Download as pptx, pdf, or txt
You might also like
- Canada Gateway MCC Qe Questions 1Document100 pagesCanada Gateway MCC Qe Questions 1Kak KfgaNo ratings yet
- NCLEX Cardiovascular Exam 2020 - Questions and AnswersDocument74 pagesNCLEX Cardiovascular Exam 2020 - Questions and AnswersNeoGellin83% (6)
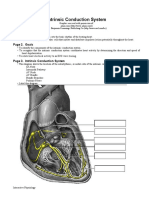
- Intrinsic Conduction System: Page 1. IntroductionDocument5 pagesIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNo ratings yet
- POMR FIN CholangitisDocument29 pagesPOMR FIN Cholangitisphyna27No ratings yet
- SOS AYU - Ax - PeunjangDocument11 pagesSOS AYU - Ax - PeunjangIka AyuNo ratings yet
- Hypocalcemia, Hypoparathyroid WahyuDocument27 pagesHypocalcemia, Hypoparathyroid WahyuFerdinando BaehaNo ratings yet
- Heteroanamnesa Chief Complaint: Coffe Ground Vomiting History of Present IllnessDocument6 pagesHeteroanamnesa Chief Complaint: Coffe Ground Vomiting History of Present IllnessIka AyuNo ratings yet
- Duty Report Saturday, May 2 2015 Dr. Ramadhan Physician in ChargeDocument6 pagesDuty Report Saturday, May 2 2015 Dr. Ramadhan Physician in ChargeCristian RajagukgukNo ratings yet
- ArestrdyuguycdrsrtDocument29 pagesArestrdyuguycdrsrtAryo SupodoNo ratings yet
- Morning ReportDocument22 pagesMorning ReportNiinna AwliaNo ratings yet
- Template MRDocument27 pagesTemplate MRdipo buyerNo ratings yet
- Morning ReportDocument27 pagesMorning ReportDody PrasetyaNo ratings yet
- LeptospirosisDocument19 pagesLeptospirosisFelicia adeline ChristianNo ratings yet
- Morning Report: Date: Monday, 2 November 2020Document24 pagesMorning Report: Date: Monday, 2 November 2020Ika AyuNo ratings yet
- Morning Report: Date: 25-07-2019Document30 pagesMorning Report: Date: 25-07-2019Aryo SupodoNo ratings yet
- FINAL CervicalCA7BDocument6 pagesFINAL CervicalCA7BRommel OliverasNo ratings yet
- Morning Report: June 2022 Physician in ChargeDocument24 pagesMorning Report: June 2022 Physician in ChargeIka AyuNo ratings yet
- Summary of Data Base: MR Z/41 YO/W.26Document35 pagesSummary of Data Base: MR Z/41 YO/W.26Faricha KurniaNo ratings yet
- Case Based DiscussionDocument49 pagesCase Based DiscussionMaulana IbrahimNo ratings yet
- DK Gastro KonsulDocument56 pagesDK Gastro Konsuldenina setyaNo ratings yet
- DK IKA 1 - Ogie RevDocument193 pagesDK IKA 1 - Ogie RevhariogieNo ratings yet
- Mrs Siti Wahyuni/ 48 Yo/ Ward 25 Bed 1.6Document7 pagesMrs Siti Wahyuni/ 48 Yo/ Ward 25 Bed 1.6DoctoRides 46No ratings yet
- Morning Report: Physician in ChargeDocument33 pagesMorning Report: Physician in ChargeIka AyuNo ratings yet
- Stemi Anterior ExtensiveDocument29 pagesStemi Anterior ExtensiveNur Abidatul FitriaNo ratings yet
- MR R 26 6-3 2017 MR W Fix AMS Septic AKIDocument15 pagesMR R 26 6-3 2017 MR W Fix AMS Septic AKISafira RNo ratings yet
- Morning Report Case: 7th October, 2011Document29 pagesMorning Report Case: 7th October, 2011Felicia adeline ChristianNo ratings yet
- TN Ahmad KusaeriDocument5 pagesTN Ahmad KusaeriCristian RajagukgukNo ratings yet
- Mrs. Fera Febriyani/ 27 y.o/MR 1.43.51.17 Admitted On July 27 2019 at 11.00 PMDocument11 pagesMrs. Fera Febriyani/ 27 y.o/MR 1.43.51.17 Admitted On July 27 2019 at 11.00 PMmonyet65No ratings yet
- Morning Report: Physician in ChargeDocument28 pagesMorning Report: Physician in Chargenando baehaNo ratings yet
- Template Duty ReportDocument6 pagesTemplate Duty ReportJefri SusantoNo ratings yet
- Morning Report: Dr. Dikara WS Maulidy, SP - PDDocument24 pagesMorning Report: Dr. Dikara WS Maulidy, SP - PDBethari Abi SafitriNo ratings yet
- DK Gastro Atresia Bilier - Ogie Feses LengkapDocument48 pagesDK Gastro Atresia Bilier - Ogie Feses LengkaphariogieNo ratings yet
- Tumor Board - Mucinous.Document54 pagesTumor Board - Mucinous.Apmc SchwartzNo ratings yet
- DK IPD 3 - Ogie AsitesDocument174 pagesDK IPD 3 - Ogie AsiteshariogieNo ratings yet
- Infective EndocarditisDocument8 pagesInfective EndocarditisAiman Arifin100% (1)
- MR - Suardi Tumor Paru + Efusi Pleura KiriDocument14 pagesMR - Suardi Tumor Paru + Efusi Pleura KiritiarapolarisiriuzNo ratings yet
- Template MR KosongDocument28 pagesTemplate MR KosongDoctoRides 46No ratings yet
- Morning Report: Friday 20 April 2012Document18 pagesMorning Report: Friday 20 April 2012Felicia adeline ChristianNo ratings yet
- CKD + Kejang SuyonoDocument15 pagesCKD + Kejang Suyonodevi_pramulawatiNo ratings yet
- DK Gastro EditDocument65 pagesDK Gastro Editdenina setyaNo ratings yet
- Morning Report: Sunday, Oktober 7 2018Document21 pagesMorning Report: Sunday, Oktober 7 2018Bhisma DewabrathaNo ratings yet
- MR Placenta Previa Dr. Edy SpOGDocument17 pagesMR Placenta Previa Dr. Edy SpOGtiaraNo ratings yet
- DK GastroDocument79 pagesDK Gastrodenina setyaNo ratings yet
- Friday 2-2-2018 Multiple MyelomaDocument20 pagesFriday 2-2-2018 Multiple MyelomaJefri SusantoNo ratings yet
- DK IKA-5 Raymond - Intra Abdominal Tumor in 7-Y.o-Boy With Renal FailureDocument45 pagesDK IKA-5 Raymond - Intra Abdominal Tumor in 7-Y.o-Boy With Renal FailurepudjoNo ratings yet
- MR SipDocument26 pagesMR SipFelicia adeline ChristianNo ratings yet
- MR DOC KAD DR HeriDocument16 pagesMR DOC KAD DR HeriIffaNo ratings yet
- ST Elevation Myocard InfarkDocument30 pagesST Elevation Myocard InfarkNancy Dwi Puspita100% (1)
- POMR - Belakang - Nanda NHL 0103Document36 pagesPOMR - Belakang - Nanda NHL 0103Wilujeng AnggrainiNo ratings yet
- DK Gastro KonsulDocument48 pagesDK Gastro Konsuldenina setyaNo ratings yet
- NC - Muhammad RaditDocument18 pagesNC - Muhammad RaditDodi DiNo ratings yet
- MR DM Hematemesis IMADocument15 pagesMR DM Hematemesis IMANadine BushNo ratings yet
- Duty Report: Sunday, 27 May 2018Document17 pagesDuty Report: Sunday, 27 May 2018HarisNo ratings yet
- Latihan POMR: Dr. Venna Febrian KDocument39 pagesLatihan POMR: Dr. Venna Febrian KLoudry ElfaNo ratings yet
- DK Gastro 2 - CA PankreasDocument111 pagesDK Gastro 2 - CA Pankreasdenina setyaNo ratings yet
- Morning Report CKDDocument20 pagesMorning Report CKDjoe joeNo ratings yet
- Morning Report: Physician in ChargeDocument29 pagesMorning Report: Physician in ChargeWilujeng AnggrainiNo ratings yet
- Afternoon Report 9 April 2017Document17 pagesAfternoon Report 9 April 2017Puteri Diah RahtiniNo ratings yet
- Morning Report: Doctor Incharge: Dr. Dikara WS Maulidy, SP - PDDocument21 pagesMorning Report: Doctor Incharge: Dr. Dikara WS Maulidy, SP - PDBethari Abi Safitri100% (1)
- Atherosclerotic Cardiovascular Disease - Critical CareDocument39 pagesAtherosclerotic Cardiovascular Disease - Critical CareAdolf Benedick Dacanay MalalaNo ratings yet
- Bisitopenia + HyperleukocytosisDocument77 pagesBisitopenia + Hyperleukocytosisdenina setyaNo ratings yet
- Morning Report: 7 February 2011Document20 pagesMorning Report: 7 February 2011adi_ancuxNo ratings yet
- Azotemia - Tumor BuliDocument2 pagesAzotemia - Tumor BuliWilujeng AnggrainiNo ratings yet
- MR BHD / 53 Y.o/ W.24ADocument22 pagesMR BHD / 53 Y.o/ W.24AWilujeng AnggrainiNo ratings yet
- Morning Report: Physician in ChargeDocument29 pagesMorning Report: Physician in ChargeWilujeng AnggrainiNo ratings yet
- Morning Report: 2 March 2021 Night ShiftDocument16 pagesMorning Report: 2 March 2021 Night ShiftWilujeng AnggrainiNo ratings yet
- Gangrene Hand of Mrs. Mustiah, 86 YoDocument27 pagesGangrene Hand of Mrs. Mustiah, 86 YoWilujeng AnggrainiNo ratings yet
- IGD BAR Confirmed CovidDocument4 pagesIGD BAR Confirmed CovidWilujeng AnggrainiNo ratings yet
- POMR - Belakang - Nanda NHL 0103Document36 pagesPOMR - Belakang - Nanda NHL 0103Wilujeng AnggrainiNo ratings yet
- Indri Astutik CAPD Peritonitis RezdyDocument2 pagesIndri Astutik CAPD Peritonitis RezdyWilujeng AnggrainiNo ratings yet
- 02-03-21 - Impending Thyroid Storm PerioperativeDocument4 pages02-03-21 - Impending Thyroid Storm PerioperativeWilujeng AnggrainiNo ratings yet
- Teaching-Learning Models in Clinical Setting: Susanto NugrohoDocument47 pagesTeaching-Learning Models in Clinical Setting: Susanto NugrohoWilujeng AnggrainiNo ratings yet
- Cue and Clue Problem List and Initial Diagnosis PlanningDocument2 pagesCue and Clue Problem List and Initial Diagnosis PlanningWilujeng AnggrainiNo ratings yet
- 18 - CHD ICU Management - Shunt LesionsDocument15 pages18 - CHD ICU Management - Shunt LesionsRAM SOFTWARENo ratings yet
- Operation Manual Stress Test Ast-3000Document16 pagesOperation Manual Stress Test Ast-3000AhmadAlBadiNo ratings yet
- ECG WorkbookDocument0 pagesECG WorkbookJim ThorntonNo ratings yet
- A Novel 12lead ECG System For Home Use - Development and Usability TestingDocument14 pagesA Novel 12lead ECG System For Home Use - Development and Usability Testing허세진No ratings yet
- ECGDocument41 pagesECGmiguel mendezNo ratings yet
- ElectrocardiogramDocument52 pagesElectrocardiogramMona AlhindiNo ratings yet
- Design and Development of A Heart Rate Measuring Device Using FingertipDocument6 pagesDesign and Development of A Heart Rate Measuring Device Using FingertipKazandra Cassidy GarciaNo ratings yet
- EkgDocument67 pagesEkgFendi Rafif Dad'sNo ratings yet
- EDHKL ACLS Manual - Final Edit (1) - 1Document43 pagesEDHKL ACLS Manual - Final Edit (1) - 1Nurhafizah IbrahimNo ratings yet
- Manual Cardiofax 1150 - PDF Free Download PDFDocument140 pagesManual Cardiofax 1150 - PDF Free Download PDFTường Nguyễn BáNo ratings yet
- Cardioline AR 1200 - Service ManualDocument38 pagesCardioline AR 1200 - Service ManualEuris Otilio Dominguez AmadisNo ratings yet
- ECG Workshop STUDENTDocument9 pagesECG Workshop STUDENToyim sNo ratings yet
- 1.5-DOH Reviewer & Examination-NurseDocument111 pages1.5-DOH Reviewer & Examination-NurseRoger CarpisoNo ratings yet
- Ekg BasicDocument24 pagesEkg BasicGhica CostinNo ratings yet
- DefiMonitor EVO 18 MGA22955Document238 pagesDefiMonitor EVO 18 MGA22955Piotr OkorskiNo ratings yet
- ReportDocument72 pagesReportAmyrul HaqiemNo ratings yet
- Basics of EKG InterpretationDocument68 pagesBasics of EKG InterpretationMarthaNo ratings yet
- Pulsebit EX User ManualDocument88 pagesPulsebit EX User ManualPredrag DjurdjevicNo ratings yet
- ECG Minesota CodeDocument7 pagesECG Minesota CodeIman AzrbjNo ratings yet
- Introduction To ECG: Presenter: Emiacu Kenneth Facilitator: Dr. Ssebuliba MosesDocument36 pagesIntroduction To ECG: Presenter: Emiacu Kenneth Facilitator: Dr. Ssebuliba MosesNinaNo ratings yet
- Picu Ready RecknerDocument2 pagesPicu Ready RecknerPranitha Reddy0% (1)
- Basic Ecg Interpretation For NursesDocument4 pagesBasic Ecg Interpretation For Nurseskimberly dobleNo ratings yet
- Thesis Word-3 PDFDocument82 pagesThesis Word-3 PDFSaitejaNo ratings yet
- ECG Lead Placement and Lead Reversal GuideDocument2 pagesECG Lead Placement and Lead Reversal Guidealfurlani100% (1)
- Sample Pages of Koncpt 20 Authors 2nd EditionDocument25 pagesSample Pages of Koncpt 20 Authors 2nd EditionvkNo ratings yet
- Adverse Drug Event of Hypokalaemia-Induced Cardiotoxicity Secondary To The Use of Laxatives: A Systematic Review of Case ReportsDocument10 pagesAdverse Drug Event of Hypokalaemia-Induced Cardiotoxicity Secondary To The Use of Laxatives: A Systematic Review of Case ReportsNadial uzmahNo ratings yet
- Summer 2011Document16 pagesSummer 2011Marcus GibbsNo ratings yet