Download as pptx, pdf, or txt
You might also like
- Test Bank For Healthcare Human Resource Management 3rd EditionDocument37 pagesTest Bank For Healthcare Human Resource Management 3rd Editionsequelundam6h17s100% (17)
- Obstetrics MCQDocument8 pagesObstetrics MCQSandip Patil100% (6)
- Obstetrics and Gynecology NOTESDocument73 pagesObstetrics and Gynecology NOTESAwais Awais100% (6)
- RCOG Green Top Notes 1Document48 pagesRCOG Green Top Notes 1Anonymous LnLvsb100% (1)
- Ovarian Cysts: Presented by Neha Barari Assistant Professor SNSRDocument52 pagesOvarian Cysts: Presented by Neha Barari Assistant Professor SNSRBhawna JoshiNo ratings yet
- Benign Diseases of Cervix, Uterus & OvaryDocument58 pagesBenign Diseases of Cervix, Uterus & OvaryFaheem HassanNo ratings yet
- High Risk PregnancyDocument108 pagesHigh Risk PregnancyVincent Maralit MaterialNo ratings yet
- Fibroid Uterus 2019Document60 pagesFibroid Uterus 2019Mahmoud Abu Al AmrainNo ratings yet
- 1 MiscarriageDocument34 pages1 Miscarriagezxcvbzaki123No ratings yet
- REPRODUCTIONNDocument25 pagesREPRODUCTIONNSaqib ButtNo ratings yet
- Bleeding in Early PregnancyDocument40 pagesBleeding in Early PregnancyOmar mohamedNo ratings yet
- Breast DisordersDocument50 pagesBreast DisordersIsraa AlaaNo ratings yet
- Abortion: Mohamed Sinan Govt Medical College, CalicutDocument60 pagesAbortion: Mohamed Sinan Govt Medical College, CalicutMhr AliNo ratings yet
- Ovarian CystDocument19 pagesOvarian CystMuhammad AbeeshNo ratings yet
- Abortion: Mohamed Sinan Govt Medical College, CalicutDocument60 pagesAbortion: Mohamed Sinan Govt Medical College, CalicutYash SharmaNo ratings yet
- Benignlesionshanisah 161129150208Document71 pagesBenignlesionshanisah 161129150208Mohammad Saadullah Khan KakarNo ratings yet
- PA Genitalia WanitaDocument100 pagesPA Genitalia WanitaBNo ratings yet
- Benign Breast DisordersDocument30 pagesBenign Breast DisordersShams Nadeem AlamNo ratings yet
- Endometriosis O&g PresentationDocument31 pagesEndometriosis O&g PresentationChauthiran Agamudaiyar100% (1)
- MK Disorders in Early Pregnancy (OBGY)Document26 pagesMK Disorders in Early Pregnancy (OBGY)Moses Jr KazevuNo ratings yet
- Ectopic Pregancy: Chena B. CurigDocument35 pagesEctopic Pregancy: Chena B. CurigJaicca Faith Tandih AllasNo ratings yet
- Nursing Care of Mothers With Gestational Conditions:: 1. Abortion 2. Ectopic PregnancyDocument59 pagesNursing Care of Mothers With Gestational Conditions:: 1. Abortion 2. Ectopic PregnancyGwyneth FisherNo ratings yet
- Path Pathology of The Uterus Part 1 2020-2021Document7 pagesPath Pathology of The Uterus Part 1 2020-2021JohnNo ratings yet
- Abortion Sept2021Document51 pagesAbortion Sept2021vrunda joshiNo ratings yet
- 12.4 Female Reproductive DiseasesDocument20 pages12.4 Female Reproductive Diseasessanat kr pratiharNo ratings yet
- Gestational and Placental Disorders: Obstetric PathologyDocument45 pagesGestational and Placental Disorders: Obstetric PathologyVanessa HermioneNo ratings yet
- Ectopic PregnancyDocument54 pagesEctopic Pregnancypecolaa3No ratings yet
- ENDOMETRIOSISDocument33 pagesENDOMETRIOSISpriyanka bhowmikNo ratings yet
- Ectopic Pregnancy: Mbiine Ronald Nakiyemba OliviaDocument30 pagesEctopic Pregnancy: Mbiine Ronald Nakiyemba OliviaDIANENo ratings yet
- MiscarriageDocument39 pagesMiscarriagehacker ammerNo ratings yet
- 3&4 MiscarraigeDocument90 pages3&4 MiscarraigeAbdullah GadNo ratings yet
- Final ReviewerDocument22 pagesFinal ReviewerAlyssa DeleonNo ratings yet
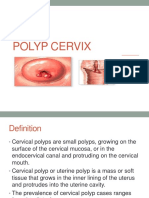
- Polyp CervixDocument14 pagesPolyp CervixT Horan100% (1)
- Female InfertilityDocument33 pagesFemale InfertilityKiprotich Titus NgetichNo ratings yet
- Benign Ovarian TumourDocument45 pagesBenign Ovarian Tumourahmed shorshNo ratings yet
- BENIGN OVARIAN DISEASES - Updated January 2018Document31 pagesBENIGN OVARIAN DISEASES - Updated January 2018daniel100% (1)
- 13 Gynaecological Conditions in General PracticeDocument64 pages13 Gynaecological Conditions in General Practices14214lscNo ratings yet
- Bleeding From The Genital Tract in Early Pregnancy (Before 28 Weeks)Document76 pagesBleeding From The Genital Tract in Early Pregnancy (Before 28 Weeks)Tiondi francisNo ratings yet
- Bleeding Early PreganacyDocument115 pagesBleeding Early PreganacyHaziq MarsNo ratings yet
- First Trimester BleedingDocument48 pagesFirst Trimester BleedingEliana ArshidNo ratings yet
- Ectopic PregnancyDocument3 pagesEctopic PregnancyMary Anne Yap100% (1)
- Bleeding in Early PregnancyDocument34 pagesBleeding in Early PregnancyAdenike OLAOGUNNo ratings yet
- Ectopic Pregnancy: Read MoreDocument15 pagesEctopic Pregnancy: Read MoreVanessa Santos100% (1)
- Benign ConditionsDocument40 pagesBenign ConditionsnoreenfatimamaanNo ratings yet
- Ectopic Pregnancy (Autosaved)Document56 pagesEctopic Pregnancy (Autosaved)susmita shresthaNo ratings yet
- AbortionDocument30 pagesAbortionKIYANo ratings yet
- 2 Pre Gestation and Gestational ConditionsDocument88 pages2 Pre Gestation and Gestational Conditionslermacornel61No ratings yet
- Management of Bleeding in Early PregnancyDocument44 pagesManagement of Bleeding in Early PregnancyOyedele OluwaseunNo ratings yet
- Presentation 1Document31 pagesPresentation 1SaadNo ratings yet
- Diseases MaleDocument45 pagesDiseases MaleFarhan DogarNo ratings yet
- Seminar G2 (Early Trimester Pregnancy Vaginal Bleeding)Document47 pagesSeminar G2 (Early Trimester Pregnancy Vaginal Bleeding)Chalie MequanentNo ratings yet
- CRT Breast (Complete)Document70 pagesCRT Breast (Complete)NATTAPAT SANGKAKULNo ratings yet
- Cervical Cancer: Santos, Maxime Ella L. Gecera, Alondra KateDocument22 pagesCervical Cancer: Santos, Maxime Ella L. Gecera, Alondra KateLyssaMarieKathryneEgeNo ratings yet
- Dysfunctional Uterine Bleeding Lecture DR Gem AshbyDocument45 pagesDysfunctional Uterine Bleeding Lecture DR Gem AshbyPandawa ObgynNo ratings yet
- Liomyoma (Fibroid) : DR Henan DH Skheel 2016 5 Year Directed LectureDocument11 pagesLiomyoma (Fibroid) : DR Henan DH Skheel 2016 5 Year Directed LectureAnonymous UHnQSkxLBDNo ratings yet
- Endometriosis Team 3 DidacticsDocument80 pagesEndometriosis Team 3 DidacticsAbegail IbañezNo ratings yet
- 64 GTD LectureDocument53 pages64 GTD Lecturecollinsmag0% (1)
- HemorrhagesDocument3 pagesHemorrhagesARAugustoNo ratings yet
- Multiple PregnancyDocument55 pagesMultiple PregnancyNathaniel YeriNo ratings yet
- Molar PregnancyDocument13 pagesMolar PregnancyShalynurNo ratings yet
- Abnormal Uterine Bleeding: 5 Year Medical Student Obstetrics & GynecologyDocument42 pagesAbnormal Uterine Bleeding: 5 Year Medical Student Obstetrics & Gynecologynoor hyNo ratings yet
- Theory of Myoma Uteri: Gede Nanda Surya WijayaDocument32 pagesTheory of Myoma Uteri: Gede Nanda Surya WijayaNandaSuryaWijayaNo ratings yet
- Female Infertility: DR Jaqueline Sudiman, PHDDocument21 pagesFemale Infertility: DR Jaqueline Sudiman, PHDJuli FionaNo ratings yet
- Ovarian Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOvarian Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 3 out of 5 stars3/5 (2)
- For A Complete List of Sponsors, Refer To The North Carolina General Assembly Web SiteDocument3 pagesFor A Complete List of Sponsors, Refer To The North Carolina General Assembly Web SiteUSA TODAY NetworkNo ratings yet
- 2 DOD POEP10 PerinatalLossDocument8 pages2 DOD POEP10 PerinatalLossLinda SzaboNo ratings yet
- StillbirthDocument27 pagesStillbirthJoseph Nawen SindiongNo ratings yet
- Full Download Introduction To Operations and Supply Chain Management 3rd Edition Bozarth Test BankDocument36 pagesFull Download Introduction To Operations and Supply Chain Management 3rd Edition Bozarth Test Bankcoraleementgen1858100% (49)
- Laporan Bulanan Lb1: 0-7 HR Baru LDocument20 pagesLaporan Bulanan Lb1: 0-7 HR Baru LOla SarlinaNo ratings yet
- Currens Math For Meds Dosages and Solutions 11th Edition Curren Test BankDocument36 pagesCurrens Math For Meds Dosages and Solutions 11th Edition Curren Test Banksynechia.goblinqrs4v100% (35)
- Lesson 11 - Appled Ethics and Reproductive IssuesDocument8 pagesLesson 11 - Appled Ethics and Reproductive IssuesTheodosia KNo ratings yet
- TorchDocument10 pagesTorchAyen Fajardo-HernalNo ratings yet
- Management of Miscarriage 2016 PDFDocument16 pagesManagement of Miscarriage 2016 PDFJLan JoNo ratings yet
- Embarazo Ectopico Tubarico ACOG 2018Document13 pagesEmbarazo Ectopico Tubarico ACOG 2018Jesus SuarezNo ratings yet
- ICICI Prudential Life Insurance Co LTD - Attachment - 6Document2 pagesICICI Prudential Life Insurance Co LTD - Attachment - 6vermalabNo ratings yet
- Maternity PolicyDocument4 pagesMaternity PolicyAshwini DasguptaNo ratings yet
- Malformasi KongenitalDocument6 pagesMalformasi KongenitalIntan PermataNo ratings yet
- Fertility AssessmentDocument38 pagesFertility AssessmentSkmc InfertilityNo ratings yet
- Obstetrics and Gynecology NotesDocument73 pagesObstetrics and Gynecology NotesHaspreet GillNo ratings yet
- Grief Unseen Healing Pregnancy Loss Through The ArtsDocument193 pagesGrief Unseen Healing Pregnancy Loss Through The Artselizondoag100% (1)
- Pathophysiology-Threatened MiscarriageDocument1 pagePathophysiology-Threatened MiscarriageMoses Gabriel ValledorNo ratings yet
- APPSC Departmental Tests Nov 2020 Session 11th Aug 2021 S2Document22 pagesAPPSC Departmental Tests Nov 2020 Session 11th Aug 2021 S2surya sunNo ratings yet
- Metroharrgia and Exopthalmus & ProptosisDocument12 pagesMetroharrgia and Exopthalmus & Proptosisfarah fadzilNo ratings yet
- Teen Birth StudyDocument26 pagesTeen Birth StudyWBURNo ratings yet
- Maternal and Child Health Practice TestDocument25 pagesMaternal and Child Health Practice TestANONYMOUSNo ratings yet
- Government College of Nursing Jodhpur (Raj.)Document5 pagesGovernment College of Nursing Jodhpur (Raj.)priyankaNo ratings yet
- Clinical Practice Guidelines On Miscarriage ManagementDocument44 pagesClinical Practice Guidelines On Miscarriage ManagementEvelyn LimNo ratings yet
- Bleeding During PregnancyDocument69 pagesBleeding During PregnancyMohnnad Hmood AlgaraybhNo ratings yet
- Piette YBEOG 2020 The Pharmacodynamics and Safety of ProgesteroneDocument17 pagesPiette YBEOG 2020 The Pharmacodynamics and Safety of ProgesteronePaul PIETTENo ratings yet
- Practical Research 2Document18 pagesPractical Research 2Maryrose TrajeBarroNo ratings yet