Download as pptx, pdf, or txt
You might also like
- Metacognitive Therapy For Generalized AnxietyDocument7 pagesMetacognitive Therapy For Generalized AnxietySergio Ignacio VaccaroNo ratings yet
- Open Reduction Internal Fixation PPT With Nursing ResponsibilitiesDocument13 pagesOpen Reduction Internal Fixation PPT With Nursing ResponsibilitiesMiciola Mitch Tanquiamco100% (2)
- TracheostomyDocument17 pagesTracheostomyCalimlim KimNo ratings yet
- TahbsoDocument4 pagesTahbsomichZ_13No ratings yet
- Colostomy CareDocument7 pagesColostomy CareChrismon Arek KeneNo ratings yet
- Colostomy CareDocument49 pagesColostomy Caregladz25100% (1)
- Colostomy ClassDocument24 pagesColostomy Classshahulkp100% (1)
- OstomyDocument22 pagesOstomyJosiah VillacampaNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Appendicitis (History & Examination)Document6 pagesAppendicitis (History & Examination)Doctor Saleem Rehman75% (4)
- Colostomy - Care - Module 2Document5 pagesColostomy - Care - Module 2Esmareldah Henry SirueNo ratings yet
- A Case Presentation On CholedocholithiasisDocument11 pagesA Case Presentation On CholedocholithiasisPaul Vincent EspereNo ratings yet
- Skin Grafting Surgical NursingDocument21 pagesSkin Grafting Surgical NursingHEMMA100% (1)
- Ostomy CareDocument13 pagesOstomy Carekyshb100% (1)
- HemorrhoidectomyDocument5 pagesHemorrhoidectomydrnareshkumar3281100% (1)
- Giving and Removing A Bedpan and Urinal DefinitionDocument4 pagesGiving and Removing A Bedpan and Urinal DefinitionFreisan ChenNo ratings yet
- Administering Anal SuppositoryDocument1 pageAdministering Anal SuppositorymichaelbenedictoNo ratings yet
- What Is Colonoscopy and Its PurposeDocument6 pagesWhat Is Colonoscopy and Its PurposeGrape JuiceNo ratings yet
- Surgical DressingDocument2 pagesSurgical Dressinggao1989No ratings yet
- Tracheostomy CareDocument4 pagesTracheostomy CareZar Ybañez MabanagNo ratings yet
- Barium EnemaDocument19 pagesBarium EnemaHamzeh Almasri100% (1)
- Barium SwallowDocument2 pagesBarium SwallowmameenNo ratings yet
- Gastric LavageDocument15 pagesGastric LavageEm BelandoNo ratings yet
- Gavage FedingDocument9 pagesGavage FedingGeetha ReddyNo ratings yet
- Sigmoidoscopy: Presented by Kriti Adhikari Roll No: 17Document38 pagesSigmoidoscopy: Presented by Kriti Adhikari Roll No: 17sushma shresthaNo ratings yet
- Nursing Care Plan For Inguinal Hernia HBDocument4 pagesNursing Care Plan For Inguinal Hernia HBdheeneshbabu0% (1)
- Assessment of GI SystemDocument40 pagesAssessment of GI SystemJeffRy SinyOe100% (1)
- Surgical TeamDocument9 pagesSurgical Teamkarenkaren09No ratings yet
- Positioning and Draping The PatientDocument4 pagesPositioning and Draping The PatientNazire Luis Colita YandugNo ratings yet
- Colostomy CareDocument8 pagesColostomy CareAhmed Hamed100% (2)
- Gastrostomy FeedingDocument9 pagesGastrostomy FeedingJamie Luz Tongco0% (1)
- Colostomy Care ChecklistDocument5 pagesColostomy Care ChecklistLynette JavaNo ratings yet
- Colostomy IrrigationDocument3 pagesColostomy IrrigationJikko Verra GarciaNo ratings yet
- MSN Ii - 24.6.2020 An-Tonsillitis and AdenoiditisDocument41 pagesMSN Ii - 24.6.2020 An-Tonsillitis and AdenoiditisYAMINIPRIYANNo ratings yet
- PeritonitisDocument22 pagesPeritonitisBobby Faisyal Rakhman100% (1)
- Colostomy CareDocument6 pagesColostomy CareLoren Sales ReyesNo ratings yet
- Tracheostomy CareDocument4 pagesTracheostomy CareEriel Custodio Quijada100% (2)
- Procedure Checklist Chapter 27: Inserting An Indwelling Urinary Catheter (Male)Document4 pagesProcedure Checklist Chapter 27: Inserting An Indwelling Urinary Catheter (Male)jths100% (1)
- Indirect Inguinal HerniaDocument54 pagesIndirect Inguinal HerniaYlamher Bufi Imperial100% (1)
- Assisting in Application of Plaster of ParisDocument2 pagesAssisting in Application of Plaster of ParisGopi RajNo ratings yet
- Colostomy Care & IrrigationDocument18 pagesColostomy Care & Irrigationpbatongbakal100% (2)
- Hemorrhoids: Presented By-Stuti Rastogi BSC Nursing 2 YearDocument25 pagesHemorrhoids: Presented By-Stuti Rastogi BSC Nursing 2 YearStuti RastogiNo ratings yet
- Nasogastric Feeding ProcedureDocument20 pagesNasogastric Feeding ProcedureKrishna Sonu SoniNo ratings yet
- Fistulectomy: - Prepared byDocument65 pagesFistulectomy: - Prepared byMonette Abalos MendovaNo ratings yet
- Liver Biopsy and AbdominalDocument25 pagesLiver Biopsy and AbdominalAfiq Mubasyyir AmranNo ratings yet
- NCP Acute-PainDocument4 pagesNCP Acute-PainMarie CatapiaNo ratings yet
- Assisting With Lumbar PunctureDocument4 pagesAssisting With Lumbar PuncturePhelanCoy100% (1)
- SuctioningDocument30 pagesSuctioningbajaoc60% (5)
- Leopold S ManeuverDocument5 pagesLeopold S Maneuverastak ghisingNo ratings yet
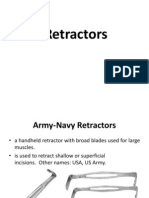
- RetractorsDocument18 pagesRetractorsNicole SooNo ratings yet
- Colostomy Care PDFDocument18 pagesColostomy Care PDFcayla mae carlosNo ratings yet
- Types of AnesthesiaDocument6 pagesTypes of AnesthesiaEnrick CastroNo ratings yet
- 13 Surgery (Perioperative Client) Nursing Care Plans - NurseslabsDocument31 pages13 Surgery (Perioperative Client) Nursing Care Plans - NurseslabsRena SafitriNo ratings yet
- Purpose of The LaryngosDocument13 pagesPurpose of The LaryngosdessriyaNo ratings yet
- Tracheostomy CareDocument1 pageTracheostomy CareShreyas WalvekarNo ratings yet
- NSO Gastric LavageDocument3 pagesNSO Gastric Lavagetry dokkNo ratings yet
- Appendectomy O.R. Write UpDocument11 pagesAppendectomy O.R. Write UpJessica Christine Datuin GustiloNo ratings yet
- Mixed HemorrhoidsDocument4 pagesMixed HemorrhoidsHerne BalberdeNo ratings yet
- AADocument20 pagesAAAiyaz AliNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Colostomy Care: Sital B Sharma MSC Nursing Part I Con, NBMCDocument39 pagesColostomy Care: Sital B Sharma MSC Nursing Part I Con, NBMCShetal Sharma100% (1)
- Hyperosmolar Hyperglycemic Nonketotic Syndrome HHNSDocument12 pagesHyperosmolar Hyperglycemic Nonketotic Syndrome HHNSKyle Ü D. CunanersNo ratings yet
- Epilepsy / Seizures: Roche'e Aguarin BSN - IiiDocument31 pagesEpilepsy / Seizures: Roche'e Aguarin BSN - IiiKyle Ü D. CunanersNo ratings yet
- Glaucoma Oral RevalidaDocument11 pagesGlaucoma Oral RevalidaKyle Ü D. CunanersNo ratings yet
- Ulcerative ColitisDocument18 pagesUlcerative ColitisKyle Ü D. CunanersNo ratings yet
- Path o PhysiologyDocument9 pagesPath o PhysiologyKyle Ü D. CunanersNo ratings yet
- Cva Vs BleedDocument30 pagesCva Vs BleedKyle Ü D. CunanersNo ratings yet
- NCP - Psychiatric SettingDocument20 pagesNCP - Psychiatric SettingKyle Ü D. CunanersNo ratings yet
- Chronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisDocument6 pagesChronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisKyle Ü D. CunanersNo ratings yet
- Drug StudyDocument20 pagesDrug StudyKyle Ü D. CunanersNo ratings yet
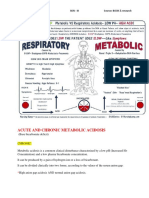
- Acute and Chronic Metabolic Acidosis: Amada, Kevin Moor N. BSN - Iii Source: BOOK & ResearchDocument10 pagesAcute and Chronic Metabolic Acidosis: Amada, Kevin Moor N. BSN - Iii Source: BOOK & ResearchKyle Ü D. CunanersNo ratings yet
- PriorDocument1 pagePriorKyle Ü D. CunanersNo ratings yet
- Table 1. 24 Hours Food Diary Breakfast Number of Serving Kcal CHO Fats ChonDocument1 pageTable 1. 24 Hours Food Diary Breakfast Number of Serving Kcal CHO Fats ChonKyle Ü D. CunanersNo ratings yet
- New Jersey State Sanitary Code Body Art Procedures N.J.A.C. 8:27-1 ET SEQDocument18 pagesNew Jersey State Sanitary Code Body Art Procedures N.J.A.C. 8:27-1 ET SEQpippo07No ratings yet
- Fosfomycin: Review and Use Criteria BackgroundDocument12 pagesFosfomycin: Review and Use Criteria BackgroundAbu Azzam Al-Hadi100% (1)
- Group 3 - DettolDocument37 pagesGroup 3 - DettolSubrata MondalNo ratings yet
- F2F Forms Grade LevelDocument7 pagesF2F Forms Grade LevelJAHYRAH BARTOLOMENo ratings yet
- Practice Guidelines For Tumor Marker Use in The Clinic: Catharine SturgeonDocument9 pagesPractice Guidelines For Tumor Marker Use in The Clinic: Catharine SturgeonYder AtrupNo ratings yet
- Physical Therapy For A Child With Encopresis: A Case ReportDocument8 pagesPhysical Therapy For A Child With Encopresis: A Case ReportChiara GaleazziNo ratings yet
- Roles & Functions of Community Health NurseDocument9 pagesRoles & Functions of Community Health NurseJan Jewey33% (3)
- Why Kids Need DirtDocument5 pagesWhy Kids Need DirtViraj Shelke100% (1)
- BAB 3 (1-6) Play and Social Skills For Children With Autism Spectrum Disorder (PDFDrive)Document6 pagesBAB 3 (1-6) Play and Social Skills For Children With Autism Spectrum Disorder (PDFDrive)Jiminel HereNo ratings yet
- Hindustan Times Delhi 21 - 6Document44 pagesHindustan Times Delhi 21 - 6Hmbe hmbeNo ratings yet
- Cle2018 Industrial-wastes-treatment-And-disposalDocument2 pagesCle2018 Industrial-wastes-treatment-And-disposalSuraj SainiNo ratings yet
- Positive Peace Implementation GuideDocument14 pagesPositive Peace Implementation GuideRawalpindi Arts CouncilNo ratings yet
- DanielsTables3!00!00 2Document7 pagesDanielsTables3!00!00 2Penelope Pancho Fangio Perez PandoNo ratings yet
- 127-Manuscript (Title, Abstract, Introduction, Materials and Methods, Etc.) - 516-1-10-20200814 PDFDocument10 pages127-Manuscript (Title, Abstract, Introduction, Materials and Methods, Etc.) - 516-1-10-20200814 PDFhayascent hilarioNo ratings yet
- Comparative Analysis of Lunge Techniques: Forward, Reverse, Walking LungeDocument4 pagesComparative Analysis of Lunge Techniques: Forward, Reverse, Walking LungeWaldir Martins NetoNo ratings yet
- Short Essay On The Pros/cons of VaccinationDocument3 pagesShort Essay On The Pros/cons of Vaccinationwendyy67% (3)
- Micro Teaching On Intestinal Obstruction: School of Nursing Science and Research Sharda UniversityDocument21 pagesMicro Teaching On Intestinal Obstruction: School of Nursing Science and Research Sharda UniversityRohan SahuNo ratings yet
- Proximal Humerus and Humeral Shaft Fractures in Children: M. Wade Shrader, MDDocument5 pagesProximal Humerus and Humeral Shaft Fractures in Children: M. Wade Shrader, MDRoyman MejiaNo ratings yet
- Safety Training FormatsDocument11 pagesSafety Training FormatsAsan IbrahimNo ratings yet
- Craft Certificate in Business ManagementDocument2 pagesCraft Certificate in Business ManagementChristine KendiNo ratings yet
- Diseases of Major Pulse Crops in Pakistan-A Review: Tropical Pest ManagementDocument8 pagesDiseases of Major Pulse Crops in Pakistan-A Review: Tropical Pest Managementদিবা স্বপ্নচারীNo ratings yet
- ECT Electroconvulsive Therapy Fact SheetDocument4 pagesECT Electroconvulsive Therapy Fact SheetSonali DakhoreNo ratings yet
- Ear Surgery: Tympanoplasty, Mastoidectomy: Patient Postoperative Instructions and InformationDocument4 pagesEar Surgery: Tympanoplasty, Mastoidectomy: Patient Postoperative Instructions and InformationPaul Jordan SandaloNo ratings yet
- Testo Alpha ExDocument2 pagesTesto Alpha Extesto alphaexNo ratings yet
- IPM Presentation 010312 FINALDocument17 pagesIPM Presentation 010312 FINALTerri BimmNo ratings yet
- Pengujian Toleransi Mangrove Muda Terhadap Cemaran Minyak BumiDocument7 pagesPengujian Toleransi Mangrove Muda Terhadap Cemaran Minyak BumiAmando DoloksaribuNo ratings yet
- Pit AstidDocument12 pagesPit AstidAstidya GobelNo ratings yet
- m106 Report Competencies of Midwifery PracticeDocument71 pagesm106 Report Competencies of Midwifery PracticeTresiah LozanoNo ratings yet
- Materia Medica Revision - Allen's Keynotes & BoerickDocument11 pagesMateria Medica Revision - Allen's Keynotes & Boerickssrkm guptaNo ratings yet