Download as pptx, pdf, or txt
You might also like
- St. Augustine Choir Booklet-1Document255 pagesSt. Augustine Choir Booklet-1Henry Kaweesa97% (58)
- Primarchs DatasheetsDocument24 pagesPrimarchs DatasheetsJosiah Young1100% (5)
- Hematology & UrinalysisDocument77 pagesHematology & UrinalysismekuriawNo ratings yet
- Complete Blood Count: at A GlanceDocument6 pagesComplete Blood Count: at A Glancecsy123No ratings yet
- UntitledDocument112 pagesUntitledMerriyet MbNo ratings yet
- Blood Cell CountDocument27 pagesBlood Cell CountDiane-Richie PezLoNo ratings yet
- 1 Hematology TestDocument48 pages1 Hematology TestAhmed YassinNo ratings yet
- Anemia Clinical ConsiderationDocument39 pagesAnemia Clinical Considerationema dwi laksanaNo ratings yet
- The Complete Blood Count Is The Calculation of The Cellular (Formed Elements) of BloodDocument26 pagesThe Complete Blood Count Is The Calculation of The Cellular (Formed Elements) of BloodNabard MhammadNo ratings yet
- Hematology L5Document22 pagesHematology L5Haibat Sultan StationeryNo ratings yet
- Integrated Therapeutics Iii Credit 4Hrs/Week: Instructor: Tamrat Legesse (B.Pharm, MSC in Clinical Pharmacy)Document145 pagesIntegrated Therapeutics Iii Credit 4Hrs/Week: Instructor: Tamrat Legesse (B.Pharm, MSC in Clinical Pharmacy)dawitNo ratings yet
- Como Interpreto Un Hemograma en Adulto-Mayo-2005Document14 pagesComo Interpreto Un Hemograma en Adulto-Mayo-2005Gustavo VasquezNo ratings yet
- White Blood Cells Red Blood Cells Platelets: Complete Blood Count (CBC)Document11 pagesWhite Blood Cells Red Blood Cells Platelets: Complete Blood Count (CBC)bsonNo ratings yet
- Piis0025619611615681 PDFDocument14 pagesPiis0025619611615681 PDFMaryJoy Dela CruzNo ratings yet
- Laboratory Investigations in Oral and Maxillofacial SurgeryDocument187 pagesLaboratory Investigations in Oral and Maxillofacial SurgeryTarun KashyapNo ratings yet
- Complete Blood Count (CBC) Test: WBC DifferentialDocument4 pagesComplete Blood Count (CBC) Test: WBC Differentialchang02No ratings yet
- UPTODATE: Approach To The Adult With AnemiaDocument8 pagesUPTODATE: Approach To The Adult With AnemiakimberlynNo ratings yet
- 39notes Clinical PathologyDocument9 pages39notes Clinical PathologyaymenNo ratings yet
- Rodaks 6th Ed. Hema Lab Midterm ReviewerDocument30 pagesRodaks 6th Ed. Hema Lab Midterm ReviewerGerald SorianoNo ratings yet
- CBCDocument15 pagesCBCUlicer CruzNo ratings yet
- Handout Basic HematologyDocument188 pagesHandout Basic HematologymaikkadoriaNo ratings yet
- Anemia LectureDocument70 pagesAnemia LectureramwshNo ratings yet
- Complete Blood Count: Performed To Provide An Overview of A Patient's General Health StatusDocument4 pagesComplete Blood Count: Performed To Provide An Overview of A Patient's General Health StatusRaprnaNo ratings yet
- Cardio Skills LabDocument4 pagesCardio Skills LabShine KhayNo ratings yet
- List Blood Tests Performed As Part of A CBCDocument9 pagesList Blood Tests Performed As Part of A CBCamiosaNo ratings yet
- Hematology Interest Group CNL Myeloproliferative NeoplasmDocument10 pagesHematology Interest Group CNL Myeloproliferative Neoplasmapi-384537137No ratings yet
- CP RBC DisorderDocument15 pagesCP RBC DisorderDETECTIVE CONANNo ratings yet
- Anemia, Tic, DLC MbbsDocument50 pagesAnemia, Tic, DLC Mbbssharads221004No ratings yet
- Case 1: 25 Yr Old Patient With History of FatigueDocument79 pagesCase 1: 25 Yr Old Patient With History of FatigueMira Wrycza100% (1)
- Haematology 2 ManualDocument26 pagesHaematology 2 Manualhayamitib11No ratings yet
- Red CellDocument4 pagesRed CellUmer naeemNo ratings yet
- (PATHO) LEC 013 RBC-and-Bleeding-DisordersDocument20 pages(PATHO) LEC 013 RBC-and-Bleeding-DisordersEzhilNo ratings yet
- Hematological Investigation or Quantitative Evaluation of The Hematopoietic SystemDocument21 pagesHematological Investigation or Quantitative Evaluation of The Hematopoietic SystemMAMA LALANo ratings yet
- Haematological Tests: Jhanvi Ka Patel Rool No. 09Document21 pagesHaematological Tests: Jhanvi Ka Patel Rool No. 09Aditya PatelNo ratings yet
- ABC of CBC: RDW-all That One Should Know & Apply in Clinical Practice: Dr. Sudhir MehtaDocument21 pagesABC of CBC: RDW-all That One Should Know & Apply in Clinical Practice: Dr. Sudhir Mehtaamba100% (1)
- (S.C. Rastogi) Essentials of Animal Physiology, 4t (BookSee - Org) 247Document1 page(S.C. Rastogi) Essentials of Animal Physiology, 4t (BookSee - Org) 247Indah Rizka AprilianiNo ratings yet
- Classification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Document78 pagesClassification of Anemias: What Is Anemia, How Do You Diagnose Anemia, and How Are The Different Anemias Classified?Kaushik BhuvaNo ratings yet
- CBC InterpretationDocument6 pagesCBC InterpretationKate Basa100% (2)
- Nucleated Rbcs-Significance in The Peripheral Blood Film: H He em Ma at To Ol Lo Og Gy YDocument7 pagesNucleated Rbcs-Significance in The Peripheral Blood Film: H He em Ma at To Ol Lo Og Gy YFede0No ratings yet
- 2nd Sem - Hema1 - An Overview of Clinical Laboratory HematologyDocument3 pages2nd Sem - Hema1 - An Overview of Clinical Laboratory HematologyAisle Malibiran PalerNo ratings yet
- CBC StudyDocument3 pagesCBC Studyremjith rajendranNo ratings yet
- The An Them We Have The Second One That Is The: Causes of AnemiaDocument6 pagesThe An Them We Have The Second One That Is The: Causes of AnemiakimberlynNo ratings yet
- 21-22 - Laboratory Examination and Work-Up For Hematologic Disorders - DR - Ariful HayatDocument111 pages21-22 - Laboratory Examination and Work-Up For Hematologic Disorders - DR - Ariful HayatGiselleNo ratings yet
- Blood IndicesDocument4 pagesBlood IndicesCharmaine RosalesNo ratings yet
- What Is The Complete Blood Count Test (CBC) ?: White Blood Cells Red Blood Cells PlateletsDocument4 pagesWhat Is The Complete Blood Count Test (CBC) ?: White Blood Cells Red Blood Cells PlateletsSheryl Ann Celis BacaniNo ratings yet
- Interpretation of CBC: Dr. N. BajajDocument56 pagesInterpretation of CBC: Dr. N. BajajHaSan Z. MustafaNo ratings yet
- Hematology: Complete Blood Count and Differential CountDocument12 pagesHematology: Complete Blood Count and Differential CountimperiouxxNo ratings yet
- S0850alug 1670953860959-SEU HDocument56 pagesS0850alug 1670953860959-SEU HAziz KhwajaNo ratings yet
- Hematology Tests - G I SVDocument49 pagesHematology Tests - G I SVSV. Trần Hữu ThắngNo ratings yet
- Chapter 18 Anemia HematologyDocument30 pagesChapter 18 Anemia HematologyYelnats DatsimaNo ratings yet
- Lab Investigations of AnemiaDocument109 pagesLab Investigations of AnemiaMadhura ShekatkarNo ratings yet
- 1 Introduction To AnemiaDocument60 pages1 Introduction To AnemiaKhisha RangasNo ratings yet
- Red and White Blood Cell DisordersDocument11 pagesRed and White Blood Cell DisordersVittorio Di PaoloNo ratings yet
- Anemia Determining The CauseDocument13 pagesAnemia Determining The CauseMarisol AsakuraNo ratings yet
- 17 AnemiaDocument46 pages17 AnemiaMeraol HusseinNo ratings yet
- Hematopathology All LecturesDocument226 pagesHematopathology All LecturesYousif AlaaNo ratings yet
- N 5315 Advaned Pathophysiology Anemia TranscriptDocument9 pagesN 5315 Advaned Pathophysiology Anemia TranscriptllukelawrenceNo ratings yet
- 1st Lect in Hem-2021-Dr - HazimDocument5 pages1st Lect in Hem-2021-Dr - HazimAnmarNo ratings yet
- CLS Unit 2 NotesDocument8 pagesCLS Unit 2 NotesBailey EdwinsonNo ratings yet
- BloodDocument6 pagesBloodMatthew Zane BroderickNo ratings yet
- 5db83ef1f71e482 PDFDocument192 pages5db83ef1f71e482 PDFRajesh RoyNo ratings yet
- Fizika RadiologijaDocument9 pagesFizika RadiologijaBorislav TapavičkiNo ratings yet
- Atlas Engineering Bar Handbook Rev Jan 2005-Oct 2011Document136 pagesAtlas Engineering Bar Handbook Rev Jan 2005-Oct 2011carlosc19715043No ratings yet
- Notes On Jean Piaget DeweyDocument2 pagesNotes On Jean Piaget DeweyfadzillahNo ratings yet
- Swathi Final Project AnilDocument100 pagesSwathi Final Project AnilHussainNo ratings yet
- Distribution Channel of AMULDocument13 pagesDistribution Channel of AMULMeet JivaniNo ratings yet
- IVRA07 1656 01 English ManualDocument2 pagesIVRA07 1656 01 English ManualDejan MilosavljevicNo ratings yet
- Chapter 11 Icse Midpoint TheoremDocument10 pagesChapter 11 Icse Midpoint TheoremDeepika MohanbabuNo ratings yet
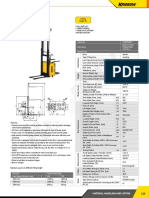
- Electric Stacker: Article No. KW0500894 Description Electric Stacker (Triplex Mast) 1.5T x3 M SpecificationDocument1 pageElectric Stacker: Article No. KW0500894 Description Electric Stacker (Triplex Mast) 1.5T x3 M SpecificationAsty RikyNo ratings yet
- 3 PBDocument11 pages3 PBSuci DwiNo ratings yet
- CBC TMDocument108 pagesCBC TMChryz SantosNo ratings yet
- Pipe Pressure Drope ASEREHDocument3 pagesPipe Pressure Drope ASEREHSenghou MeasNo ratings yet
- ITSM Gap Analysis TemplateDocument57 pagesITSM Gap Analysis TemplateSuresh RajamaniNo ratings yet
- 3.3 PfmeaDocument5 pages3.3 PfmeaEaswaranNo ratings yet
- Siemens 3VT MCCBDocument39 pagesSiemens 3VT MCCBerkamlakar2234No ratings yet
- Scala AccesoriesDocument27 pagesScala AccesoriesZiggy BussyNo ratings yet
- Supra AccessoryDocument7 pagesSupra AccessoryaeroglideNo ratings yet
- Skills Test Unit 1 BDocument5 pagesSkills Test Unit 1 BOsama CanaanNo ratings yet
- Acm 4 - B4-A1Document4 pagesAcm 4 - B4-A1Heru HaryantoNo ratings yet
- HBR Catalogue Eng KKPCDocument2 pagesHBR Catalogue Eng KKPCIulian Victor MafteiNo ratings yet
- KaizenDocument8 pagesKaizenGigih SetijawanNo ratings yet
- The Challenges of TodayDocument5 pagesThe Challenges of TodayqamaradeelNo ratings yet
- Lesson 11 Creating A Positive School CultureDocument4 pagesLesson 11 Creating A Positive School CultureLIM CHUNG SZE KPM-GuruNo ratings yet
- Progress in The Development of A Reynolds-Stress Turbulence ClosureDocument30 pagesProgress in The Development of A Reynolds-Stress Turbulence ClosureMutiaRezaNo ratings yet
- GlobalCOD Method 2000 2015Document85 pagesGlobalCOD Method 2000 2015suma riadiNo ratings yet
- Module 6 - Sequential Circuits, Excitation Function, State Table, State DiagramDocument21 pagesModule 6 - Sequential Circuits, Excitation Function, State Table, State DiagramYvanne Esquia CuregNo ratings yet
- Bahir Dar University College of Medicine and Health SciencesDocument21 pagesBahir Dar University College of Medicine and Health SciencesMegbaruNo ratings yet
- Final DKSSKDocument79 pagesFinal DKSSKSarita Latthe100% (2)