Download as pptx, pdf, or txt
You might also like
- Blood Disorders Seminar No 7Document142 pagesBlood Disorders Seminar No 7Hysum Mushtaq100% (2)
- Approach To Pale ChildDocument37 pagesApproach To Pale ChildsangheetaNo ratings yet
- Sickle Cell AnemiaDocument42 pagesSickle Cell Anemiaaafrah100% (2)
- Chapter 44: Nursing Care of The Client With An Hematologic DisordersDocument18 pagesChapter 44: Nursing Care of The Client With An Hematologic DisordersfLOR_ZIANE_MAENo ratings yet
- Lecture INST-100473 2023 08 05 10 30 19Document85 pagesLecture INST-100473 2023 08 05 10 30 19ashmangalNo ratings yet
- 260120200anemia in PregnancyDocument40 pages260120200anemia in Pregnancyraph faith100% (1)
- Hemolytic AnemiasDocument59 pagesHemolytic AnemiasRajesh darlingNo ratings yet
- Hematologic DisorderDocument16 pagesHematologic DisorderZoe DorothyNo ratings yet
- Hematological DisordersDocument45 pagesHematological Disordersbara.jarrar2001No ratings yet
- Hemoglobin Opa ThiesDocument11 pagesHemoglobin Opa ThiesprasasthiNo ratings yet
- Microcytic Normocytic and Macrocytic: by DR Hodan Jama 02/12/2017Document47 pagesMicrocytic Normocytic and Macrocytic: by DR Hodan Jama 02/12/2017Abdisalan hassanNo ratings yet
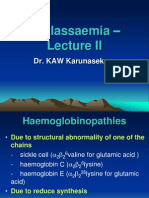
- Thalassaemia - : Dr. KAW KarunasekeraDocument36 pagesThalassaemia - : Dr. KAW KarunasekerarikarzNo ratings yet
- - تفسیر آزمایشات روتینDocument116 pages- تفسیر آزمایشات روتینrajabisamira8No ratings yet
- Sickle Cell DiseaseDocument26 pagesSickle Cell Diseaseinyanji.barasaNo ratings yet
- Neonatal HemopoeisisDocument22 pagesNeonatal HemopoeisisJaime BarraganNo ratings yet
- Cardiovascular System: Blood Heart Blood VesselsDocument56 pagesCardiovascular System: Blood Heart Blood VesselsTheophilus BaidooNo ratings yet
- Anemia-Dr Moses KazevuDocument86 pagesAnemia-Dr Moses KazevuMoses Jr KazevuNo ratings yet
- Blood Disorder in PregnancyDocument43 pagesBlood Disorder in PregnancyNadhrah zulkifliNo ratings yet
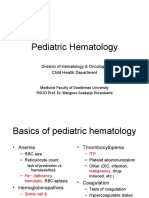
- Pediatric Hematology: Division of Hematology & Oncology Child Health DepartmentDocument37 pagesPediatric Hematology: Division of Hematology & Oncology Child Health DepartmentIsmail Satrio WibowoNo ratings yet
- 13.2 AnemiaDocument75 pages13.2 AnemiaMohammad AlrefaiNo ratings yet
- MBBS-4 No014090Document43 pagesMBBS-4 No014090diphylleia90grayiNo ratings yet
- Interpreting The CBC - When To ReferDocument44 pagesInterpreting The CBC - When To ReferKannan KannanNo ratings yet
- Anemia in PregnancyDocument18 pagesAnemia in Pregnancysaagiba100% (1)
- Abnormal HBDocument55 pagesAbnormal HBtofyNo ratings yet
- Blood Basics1Document6 pagesBlood Basics1Celina PastorNo ratings yet
- BloodDocument142 pagesBloodChelleyOllitroNo ratings yet
- Hemolytic Anemia-Pediatric MasterDocument62 pagesHemolytic Anemia-Pediatric MasterPedia 2020No ratings yet
- Thalassemia-Engleza NouDocument73 pagesThalassemia-Engleza NouDM XyzNo ratings yet
- Thalassemia SyndromesDocument29 pagesThalassemia SyndromesIsaac MwangiNo ratings yet
- Anemias&Leukemias 1Document80 pagesAnemias&Leukemias 1Fallen AngelNo ratings yet
- AnaemiaDocument71 pagesAnaemiaREETHUNo ratings yet
- Anemia Neonatus MhsDocument32 pagesAnemia Neonatus MhsTria100% (1)
- Anemia in ChildrenDocument34 pagesAnemia in ChildrensmpoojasubashNo ratings yet
- Laboratory Diagnosis of Anemia: by Dr. Ankita Pal Department of PathologyDocument43 pagesLaboratory Diagnosis of Anemia: by Dr. Ankita Pal Department of PathologyHimanshiNo ratings yet
- Hematology& Onco LectureDocument66 pagesHematology& Onco Lecturehasanatiya41No ratings yet
- Anemia in PregnancyDocument23 pagesAnemia in PregnancysuperjaxxxonNo ratings yet
- Hemolytic AnemiaDocument61 pagesHemolytic AnemiaMangayarkarasi ChandrakasanNo ratings yet
- Approach To Anemia: Bisrat DDocument45 pagesApproach To Anemia: Bisrat Dyared getachewNo ratings yet
- Sickle Cell Disease ManagementDocument23 pagesSickle Cell Disease ManagementAndrew SilungweNo ratings yet
- Sickle Cell AnemiaDocument29 pagesSickle Cell AnemiakademuhigiNo ratings yet
- Anaemias Due To Excessive Red Cell DestructionDocument20 pagesAnaemias Due To Excessive Red Cell DestructionzamadulaNo ratings yet
- CBC Arikod HoimaDocument37 pagesCBC Arikod Hoimadaniel arikodNo ratings yet
- Thalassemia Syndromes: Hematology-Oncology Division Pediatric Departement School of Medicine University of North SumateraDocument34 pagesThalassemia Syndromes: Hematology-Oncology Division Pediatric Departement School of Medicine University of North SumateraAbdusSomadNo ratings yet
- Abnormal CBC - PresentationDocument23 pagesAbnormal CBC - PresentationMateen ShukriNo ratings yet
- Anemia SDocument125 pagesAnemia SamirhsheikhiNo ratings yet
- HemogramDocument42 pagesHemogramTrung LêNo ratings yet
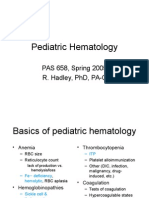
- Pediatric Hematology: Pas 658, Spring 2005 R. Hadley, PHD, Pa-CDocument34 pagesPediatric Hematology: Pas 658, Spring 2005 R. Hadley, PHD, Pa-CMateen ShukriNo ratings yet
- Approach To AnemiaDocument70 pagesApproach To AnemiaKidistNo ratings yet
- Heamatological Disorder: Disorder Related To Red Blood CellDocument12 pagesHeamatological Disorder: Disorder Related To Red Blood CellHelmiNo ratings yet
- Disampaikan Oleh: Dr. Ong Tjandra, MMPD., Spog (K)Document46 pagesDisampaikan Oleh: Dr. Ong Tjandra, MMPD., Spog (K)Asis muhammadNo ratings yet
- Anemia Anak 2: Dr. BerthaDocument35 pagesAnemia Anak 2: Dr. BerthaAriNo ratings yet
- Anaemias: P. Manyau School of Pharmacy University of ZimbabweDocument41 pagesAnaemias: P. Manyau School of Pharmacy University of Zimbabwebrian mgabiNo ratings yet
- Hematology 1Document64 pagesHematology 1Kervy Jay AgraviadorNo ratings yet
- RBC DisordersDocument49 pagesRBC DisordersGeraldine AgpesNo ratings yet
- Anaemia: Chan Sze Qi Chen Mi San Shafiq ZahariDocument63 pagesAnaemia: Chan Sze Qi Chen Mi San Shafiq ZahariRZ NgNo ratings yet
- Hemolytic Disease of The Fetus /newbornDocument46 pagesHemolytic Disease of The Fetus /newbornK.M.S. ChathunikaNo ratings yet
- Sickle Cell AnemiaDocument24 pagesSickle Cell Anemiacopy smartNo ratings yet
- Paroxysmal Nocturnal Hemoglobinuria, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandParoxysmal Nocturnal Hemoglobinuria, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Genetic Disorders: Biology Investigatory ProjectDocument15 pagesGenetic Disorders: Biology Investigatory ProjectAshwin ShajithNo ratings yet
- Psychological Problems Associated With Thalassemia in Diyala Province, Iraq - OdtDocument6 pagesPsychological Problems Associated With Thalassemia in Diyala Province, Iraq - OdtThe Swedish Journal of Scientific Research (SJSR) ISSN: 2001-9211No ratings yet
- RBC Disorder BcqsDocument68 pagesRBC Disorder BcqsMukhtiar AhmedNo ratings yet
- Sickle Cell Disease: Case StudyDocument22 pagesSickle Cell Disease: Case Studyapi-608465780No ratings yet
- HPLC Studies in HemoglobinopathiesDocument6 pagesHPLC Studies in HemoglobinopathiesDevi SusantiNo ratings yet
- Brochure HbA1c - Scientific - Discussion - Paper - AND - Variant - Study PDFDocument20 pagesBrochure HbA1c - Scientific - Discussion - Paper - AND - Variant - Study PDFNitin TiwariNo ratings yet
- Anthropometric Measurements in Children Having Transfusion Dependent Beta Thalassemia PDFDocument6 pagesAnthropometric Measurements in Children Having Transfusion Dependent Beta Thalassemia PDFMuthmainnah NihNo ratings yet
- Genetic LoadDocument20 pagesGenetic Loadmrdhar22No ratings yet
- AIPGMEE 2003 Question Paper With AnswerDocument59 pagesAIPGMEE 2003 Question Paper With AnswerpavaniNo ratings yet
- Pregnancy in Thalassemia Trait Carriers An Uneventful JourneyDocument4 pagesPregnancy in Thalassemia Trait Carriers An Uneventful JourneyHendry SusantoNo ratings yet
- Lesson 2 DiseasesDocument20 pagesLesson 2 DiseasesYzel Vasquez AdavanNo ratings yet
- Quiz PediatricsDocument56 pagesQuiz PediatricsMedShare87% (39)
- Supplementary Material: U Vi: C 1 1.1, P 6Document4 pagesSupplementary Material: U Vi: C 1 1.1, P 6himanshuNo ratings yet
- 4 Thalassemia 1Document20 pages4 Thalassemia 1Berlia NarayaniNo ratings yet
- Mendelian Disorder KrishnaDocument16 pagesMendelian Disorder KrishnaTanmay kalraNo ratings yet
- Sop For Thalassemia Screening Wwith NbsDocument11 pagesSop For Thalassemia Screening Wwith NbsUMMID WashimNo ratings yet
- A Study On Wheat Grass and Its Nutritional Value: January 2012Document10 pagesA Study On Wheat Grass and Its Nutritional Value: January 2012gurupreet singhNo ratings yet
- Thalassemia Disease: DefintionDocument6 pagesThalassemia Disease: DefintionyuddNo ratings yet
- Alpha Thalassemia TraitDocument12 pagesAlpha Thalassemia Traitdrtsotlhe mogolegwaNo ratings yet
- TH TH THDocument5 pagesTH TH THRomelu MartialNo ratings yet
- The Hemoglobin E Thalassemias: Correspondence: Grsfc@mahidol - Ac.thDocument15 pagesThe Hemoglobin E Thalassemias: Correspondence: Grsfc@mahidol - Ac.thDrAstha GuptaNo ratings yet
- Case Study Sickle CellDocument2 pagesCase Study Sickle CellAweGooseTreeNo ratings yet
- Presentasi Gen Letal (131109)Document38 pagesPresentasi Gen Letal (131109)Candace HillNo ratings yet
- 1 s2.0 S1658387617300602 MainDocument9 pages1 s2.0 S1658387617300602 MainFalisha Belvia KairinNo ratings yet
- Thalasemia RSCMDocument28 pagesThalasemia RSCMAnonymous ujOv31SNo ratings yet
- Nursing Care of Child With Thalassemia and LeukemiaDocument60 pagesNursing Care of Child With Thalassemia and LeukemiaJanicex FongNo ratings yet
- Classification of The Disorders of Hemoglobin: Bernard G. Forget and H. Franklin BunnDocument13 pagesClassification of The Disorders of Hemoglobin: Bernard G. Forget and H. Franklin BunnMade Oka HeryanaNo ratings yet
- PathophysiologyDocument137 pagesPathophysiologyAhmed S. Hamid0% (1)
- Prevalence of Hemoglobinosis in School Environments: Case of The City of Abengourou in Ivory CoastDocument6 pagesPrevalence of Hemoglobinosis in School Environments: Case of The City of Abengourou in Ivory CoastIJAR JOURNALNo ratings yet
- Journal 1Document13 pagesJournal 1Nur Ajiyanti 'anthi' SabirinaNo ratings yet