Download as ppt, pdf, or txt
You might also like
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Methods in Malaria Research-6th EditionDocument499 pagesMethods in Malaria Research-6th EditionAlirea BaharvandNo ratings yet
- Torch Infection in Pregnancy: Neha Barari Assistant Professor SNSRDocument44 pagesTorch Infection in Pregnancy: Neha Barari Assistant Professor SNSRBhawna JoshiNo ratings yet
- ToxoplasmosisDocument12 pagesToxoplasmosisaltabeb hasoon100% (2)
- Torch Infection: Reporter: Zhao Meiling (Alice) Date: April.10.2019Document35 pagesTorch Infection: Reporter: Zhao Meiling (Alice) Date: April.10.2019Hilary WangNo ratings yet
- 24.11.09 PPT On Intrauterine InfectionDocument57 pages24.11.09 PPT On Intrauterine InfectionDhara Meena90% (10)
- Senin 20 Oktober 2014 - Parasit 1 - Parasitologi - Toxoplasma - 12Document32 pagesSenin 20 Oktober 2014 - Parasit 1 - Parasitologi - Toxoplasma - 12Zahra AstriantaniNo ratings yet
- Slide - K-21-22 Patogenesis Dan Diagnosis Parasit OportunistikDocument69 pagesSlide - K-21-22 Patogenesis Dan Diagnosis Parasit OportunistikFaisal AlhasNo ratings yet
- Diagnosis: Neglected Parasitic Infections DPDXDocument11 pagesDiagnosis: Neglected Parasitic Infections DPDXSani Widya FirnandaNo ratings yet
- ToxoplasmosisDocument0 pagesToxoplasmosisAhmad Badrul AminNo ratings yet
- Tokso (Neuro)Document38 pagesTokso (Neuro)ninda karisaNo ratings yet
- Toxoplasma GondiiDocument6 pagesToxoplasma GondiiSyawal HariadiNo ratings yet
- Part 1 ProtozoaDocument111 pagesPart 1 ProtozoaDiana Joyce MabborangNo ratings yet
- Congenital ToxoplasmosisDocument26 pagesCongenital ToxoplasmosisMichael WijayaNo ratings yet
- 10 - Torch Pads KehamilanDocument43 pages10 - Torch Pads KehamilanMuhammad LutfiNo ratings yet
- ParasitosisCongenitas Eq2Document11 pagesParasitosisCongenitas Eq2Samanta OtapaNo ratings yet
- Toxoplasma Gondii (2003)Document41 pagesToxoplasma Gondii (2003)Rodrigo Simões MarquesNo ratings yet
- Gynecological Disorders in Pregnanacy FinalDocument62 pagesGynecological Disorders in Pregnanacy Finalsanthiyasandy100% (3)
- Infeksi in Pregnancy and PuerperiumDocument35 pagesInfeksi in Pregnancy and PuerperiumGerarld Immanuel KairupanNo ratings yet
- Para Handout - Coccidia - ToxoplasmaDocument15 pagesPara Handout - Coccidia - ToxoplasmaDerick SemNo ratings yet
- Toxoplasmosis PowerPointDocument31 pagesToxoplasmosis PowerPointاحمد الفضلNo ratings yet
- Toxoplasma GondiiDocument21 pagesToxoplasma GondiiIlac Tristan BernardoNo ratings yet
- Feco-Orally Transmitted Diseases: (Diseases Transmitted by Contaminated Water, Food, and Others)Document133 pagesFeco-Orally Transmitted Diseases: (Diseases Transmitted by Contaminated Water, Food, and Others)TekletsadikNo ratings yet
- 13 ToxoplasmosisDocument10 pages13 ToxoplasmosisAboubakar Moalim Mahad moh'dNo ratings yet
- 3.torch InfectionsDocument15 pages3.torch InfectionsKuleshwar SahuNo ratings yet
- Torch: Diana Khoirun Nida - 1710211042Document34 pagesTorch: Diana Khoirun Nida - 1710211042Diana Khoirun NidaNo ratings yet
- Genera:: Treponema & BorreiliaDocument25 pagesGenera:: Treponema & BorreiliaKhalifa Sifaw Ghenghesh100% (1)
- Toxoplasma and RubellaDocument37 pagesToxoplasma and RubellaHervi LaksariNo ratings yet
- Congenital Toxoplasmosis Treatment: D. Serranti, D. Buonsenso, P. ValentiniDocument6 pagesCongenital Toxoplasmosis Treatment: D. Serranti, D. Buonsenso, P. ValentiniAndra KurniantoNo ratings yet
- Tropmed 2 Malaria: Alterations of The Host Cells: 1. A Visible Change of Shape and ReducedDocument7 pagesTropmed 2 Malaria: Alterations of The Host Cells: 1. A Visible Change of Shape and Reduced玮雁No ratings yet
- Leptospirosis: Divisi Penyakit Tropik Dan Infeksi Departemen Penyakit Dalam FK USU/RSU HAMDocument20 pagesLeptospirosis: Divisi Penyakit Tropik Dan Infeksi Departemen Penyakit Dalam FK USU/RSU HAMJoice RumondangNo ratings yet
- Epidemiology & Risk Factors: ProtozoanDocument5 pagesEpidemiology & Risk Factors: Protozoanmilind_vetyNo ratings yet
- Lecture Parasites in Immunocompromised PatientDocument50 pagesLecture Parasites in Immunocompromised PatientalgutNo ratings yet
- Diseases PIDSRDocument25 pagesDiseases PIDSRaringkinking100% (1)
- HGJK J LHB, JKDocument4 pagesHGJK J LHB, JKChandra Noor RachmanNo ratings yet
- 15 Virusne Infekcije U Trudnoci - PrevedenoDocument7 pages15 Virusne Infekcije U Trudnoci - PrevedenoVelibor StankovićNo ratings yet
- Enteric FeverDocument7 pagesEnteric FeverkudzaimuregidubeNo ratings yet
- RB - Petersen. Toxoplasmosis, UpToDate, 2019Document12 pagesRB - Petersen. Toxoplasmosis, UpToDate, 2019GuilhermeNo ratings yet
- Toxoplasmosis: Acute Systemic DiseaseDocument13 pagesToxoplasmosis: Acute Systemic DiseaseClaudia NovitayantiNo ratings yet
- Listeriosis: Monocytogenes, Has Recently Been Recognized AsDocument30 pagesListeriosis: Monocytogenes, Has Recently Been Recognized AsJoanna CabildoNo ratings yet
- Slide 1 STIDocument50 pagesSlide 1 STIMatth N. ErejerNo ratings yet
- 5.toxoplasmosis (Rev 03.16)Document21 pages5.toxoplasmosis (Rev 03.16)maya dwiNo ratings yet
- Protozoa 2Document4 pagesProtozoa 2Farhat KhanNo ratings yet
- Neisseria Gonorrhoeae, Sometimes Called The: I. DefinitionDocument16 pagesNeisseria Gonorrhoeae, Sometimes Called The: I. DefinitionBerle Joy VillanuevaNo ratings yet
- Infections in Pregnancy & NewbornDocument70 pagesInfections in Pregnancy & NewbornmbbsclerkingNo ratings yet
- Identification and Classification of Neonate With InfectionsDocument62 pagesIdentification and Classification of Neonate With Infectionsvisuinsvu100% (7)
- SyphillsDocument18 pagesSyphillsped medNo ratings yet
- Toxoplasma y Citomehalovirus PDFDocument12 pagesToxoplasma y Citomehalovirus PDFGUSTAVO ANDRES NORENA LOPEZNo ratings yet
- Factsheet Toxoplasmosis enDocument2 pagesFactsheet Toxoplasmosis enSunil YadavNo ratings yet
- Typhoid Fever: Divisi Tropik Dan Infeksi Bag/Smf - Ilmu Penyakit Dalam FK Unsyiah Rsud. Dr. Zainoel Abidin Banda AcehDocument23 pagesTyphoid Fever: Divisi Tropik Dan Infeksi Bag/Smf - Ilmu Penyakit Dalam FK Unsyiah Rsud. Dr. Zainoel Abidin Banda Acehandreva8No ratings yet
- Leptospirosis in ChildrenDocument5 pagesLeptospirosis in ChildrenPramod KumarNo ratings yet
- Vaccine PreventableDocument89 pagesVaccine PreventableMohammad Doctor CabdiraxmanNo ratings yet
- Life Cycle of Toxoplasma Gondii. Source: Wikimedia Commons Author: Ladyofhats (2010)Document3 pagesLife Cycle of Toxoplasma Gondii. Source: Wikimedia Commons Author: Ladyofhats (2010)Friets KatuukNo ratings yet
- BrucellaDocument10 pagesBrucellanuhahamdyNo ratings yet
- Neglected Parasitic Infections in The United States: ToxoplasmosisDocument6 pagesNeglected Parasitic Infections in The United States: ToxoplasmosispamepomeNo ratings yet
- Torch: Jessica Santoso Moderator: Dr. Maimun ZA, M.Kes, SP - PKDocument79 pagesTorch: Jessica Santoso Moderator: Dr. Maimun ZA, M.Kes, SP - PKTommy KristantoNo ratings yet
- Brucellosis in NepalDocument22 pagesBrucellosis in NepalBinayaNo ratings yet
- TORCH Infection in Pregnant Women Ver September 2017 PDFDocument9 pagesTORCH Infection in Pregnant Women Ver September 2017 PDFRevina AmaliaNo ratings yet
- Zoonotic Diseases: by Rita NkiroteDocument44 pagesZoonotic Diseases: by Rita NkiroteIsaac JumaNo ratings yet
- Female Urinary Tract Infections in Clinical PracticeFrom EverandFemale Urinary Tract Infections in Clinical PracticeBob YangNo ratings yet
- The Infection Game Supplement: new infections, retroviruses and pandemicsFrom EverandThe Infection Game Supplement: new infections, retroviruses and pandemicsNo ratings yet
- Department of Child Health Udayana University Medical School / Sanglah Hospital DenpasarDocument11 pagesDepartment of Child Health Udayana University Medical School / Sanglah Hospital Denpasarmember12dNo ratings yet
- JR Fer IyaDocument18 pagesJR Fer Iyamember12dNo ratings yet
- Pre-Eclampsia Is A Valuable Opportunity To Diagnose Chronic Kidney Disease - A Multicentre StudyDocument11 pagesPre-Eclampsia Is A Valuable Opportunity To Diagnose Chronic Kidney Disease - A Multicentre Studymember12dNo ratings yet
- Peer Review Jurnal Third Stage of Labor - Evidence Based Practice For Prevention of Adverse Maternal and Neonatal OutcomesDocument3 pagesPeer Review Jurnal Third Stage of Labor - Evidence Based Practice For Prevention of Adverse Maternal and Neonatal Outcomesmember12dNo ratings yet
- Vitamin D Deficiency and Gestational Diabetes Mellitus in Relation To Body Mass IndexDocument10 pagesVitamin D Deficiency and Gestational Diabetes Mellitus in Relation To Body Mass Indexmember12dNo ratings yet
- Steroids, Steroid Associated Substances, and Gestational Diabetes MellitusDocument18 pagesSteroids, Steroid Associated Substances, and Gestational Diabetes Mellitusmember12dNo ratings yet
- Factors Affecting Use of Magnesium Sulphate For Pre-Eclampsia or Eclampsia - A Qualitative Evidence SynthesisDocument13 pagesFactors Affecting Use of Magnesium Sulphate For Pre-Eclampsia or Eclampsia - A Qualitative Evidence Synthesismember12dNo ratings yet
- Dietary Factors That Affect The Risk of Pre-EclampsiaDocument16 pagesDietary Factors That Affect The Risk of Pre-Eclampsiamember12dNo ratings yet
- Patient Recapitulation Delivery Room ReportDocument2 pagesPatient Recapitulation Delivery Room Reportmember12dNo ratings yet
- Depression Is A Serious Mental Health ProblemDocument2 pagesDepression Is A Serious Mental Health Problemmember12dNo ratings yet
- Mola Hidatidosa JESDocument24 pagesMola Hidatidosa JESmember12dNo ratings yet
- KET JessicaDocument44 pagesKET Jessicamember12dNo ratings yet
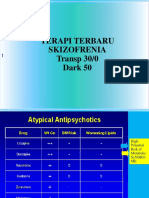
- Terapi Terbaru Skizofrenia Transp 30/0 Dark 50Document58 pagesTerapi Terbaru Skizofrenia Transp 30/0 Dark 50member12dNo ratings yet
- Bab 1 BPHDocument5 pagesBab 1 BPHmember12dNo ratings yet
- MercyDocument50 pagesMercyNdi Salem TNo ratings yet
- Laboratory Diagnosis of Parasitic DiseasesDocument37 pagesLaboratory Diagnosis of Parasitic Diseasespooja mahariyaNo ratings yet
- Super Parasitology TableDocument11 pagesSuper Parasitology Tablesleepyhead archerNo ratings yet
- Tet PGTRB Zoology Model Question Paper 2Document14 pagesTet PGTRB Zoology Model Question Paper 2Subbarayudu mamillaNo ratings yet
- Malariology: Plasmodium MalariaeDocument42 pagesMalariology: Plasmodium MalariaeFloey ZhaoNo ratings yet
- MalariaDocument17 pagesMalariaricardojosesotofontalvoNo ratings yet
- Monocystis AgilisDocument16 pagesMonocystis AgilisRavi JaiswalNo ratings yet
- Stool Microscopic ExaminationDocument5 pagesStool Microscopic Examinationsamantha_ong_22No ratings yet
- Coccidiosis in Large and Small RuminantsDocument8 pagesCoccidiosis in Large and Small RuminantsLorena PinedaNo ratings yet
- Unit 11. Blood and Tissue Coccidian (Apicomplexa)Document40 pagesUnit 11. Blood and Tissue Coccidian (Apicomplexa)Michael DawitNo ratings yet
- GR2 Plasmodium-Spp PDFDocument29 pagesGR2 Plasmodium-Spp PDFEran Mark RojasNo ratings yet
- PlasmodiumFalciparum New InformationDocument3 pagesPlasmodiumFalciparum New InformationJustin Jim SalazarNo ratings yet
- ParasitologyDocument27 pagesParasitologyDreyden HaloNo ratings yet
- Micro ParasitologyDocument5 pagesMicro ParasitologyPlzstudylav SyedNo ratings yet
- Clinical Parasitology TransesDocument73 pagesClinical Parasitology TransesNikoh Anthony EwayanNo ratings yet
- PlasmodiumDocument92 pagesPlasmodiumnitesh rawat100% (2)
- Eimeria 1 PDFDocument10 pagesEimeria 1 PDFalvian handiyantoNo ratings yet
- An Introduction of MalariaDocument19 pagesAn Introduction of MalariaSomesh GuptaNo ratings yet
- E. Histolytica Trophozoites Secrete Cysteine Proteases WhichDocument16 pagesE. Histolytica Trophozoites Secrete Cysteine Proteases WhichAherrera BanzuelaNo ratings yet
- Textbook Microbial Control of Vector Borne Diseases 1St Edition Brij Kishore Tyagi Ebook All Chapter PDFDocument53 pagesTextbook Microbial Control of Vector Borne Diseases 1St Edition Brij Kishore Tyagi Ebook All Chapter PDFjohn.saenz973100% (11)
- Lecture Notes in Medical Technology - Lecture # 16 - CLASS SPOROZOADocument23 pagesLecture Notes in Medical Technology - Lecture # 16 - CLASS SPOROZOAKat JornadalNo ratings yet
- ParasitesDocument56 pagesParasitesdenis marselaNo ratings yet
- Neet - Combined Test - 4 (P, C, B) - 23.07.2017Document21 pagesNeet - Combined Test - 4 (P, C, B) - 23.07.2017Sankar KumarasamyNo ratings yet
- Parasitic ProtozoaDocument254 pagesParasitic Protozoasivarocks100% (2)
- Care Study On MalariaDocument79 pagesCare Study On MalariaDan Agyemang NketiahNo ratings yet
- Study Guide of Medical Parasitology, Part 1. ProtozoologyDocument50 pagesStudy Guide of Medical Parasitology, Part 1. Protozoologymicrobehunter007No ratings yet
- Artículo 1 GiardiasisDocument11 pagesArtículo 1 GiardiasisJonathan Paul Ramirez RodríguezNo ratings yet
- Microbial MorphologyDocument41 pagesMicrobial MorphologyQuentin LopezNo ratings yet
- 9 Afi HDocument116 pages9 Afi HRuth DanielNo ratings yet