Download as pptx, pdf, or txt
You might also like
- SCIENCE-REPORT-GROUP-2.pdf 20240211 212133 0000Document48 pagesSCIENCE-REPORT-GROUP-2.pdf 20240211 212133 0000taishishiroganeNo ratings yet
- A-Z Booklet Nature Sunshine 2014Document126 pagesA-Z Booklet Nature Sunshine 2014api-244390023100% (1)
- Medicine History and CounsellingDocument13 pagesMedicine History and Counsellingpranjl100% (1)
- The Body Remembers - Babette RothschildDocument221 pagesThe Body Remembers - Babette RothschildBojana100% (2)
- Conn's SyndromeDocument10 pagesConn's SyndromeFathanah Yanti MphNo ratings yet
- Endocrine DisordersDocument5 pagesEndocrine DisordersBilly Ray VillanuevaNo ratings yet
- A Disease Study of Cushing's DiseaseDocument13 pagesA Disease Study of Cushing's DiseaseKristine AlejandroNo ratings yet
- Assignment 4Document8 pagesAssignment 4api-328441669100% (1)
- Surgery History TakingDocument18 pagesSurgery History Takingpranjl100% (2)
- Lecture Notes ENTDocument190 pagesLecture Notes ENTKamar Fletcher100% (3)
- Cushing'S Syndrome: Roldan, Scorch Dominique Romero, John Reden Sanchez, Tracy JoyDocument25 pagesCushing'S Syndrome: Roldan, Scorch Dominique Romero, John Reden Sanchez, Tracy JoyGerald John PazNo ratings yet
- Cushings Syndrome and Addison Disease - BPTDocument45 pagesCushings Syndrome and Addison Disease - BPTAanchal GuptaNo ratings yet
- Cushing's SyndromeDocument24 pagesCushing's SyndromeUdtjeVanDerJeyk100% (1)
- NCM116 Addison DiseaseDocument20 pagesNCM116 Addison DiseaseSofia MikaelaNo ratings yet
- Cushing SyndromeDocument5 pagesCushing SyndromeRosa Yulise PutriNo ratings yet
- A Simple Guide to Hyperaldosteronism, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hyperaldosteronism, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Cushing DiseaseDocument70 pagesCushing Diseaseاحمد المصرىNo ratings yet
- Endocrine 1.2 CushingDocument7 pagesEndocrine 1.2 CushingJem QuintoNo ratings yet
- Cushing's SyndromeDocument35 pagesCushing's SyndromeYoga KarsendaNo ratings yet
- Patho Cushing's SyndromeDocument13 pagesPatho Cushing's SyndromeAnnie Christine Rivera100% (1)
- Empty Sella SyndromeDocument2 pagesEmpty Sella Syndromewawan_291289100% (1)
- Course 4 2019 Hypoglicemia HyperuricemiaDocument57 pagesCourse 4 2019 Hypoglicemia HyperuricemiaAmelia PricopNo ratings yet
- HYPERTHYROIDISMDocument40 pagesHYPERTHYROIDISMEmmanuelNo ratings yet
- Sickle Cell DiseaseDocument23 pagesSickle Cell Diseasealejandrino_leoaugusto100% (1)
- Addison's DiseaseDocument9 pagesAddison's Diseaseash ashNo ratings yet
- Pharma Katzung - AlcoholsDocument5 pagesPharma Katzung - AlcoholsJoshua RemonNo ratings yet
- Thyroid Disease (Chan)Document29 pagesThyroid Disease (Chan)Sidiq AboobakerNo ratings yet
- Hyporeninemic HypoaldosteronismDocument12 pagesHyporeninemic HypoaldosteronismCésar Augusto Sánchez SolisNo ratings yet
- Myocardialinfarction 150223043527 Conversion Gate02 PDFDocument22 pagesMyocardialinfarction 150223043527 Conversion Gate02 PDFBhavika Aggarwal100% (1)
- Hypothyroidism: Causes, Incidence, and Risk FactorsDocument5 pagesHypothyroidism: Causes, Incidence, and Risk FactorsPhineas KangoreNo ratings yet
- Patho Final Study GuideDocument55 pagesPatho Final Study GuideBritNo ratings yet
- (MED1) 3.04 Approach To Hypertension (Dr. Bago-Azares)Document11 pages(MED1) 3.04 Approach To Hypertension (Dr. Bago-Azares)NoreenNo ratings yet
- Alzheimer Disease: Petra Nowotny, Jennifer M Kwon, Alison M GoateDocument6 pagesAlzheimer Disease: Petra Nowotny, Jennifer M Kwon, Alison M GoatedineshhissarNo ratings yet
- Hypothyroidism: Darien Liew DaojuinDocument41 pagesHypothyroidism: Darien Liew DaojuinDarien LiewNo ratings yet
- Addisonian Crisis: Manish K Medical Officer IgmhDocument47 pagesAddisonian Crisis: Manish K Medical Officer IgmhNaaz Delhiwale100% (1)
- Acromegal Y: Dr. Kushal Markanday Senior Resident Department of General Medicine MVJMC & RHDocument69 pagesAcromegal Y: Dr. Kushal Markanday Senior Resident Department of General Medicine MVJMC & RH966342No ratings yet
- Pa Tho Physiology of CushingDocument4 pagesPa Tho Physiology of CushingLouise RojoNo ratings yet
- Cushing SyndromeDocument19 pagesCushing SyndromerituNo ratings yet
- Luteinizing HormoneDocument8 pagesLuteinizing HormoneSaba MalikNo ratings yet
- PheochromocytomaDocument43 pagesPheochromocytomaJason MirasolNo ratings yet
- Hypopituitarism - ThomasDocument40 pagesHypopituitarism - Thomasguidance100% (1)
- Cushings DiseaseDocument17 pagesCushings Diseaserightspeaker22No ratings yet
- Cushing's SyndromeDocument25 pagesCushing's SyndromeRahmah Shah BahaiNo ratings yet
- Patho DiagramDocument1 pagePatho Diagrampaupaulala100% (2)
- Alzheimer's DiseaseDocument19 pagesAlzheimer's DiseaseMission JupiterNo ratings yet
- Endocrine System: THE Adrenal GlandsDocument50 pagesEndocrine System: THE Adrenal GlandsAbdel Aziz NazihNo ratings yet
- Cushing's SyndromeDocument25 pagesCushing's SyndromeRose Ann Del MundoNo ratings yet
- Sheehan SyndromeDocument6 pagesSheehan SyndromeArvie TagnongNo ratings yet
- Celiac DiseaseDocument2 pagesCeliac DiseaseGiabellNo ratings yet
- Adrenal DisordersDocument29 pagesAdrenal DisordersSuliman Garalleh100% (1)
- Pituitary DisordersDocument65 pagesPituitary Disordersgema disiyuna100% (2)
- Common Metabolic DisordersDocument7 pagesCommon Metabolic DisordersDevika RajNo ratings yet
- 1-Adrenocorticosteroids Chapter39Document94 pages1-Adrenocorticosteroids Chapter39hamidNo ratings yet
- Pathology of Thyroid DiseasesDocument5 pagesPathology of Thyroid DiseasesNur Kamalia KamalNo ratings yet
- Addison 'S Disea Se: Layne A BreuDocument8 pagesAddison 'S Disea Se: Layne A Breudavelnx2291No ratings yet
- 2 Diabetes Mellitus and DiagnosticDocument33 pages2 Diabetes Mellitus and DiagnosticSifa RismawatiNo ratings yet
- Hyperthyroidism and HypothyroidismDocument28 pagesHyperthyroidism and HypothyroidismAlthea AlbaniaNo ratings yet
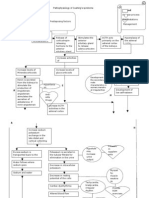
- Approach To Unconscious PatientDocument23 pagesApproach To Unconscious Patienttantw880% (1)
- By: DR Eyad Talal: Moderator: DR I - QudaisatDocument55 pagesBy: DR Eyad Talal: Moderator: DR I - QudaisatEyad AbdeljawadNo ratings yet
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいNo ratings yet
- Parathyroid GlandDocument3 pagesParathyroid GlandElla OrtegaNo ratings yet
- Adrenal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAdrenal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (1)
- A Simple Guide to Thyroiditis, Diagnosis, Treatment and Related DisordersFrom EverandA Simple Guide to Thyroiditis, Diagnosis, Treatment and Related DisordersNo ratings yet
- A Simple Guide to the Adrenal Gland and Its Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to the Adrenal Gland and Its Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Differential DiagnosisDocument41 pagesDifferential Diagnosispranjl100% (2)
- Throwers 10Document7 pagesThrowers 10pranjlNo ratings yet
- Antibiotics Quick ReviewDocument5 pagesAntibiotics Quick Reviewpranjl100% (5)
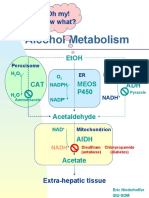
- Alcohol Metabolism: Oh My! Now What?Document5 pagesAlcohol Metabolism: Oh My! Now What?pranjlNo ratings yet
- Prolonged and Postterm Pregnancy: Roxane Rampersad and George A. MaconesDocument7 pagesProlonged and Postterm Pregnancy: Roxane Rampersad and George A. MaconesAphreLbecasean WaeNo ratings yet
- Time and Memory)Document340 pagesTime and Memory)gustavoalbertomaseraNo ratings yet
- Clinical Chemistry: Presented By: Haya Mansour SLLE Exam 2022Document61 pagesClinical Chemistry: Presented By: Haya Mansour SLLE Exam 2022apdlh 99No ratings yet
- Teaching Internal Medicine Pearls On The WardsDocument212 pagesTeaching Internal Medicine Pearls On The WardsAnonymous ZeqcLl100% (10)
- Biology Lecture 5 Hormone ChartDocument2 pagesBiology Lecture 5 Hormone Chartmark_pedersen_6No ratings yet
- Avoiding Burnout and Severe Stress: Guidelines For The Helping ProfessionalsDocument44 pagesAvoiding Burnout and Severe Stress: Guidelines For The Helping ProfessionalsChiriac Ionut IlieNo ratings yet
- Hypo Glice MiaDocument13 pagesHypo Glice MiaNurul AmaliaNo ratings yet
- Quiz LetDocument16 pagesQuiz LetMohamed Y AbdallahNo ratings yet
- Precosious Puberty Case StudyDocument27 pagesPrecosious Puberty Case Studynishavohreh100% (1)
- The Role of Hormone in ParturitionDocument36 pagesThe Role of Hormone in ParturitionDiana HayatiNo ratings yet
- The Effects of Stress On Short-Term and Long-Term MemoryDocument12 pagesThe Effects of Stress On Short-Term and Long-Term MemoryCarmen MihalachiNo ratings yet
- AACE Abstracts 2019 Los AngelesDocument357 pagesAACE Abstracts 2019 Los Angelesmimran1974No ratings yet
- Lets Talk About HealthDocument66 pagesLets Talk About HealthGigel FroneNo ratings yet
- Hormonal Responses To Exercise-1Document48 pagesHormonal Responses To Exercise-1CHANGEZ KHAN SARDARNo ratings yet
- Unit 5 Stress Management: ObjectivesDocument13 pagesUnit 5 Stress Management: ObjectivesSanjay shuklaNo ratings yet
- Endocrine 1 PageDocument3 pagesEndocrine 1 PagetimbitNo ratings yet
- Human Reproduction - DPP 10 (Of Lecture 14) - Lakshya NEET 2024Document3 pagesHuman Reproduction - DPP 10 (Of Lecture 14) - Lakshya NEET 2024Ankit BhartiNo ratings yet
- Adrenal Fatigue Symptoms Diet Remedies - DR AxeDocument38 pagesAdrenal Fatigue Symptoms Diet Remedies - DR AxeSu H Harthy50% (2)
- Malschitzky 2015Document5 pagesMalschitzky 2015maria vitoria saldanhaNo ratings yet
- Clinical Biochemistry Lecture NotesDocument55 pagesClinical Biochemistry Lecture Notesms.biwottNo ratings yet
- A4 Metabolic and EndocrineDocument50 pagesA4 Metabolic and Endocrinemineb9631No ratings yet
- Multiple Organ Dysfunction SyndromeDocument4 pagesMultiple Organ Dysfunction SyndromeJenny SisonNo ratings yet
- Antidepressant Physical Adverse ReactionsDocument110 pagesAntidepressant Physical Adverse ReactionsanntjitNo ratings yet
- EndocrineDocument2 pagesEndocrineHoney Mie MorenoNo ratings yet
- Testosterone Hacker Handbook 2-0 PDFDocument41 pagesTestosterone Hacker Handbook 2-0 PDFKevin100% (2)
- Cushing's SyndromeDocument2 pagesCushing's SyndromeKuan NgNo ratings yet
- Summery of Htma Theresa - VernonDocument5 pagesSummery of Htma Theresa - Vernonsisi marxNo ratings yet
- The Inmuen Response To Surgery and TraumaDocument8 pagesThe Inmuen Response To Surgery and TraumaCorin Boice TelloNo ratings yet