Download as pptx, pdf, or txt
You might also like
- AHA ACLS Megacode ScenariosDocument6 pagesAHA ACLS Megacode ScenariosChad Sanford78% (18)
- 2020 AHA Guidelines For CPR & ECCDocument42 pages2020 AHA Guidelines For CPR & ECCArun100% (1)
- First Aid HAndbookDocument54 pagesFirst Aid HAndbookGrethe JeneiNo ratings yet
- Student Assessment Booklet2: Hltaid003 PDocument36 pagesStudent Assessment Booklet2: Hltaid003 PPriyanka SinglaNo ratings yet
- Contraception: Kelompok 2 Farras Ajeng 16310105 Melisa Andesti 16310173 Shelfi Aprilia N 16310278Document10 pagesContraception: Kelompok 2 Farras Ajeng 16310105 Melisa Andesti 16310173 Shelfi Aprilia N 16310278sulesa askawiNo ratings yet
- Real Life 3.0 Scenario As Substitute For Bedside Clinical Practice Medical Surgical: GI BleedDocument7 pagesReal Life 3.0 Scenario As Substitute For Bedside Clinical Practice Medical Surgical: GI Bleedlmstar98No ratings yet
- Professional DevelopmentDocument11 pagesProfessional Developmentapi-340409341No ratings yet
- Existence of God & God The FatherDocument13 pagesExistence of God & God The Fatherfatherkline100% (1)
- A B C D e AssessmentDocument6 pagesA B C D e AssessmentANGELICA JANE FLORENDONo ratings yet
- Patient Centerd CareDocument42 pagesPatient Centerd Care21910589No ratings yet
- Person Centred 2Document13 pagesPerson Centred 2SARAHNo ratings yet
- Finals P PTTDocument114 pagesFinals P PTTIelle FranciscoNo ratings yet
- Telephone Delivery Conversation Worksheet RedDocument2 pagesTelephone Delivery Conversation Worksheet RedMaryNo ratings yet
- Concept of NursingDocument18 pagesConcept of Nursingنور حفيظه سلوانيNo ratings yet
- Name: Mojica, Noah Kent Date: September 19, 2020Document6 pagesName: Mojica, Noah Kent Date: September 19, 2020Noah Kent MojicaNo ratings yet
- 40 Brilliant Powerful Short Three Word QuotesDocument7 pages40 Brilliant Powerful Short Three Word QuotesShaira Mae CulladoNo ratings yet
- Jean WatsonDocument35 pagesJean WatsonSonia khanNo ratings yet
- Nurse Nurse Nurse:: Dialogue Between A Patient and Nurse Either With A Partner or SilentlyDocument3 pagesNurse Nurse Nurse:: Dialogue Between A Patient and Nurse Either With A Partner or SilentlySajib RezaNo ratings yet
- VasectomyDocument60 pagesVasectomyVlad ValentinNo ratings yet
- HRM 16 OBE-syllabusDocument12 pagesHRM 16 OBE-syllabusMark LennonNo ratings yet
- Bleeding in Early Late PregnancyDocument46 pagesBleeding in Early Late PregnancyAndrada Catrinoiu100% (2)
- Session 4-Elasticity of DemandDocument46 pagesSession 4-Elasticity of DemandDeep kardaniNo ratings yet
- L2 God As FatherDocument11 pagesL2 God As Fatherjonathan toffoloNo ratings yet
- PredictorDocument15 pagesPredictorfairwoods0% (1)
- NURS 321/527 Unit 4 Review Digestion: GERD, Malabsorption, Pancreatitis, HepatitisDocument19 pagesNURS 321/527 Unit 4 Review Digestion: GERD, Malabsorption, Pancreatitis, HepatitisSamip PatelNo ratings yet
- BFHI Case Studies FINAL PDFDocument61 pagesBFHI Case Studies FINAL PDFYhana Fheb Nabus BayacsanNo ratings yet
- 12 Trends and Issues in NursingDocument5 pages12 Trends and Issues in NursingPrincePunnoose0% (1)
- Intravenous TherapyDocument51 pagesIntravenous TherapySally GatbuntonNo ratings yet
- Nur460 - PGC Refelction PaperDocument13 pagesNur460 - PGC Refelction Paperapi-559074394No ratings yet
- Answers Accuplacer Esl Reading Skills Sample QuestionsDocument8 pagesAnswers Accuplacer Esl Reading Skills Sample QuestionsLavanya VanuNo ratings yet
- Pneumonia EvaluationDocument3 pagesPneumonia Evaluatione-MedTools50% (2)
- Adult Nursing Personal StatementDocument1 pageAdult Nursing Personal StatementlenaNo ratings yet
- Nursing ProcessDocument62 pagesNursing ProcessplethoraldorkNo ratings yet
- Principles of Biomedical EthicsDocument23 pagesPrinciples of Biomedical EthicskatyNo ratings yet
- Urinary EliminationDocument50 pagesUrinary EliminationAime MvuyekureNo ratings yet
- AdhdDocument20 pagesAdhdapi-548854218No ratings yet
- Safe and Effective Care EnvironmentDocument8 pagesSafe and Effective Care Environmentgretch_carreonNo ratings yet
- Syllabus Clinical Pathophysiology and Diagnostic Studies 2018Document8 pagesSyllabus Clinical Pathophysiology and Diagnostic Studies 2018d-fbuser-55269881No ratings yet
- Ha - Nursing ProcessDocument81 pagesHa - Nursing ProcessPam LalaNo ratings yet
- RN Job Description PDFDocument1 pageRN Job Description PDFvhon100% (1)
- Nurse Staffing Audit BookletDocument9 pagesNurse Staffing Audit BookletMaria Francesca MapaNo ratings yet
- Imaging For Urethral CalculusDocument19 pagesImaging For Urethral Calculuschimbimb100% (1)
- Chapter 18. A Safe Diagnostic StrategyDocument16 pagesChapter 18. A Safe Diagnostic StrategyMar HesNo ratings yet
- LIPPNCOTT Vital Signs Height Weight Chapter 016Document72 pagesLIPPNCOTT Vital Signs Height Weight Chapter 016Sara SabraNo ratings yet
- Oxygen Administration: Rachel Joy R. Rosale, RN, RM, MANDocument12 pagesOxygen Administration: Rachel Joy R. Rosale, RN, RM, MANChengRosaleNo ratings yet
- Patient NursingDocument7 pagesPatient Nursingsahilchaudhary7No ratings yet
- Assessment Planning and Implementation Evaluation: Subjective Data: STG: STGDocument3 pagesAssessment Planning and Implementation Evaluation: Subjective Data: STG: STGJoel Nick Molano100% (1)
- Triangle of Care Intro PDFDocument40 pagesTriangle of Care Intro PDFLaura AndreiNo ratings yet
- CH 73Document18 pagesCH 73JE Yufra100% (1)
- Why Patients Do Not Adhere To Medical Advice.: Health PsychologyDocument109 pagesWhy Patients Do Not Adhere To Medical Advice.: Health PsychologyNie' MK100% (1)
- Nurse Job Interview Questions About Rude DoctorsDocument1 pageNurse Job Interview Questions About Rude DoctorsDnr PhsNo ratings yet
- Constipation: Stools ExplainedDocument4 pagesConstipation: Stools ExplainedArun MuralidharanNo ratings yet
- Nurses Therapeutic CommunicationDocument11 pagesNurses Therapeutic Communicationsabu0099No ratings yet
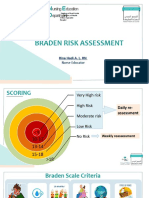
- Braden Risk AssessmentDocument19 pagesBraden Risk AssessmentRina LestariNo ratings yet
- Healthcare Provider CAB of CPR Helpful HintsDocument2 pagesHealthcare Provider CAB of CPR Helpful HintsDarrell BrightNo ratings yet
- Nursing-Unit-Conversion Leeds University PDFDocument10 pagesNursing-Unit-Conversion Leeds University PDFlucia100% (1)
- Clinical Nursing JudgementDocument6 pagesClinical Nursing Judgementapi-508132058No ratings yet
- Lassa Fever PaperDocument18 pagesLassa Fever PaperCherica OnateNo ratings yet
- ANS RPN Integrated Post Test I A PDFDocument25 pagesANS RPN Integrated Post Test I A PDFdaljit chahalNo ratings yet
- BDocument118 pagesBbeautifulme031690No ratings yet
- Implementing Personal Health Budgets: NHS Southern Derbyshire Clinical Commissioning GroupDocument23 pagesImplementing Personal Health Budgets: NHS Southern Derbyshire Clinical Commissioning Groupskw timur0% (1)
- ShockDocument22 pagesShockDiana RamberNo ratings yet
- Psych Test 1Document7 pagesPsych Test 1エルミタ ジョイ ファティマNo ratings yet
- Hiragana Katakana Chart: The Left Part Is Hiragana and The Right Part Is KatakanaDocument1 pageHiragana Katakana Chart: The Left Part Is Hiragana and The Right Part Is Katakanaエルミタ ジョイ ファティマNo ratings yet
- SDO Palawan Installs 196 RBI Sets As Part of Teachers On Air InitiativeDocument10 pagesSDO Palawan Installs 196 RBI Sets As Part of Teachers On Air Initiativeエルミタ ジョイ ファティマNo ratings yet
- CHED: 73 Schools Now Allowed To Hold Limited Face-To-Face ClassesDocument9 pagesCHED: 73 Schools Now Allowed To Hold Limited Face-To-Face Classesエルミタ ジョイ ファティマNo ratings yet
- I Love You With The Love of The Lord Icanseeinyouthe Glory of My King and I Love You With The Love of The LordDocument1 pageI Love You With The Love of The Lord Icanseeinyouthe Glory of My King and I Love You With The Love of The Lordエルミタ ジョイ ファティマNo ratings yet
- The Learners Demonstrate Understanding ofDocument15 pagesThe Learners Demonstrate Understanding ofエルミタ ジョイ ファティマNo ratings yet
- (W.a.t.c.h.) - SLM - Mathematics-3 - Ermita, Joy Fatima C.Document9 pages(W.a.t.c.h.) - SLM - Mathematics-3 - Ermita, Joy Fatima C.エルミタ ジョイ ファティマNo ratings yet
- Self - Learning - Module (Theories of Evolution) - ERMITA, JOY FATIMA C.Document12 pagesSelf - Learning - Module (Theories of Evolution) - ERMITA, JOY FATIMA C.エルミタ ジョイ ファティマNo ratings yet
- MOT-Child and Development BrochureDocument5 pagesMOT-Child and Development Brochureエルミタ ジョイ ファティマNo ratings yet
- Insight (Ermita, Joy Fatima C.)Document2 pagesInsight (Ermita, Joy Fatima C.)エルミタ ジョイ ファティマNo ratings yet
- Philippines: Crisis in Education?: Athira Nortajuddin 17 March 2021Document15 pagesPhilippines: Crisis in Education?: Athira Nortajuddin 17 March 2021エルミタ ジョイ ファティマNo ratings yet
- Developmental Theories Reflection #1: Freud'S Psychoanalytic TheoryDocument13 pagesDevelopmental Theories Reflection #1: Freud'S Psychoanalytic Theoryエルミタ ジョイ ファティマ100% (1)
- Table Runner: Prepared byDocument5 pagesTable Runner: Prepared byエルミタ ジョイ ファティマNo ratings yet
- He Said, Fear Not My Child ForDocument3 pagesHe Said, Fear Not My Child Forエルミタ ジョイ ファティマNo ratings yet
- The Placing of A SonDocument24 pagesThe Placing of A Sonエルミタ ジョイ ファティマ100% (1)
- Republic of The Philippines Camarines Sur Polytechnic CollegesDocument5 pagesRepublic of The Philippines Camarines Sur Polytechnic Collegesエルミタ ジョイ ファティマNo ratings yet
- What A Mighty GodDocument20 pagesWhat A Mighty Godエルミタ ジョイ ファティマNo ratings yet
- Deeper, DeeperDocument38 pagesDeeper, Deeperエルミタ ジョイ ファティマNo ratings yet
- When The Redeemed Are Gathering inDocument44 pagesWhen The Redeemed Are Gathering inエルミタ ジョイ ファティマNo ratings yet
- Glory To His NameDocument24 pagesGlory To His Nameエルミタ ジョイ ファティマNo ratings yet
- The Handsomest Drowned Man in The WorldDocument1 pageThe Handsomest Drowned Man in The Worldエルミタ ジョイ ファティマNo ratings yet
- Digital Technology in The Midst of Covid-19 Crisis in Educational System at LPNHSDocument3 pagesDigital Technology in The Midst of Covid-19 Crisis in Educational System at LPNHSエルミタ ジョイ ファティマNo ratings yet
- Learning Content: Writing The Reaction Paper Learning Title: Essay and Reaction Paper, Critique and Review Formal Theme Entry No. 1: Reaction PaperDocument21 pagesLearning Content: Writing The Reaction Paper Learning Title: Essay and Reaction Paper, Critique and Review Formal Theme Entry No. 1: Reaction Paperエルミタ ジョイ ファティマ100% (1)
- Come and DineDocument37 pagesCome and Dineエルミタ ジョイ ファティマNo ratings yet
- EAPP Q1M3 Tehnques in Smmrizng Diff Acad Texts R5Document24 pagesEAPP Q1M3 Tehnques in Smmrizng Diff Acad Texts R5エルミタ ジョイ ファティマ92% (13)
- Remote Health Atlas Resuscitation Trolley: 1. General InformationDocument3 pagesRemote Health Atlas Resuscitation Trolley: 1. General InformationSusanti ShantyNo ratings yet
- Pals Life SaverDocument13 pagesPals Life SaverStephany ZamorasNo ratings yet
- Emergency Prompt Cards 2021Document75 pagesEmergency Prompt Cards 2021bana.mbaroudiNo ratings yet
- A Lecture Versus Video Presentation On Knowledge and Skills of First Aid of Barangay Officials and Members of Bag-Ong Dalalguete Mahayag, Zamboanga Del SurDocument14 pagesA Lecture Versus Video Presentation On Knowledge and Skills of First Aid of Barangay Officials and Members of Bag-Ong Dalalguete Mahayag, Zamboanga Del SurJon Alvin M. Selisana0% (1)
- Basic Life Support and Advanced Cardiovascular Life SupportDocument90 pagesBasic Life Support and Advanced Cardiovascular Life SupportRakhshanda khan100% (1)
- BLS & AclsDocument112 pagesBLS & AclsPriya SharmaNo ratings yet
- Cardiopulmonary Resuscitation (CPR) : First AidDocument5 pagesCardiopulmonary Resuscitation (CPR) : First AidJules RyanNo ratings yet
- BLS Study Guide and PretestDocument47 pagesBLS Study Guide and PretestRicha AbcedeNo ratings yet
- Paramedic Refresher Download 2010Document111 pagesParamedic Refresher Download 2010Nitehawkix999100% (3)
- Clinical Audit On Code BlueDocument7 pagesClinical Audit On Code BlueSunny AnthonyNo ratings yet
- ATLSDocument18 pagesATLSإكرام النايبNo ratings yet
- Carefusion ResuscitationDocument8 pagesCarefusion Resuscitationrubenr25No ratings yet
- High Quality CPR, DR Ali Haedar PDFDocument45 pagesHigh Quality CPR, DR Ali Haedar PDFTaufik SuhendarNo ratings yet
- CPR and First AidsDocument2 pagesCPR and First AidsBruno Andre Garcia VegaNo ratings yet
- 5 Tips For CPR Training Success - Your Guide To Saving Lives - 7.4.24Document3 pages5 Tips For CPR Training Success - Your Guide To Saving Lives - 7.4.24amitvNo ratings yet
- Cardiac Arrest Upon Induction of General AnesthesiaDocument7 pagesCardiac Arrest Upon Induction of General AnesthesiaIlona HiariejNo ratings yet
- Chapter 4 Safety Practices in Outdoor RecreationDocument5 pagesChapter 4 Safety Practices in Outdoor RecreationJham LayoutsNo ratings yet
- Cvad and Code BlueDocument4 pagesCvad and Code BlueMarcus, RNNo ratings yet
- BCLS&ACLS ZJDocument26 pagesBCLS&ACLS ZJZoe Jeanne GarcianoNo ratings yet
- Enterprise 5000X (E5X) : Instructions For UseDocument60 pagesEnterprise 5000X (E5X) : Instructions For UseJiThiN vPNo ratings yet
- 76 Calling-911 ESL LIBRARY ANSWERKEYDocument7 pages76 Calling-911 ESL LIBRARY ANSWERKEYCamilo Mejía100% (2)
- T-90 Single Temp Installation ManualDocument56 pagesT-90 Single Temp Installation ManualHeriberto Felix PereiraNo ratings yet
- Prof Badge Syllabus2020 EDITED 28122021Document103 pagesProf Badge Syllabus2020 EDITED 28122021piranap piranapNo ratings yet
- Presentation For Saksham Training - Basic Life SupportDocument51 pagesPresentation For Saksham Training - Basic Life SupportPotluri SunilNo ratings yet
- Atlas NeonatologyDocument395 pagesAtlas NeonatologyNguyễn Trung83% (6)
- 2020 SPA Pediatric Perioperative Critical Events ChecklistsDocument30 pages2020 SPA Pediatric Perioperative Critical Events ChecklistsKukuh PrasetyoNo ratings yet