathic Medicines Dr. Shah FaisalShah FaisalNo ratings yet
- ABP New Content Outline PDFDocument14 pagesABP New Content Outline PDFJeremy PorterNo ratings yet
- Incision Access UrologyDocument47 pagesIncision Access UrologyHafizur RashidNo ratings yet
- LSS The Laparoscopic Surgical Skills ProgrammeDocument31 pagesLSS The Laparoscopic Surgical Skills ProgrammeSociedade Portuguesa de CirurgiaNo ratings yet
- Urinary System Nuclear Medicine: Renal ImagingDocument68 pagesUrinary System Nuclear Medicine: Renal Imagingapi-19916399No ratings yet
- Prostate Cancer: Presented By, Denna Benny Roll. No:21 3 Year B. SC NursingDocument58 pagesProstate Cancer: Presented By, Denna Benny Roll. No:21 3 Year B. SC NursingSamuel LalNo ratings yet
- Non-Gonococcal Urethritis (NGU) : Signs and SymptomsDocument2 pagesNon-Gonococcal Urethritis (NGU) : Signs and SymptomsIkhfa Yusril BahariNo ratings yet
- Transurethral Resection of The ProstateDocument48 pagesTransurethral Resection of The Prostateralf_dolanNo ratings yet
- PUF QuestionnaireDocument1 pagePUF Questionnaireatrb324No ratings yet
- MAPEH 10 1st Summative TestDocument3 pagesMAPEH 10 1st Summative TestAshierah MontasNo ratings yet
- Benign Prostatic HyperplasiaDocument15 pagesBenign Prostatic HyperplasiaPediatrics - Pediatric SurgeryNo ratings yet