Download as pptx, pdf, or txt
You might also like
- My Little Island 2 TBDocument268 pagesMy Little Island 2 TBNguyenHang100% (4)
- Health Teaching Plan (Breastfeeding)Document5 pagesHealth Teaching Plan (Breastfeeding)Zam Pamate100% (7)
- Health Teaching For Pregnant - Written ReportDocument7 pagesHealth Teaching For Pregnant - Written ReportczhuenaNo ratings yet
- PostpartumDocument7 pagesPostpartummaryNo ratings yet
- Post Natal BookletDocument16 pagesPost Natal BookletSravan GanjiNo ratings yet
- Postpartum Discharge InstructionsDocument7 pagesPostpartum Discharge InstructionsGilianne JimeneaNo ratings yet
- Birthing Positions - Health Teaching Plan - GERALIDocument7 pagesBirthing Positions - Health Teaching Plan - GERALIMikaela Gabrielle GERALINo ratings yet
- Birthing Positions - Health Teaching PlanDocument7 pagesBirthing Positions - Health Teaching PlanMikaela Gabrielle GERALINo ratings yet
- Level 2 Skills Lab PresentationDocument24 pagesLevel 2 Skills Lab PresentationJamie HaravataNo ratings yet
- For Resting:: Side-Lying. Try Placing Semi-Sitting, in Bed, On A Sitting With One Foot UpDocument5 pagesFor Resting:: Side-Lying. Try Placing Semi-Sitting, in Bed, On A Sitting With One Foot UpZhandy ZanduetaNo ratings yet
- POGP FFBirthDocument12 pagesPOGP FFBirth4pq8zgt2bqNo ratings yet
- Breastfeeding FinalDocument25 pagesBreastfeeding FinalWengel RedkissNo ratings yet
- The Birth: For Healthcare Professionals To Give To ParentsDocument8 pagesThe Birth: For Healthcare Professionals To Give To Parentsmeenurawat21No ratings yet
- No 2Document8 pagesNo 2Mifta AliNo ratings yet
- ManueversDocument97 pagesManueverscataleya mesaNo ratings yet
- Breast Feeding TechniquesDocument15 pagesBreast Feeding TechniquesIsmael NdayisangaNo ratings yet
- Anatomy and Physiology of NSDDocument4 pagesAnatomy and Physiology of NSDkyle otedaNo ratings yet
- Topic # 1 Leopold's ManueverDocument39 pagesTopic # 1 Leopold's ManueverJayrelle D. SafranNo ratings yet
- Lactaction AssignmentDocument4 pagesLactaction AssignmentShizkiNo ratings yet
- Breastfeeding SeminarDocument37 pagesBreastfeeding SeminarAlfreda MeggyNo ratings yet
- Cereneal CareDocument4 pagesCereneal CareWadhha AlsenaidiNo ratings yet
- Technique of BreastfeedingDocument8 pagesTechnique of BreastfeedingSubhranil MaityNo ratings yet
- Advice and Exercise After ChildbirthDocument24 pagesAdvice and Exercise After ChildbirthAmani TrangNo ratings yet
- Lecture Leopolds-ManeuverDocument32 pagesLecture Leopolds-ManeuverkrischaniNo ratings yet
- Module 7 ASSISTED DELIVERYDocument18 pagesModule 7 ASSISTED DELIVERYSPE CommitteeNo ratings yet
- OB Stages of Labor and Care in The Stages of Labor With VideoDocument45 pagesOB Stages of Labor and Care in The Stages of Labor With VideodsmagallanesNo ratings yet
- Stages of Labor & Delivery and Danger Signs of Labor: Week 11 ReportersDocument30 pagesStages of Labor & Delivery and Danger Signs of Labor: Week 11 ReportersMushy_ayaNo ratings yet
- Posterior Babies PDFDocument3 pagesPosterior Babies PDFMar FarréNo ratings yet
- Position During LaborDocument13 pagesPosition During LaborEvaNatashaNo ratings yet
- Pelvic Girdle Pain LeafletDocument5 pagesPelvic Girdle Pain LeafletagniosaiNo ratings yet
- Module 10 COMMON OBSTETRIC EMERGENCIESDocument53 pagesModule 10 COMMON OBSTETRIC EMERGENCIESSPE CommitteeNo ratings yet
- Rota2 Leopolds Maneuver & FHTDocument37 pagesRota2 Leopolds Maneuver & FHTSandara Delas PenasNo ratings yet
- MCN Lab - M7 - INTRAPARTUM CARE 2020-2021Document28 pagesMCN Lab - M7 - INTRAPARTUM CARE 2020-2021Kristine Kim100% (1)
- Birth Is Not An IllnessDocument13 pagesBirth Is Not An IllnessacebanditsNo ratings yet
- Nursing Management Offirst Second Stage of LaborDocument10 pagesNursing Management Offirst Second Stage of LaborSana RazaNo ratings yet
- Crisanto Cajang Mariecor Enriquez Kathleen Jayne Ramos Kathleen Kayla Baguioen Rosemarie Joy JucutanDocument58 pagesCrisanto Cajang Mariecor Enriquez Kathleen Jayne Ramos Kathleen Kayla Baguioen Rosemarie Joy JucutanGary PicarNo ratings yet
- Postnatal Exercises: Caring For Your BodyDocument16 pagesPostnatal Exercises: Caring For Your BodyLga PrakashNo ratings yet
- Normal Labor: Kevin Marcial I. Aralar, MD 1 Year ResidentDocument46 pagesNormal Labor: Kevin Marcial I. Aralar, MD 1 Year ResidentKevin AralarNo ratings yet
- SPBRDocument44 pagesSPBRNoemi CristescuNo ratings yet
- Health Education: (Intra and Post-Partum Clients)Document12 pagesHealth Education: (Intra and Post-Partum Clients)Alleja Rose M. LAGUNANo ratings yet
- Breastfeeding: PurposesDocument6 pagesBreastfeeding: PurposesAlex BasadaNo ratings yet
- Emergency ChildbirthDocument29 pagesEmergency ChildbirthFernandoMatosNo ratings yet
- The First Stage of LaborDocument5 pagesThe First Stage of LaborReyna Mee AhiyasNo ratings yet
- Group II Makati Medical Center m8 1Document107 pagesGroup II Makati Medical Center m8 1CASSANDRAJUL VARINNo ratings yet
- Technique of Breast Feeding (Position of Breast Feeding)Document17 pagesTechnique of Breast Feeding (Position of Breast Feeding)Rajeev NepalNo ratings yet
- Importance of BreastfeedingDocument6 pagesImportance of BreastfeedingJade HemmingsNo ratings yet
- MCHNDocument3 pagesMCHNBenjamin Hofschneider EspinosaNo ratings yet
- Course Task 3Document3 pagesCourse Task 3ALYSSA SAM MASANGCAYNo ratings yet
- Advice and Exercise After Childbirth V2Document22 pagesAdvice and Exercise After Childbirth V2Phạm Thị ThuậnNo ratings yet
- Different Breastfeeding Positions: Cradle HoldDocument4 pagesDifferent Breastfeeding Positions: Cradle HoldMaria Angela VirayNo ratings yet
- Labor and Birth HandoutDocument9 pagesLabor and Birth Handoutapi-240665032No ratings yet
- AB Manifesto 2Document6 pagesAB Manifesto 2yayusuk desamtaNo ratings yet
- Minor Discomfort in PuerperiumDocument39 pagesMinor Discomfort in PuerperiumVarna Mohan100% (1)
- EpisiotomyDocument7 pagesEpisiotomyJalajarani Aridass100% (1)
- Seminar On Various Child Birth Practice, PositionDocument26 pagesSeminar On Various Child Birth Practice, PositionPiyush Dutta100% (1)
- Physio Coccyx Pain During Pregnancy - Dec22Document6 pagesPhysio Coccyx Pain During Pregnancy - Dec22sophia.sadiq555No ratings yet
- Newborn Agger Docu.Document12 pagesNewborn Agger Docu.Krizamay Ongat AggerNo ratings yet
- MaternalDocument6 pagesMaternalNorbelisa Tabo-ac CadungganNo ratings yet
- Various Childbirth PracticesDocument11 pagesVarious Childbirth PracticesFarheen khan100% (1)
- Emergency Childbirth A Reference Guide for Students of the Medical Self-help Training Course, Lesson No. 11From EverandEmergency Childbirth A Reference Guide for Students of the Medical Self-help Training Course, Lesson No. 11No ratings yet
- "Physiological Monitoring and Device Interface": Report by Jawia Mustapha BSN2-ADocument21 pages"Physiological Monitoring and Device Interface": Report by Jawia Mustapha BSN2-ADimple AnticamaraNo ratings yet
- The Woman With Unique Concerns in LaborDocument10 pagesThe Woman With Unique Concerns in LaborDimple Anticamara0% (1)
- The Care of Woman During The First Stage of LaborDocument8 pagesThe Care of Woman During The First Stage of LaborDimple AnticamaraNo ratings yet
- The Care of A Woman During The Third and Fourth Stages of LaborDocument16 pagesThe Care of A Woman During The Third and Fourth Stages of LaborDimple AnticamaraNo ratings yet
- Planning, Design, and Implementation of Information Technology in Complex Healthcare SystemsDocument11 pagesPlanning, Design, and Implementation of Information Technology in Complex Healthcare SystemsDimple AnticamaraNo ratings yet
- The Woman With Unique Concerns in Labor: VACALARES - VALENZUELA - TomambilingDocument10 pagesThe Woman With Unique Concerns in Labor: VACALARES - VALENZUELA - TomambilingDimple AnticamaraNo ratings yet
- Computerized Provider Order Entry: - ObjectivesDocument7 pagesComputerized Provider Order Entry: - ObjectivesDimple AnticamaraNo ratings yet
- Nursing Informatics Chapter 47Document20 pagesNursing Informatics Chapter 47Dimple AnticamaraNo ratings yet
- Crowley - The Crisis in FreemasonryDocument18 pagesCrowley - The Crisis in FreemasonryCelephaïs Press / Unspeakable Press (Leng)100% (4)
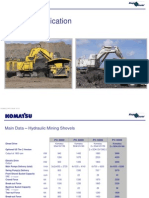
- 11 - PC8000 - 6 ApplDocument37 pages11 - PC8000 - 6 Appljhon jairo trujillo100% (1)
- BOQDocument4 pagesBOQMehmood SaleemNo ratings yet
- Answers To Questions: MishkinDocument8 pagesAnswers To Questions: Mishkin?ᄋᄉᄋNo ratings yet
- RealVNC Enterprise Edition 4Document2 pagesRealVNC Enterprise Edition 4fannybrawijayaNo ratings yet
- ADF Health Manual Vol 20, Part8, Chp2Document18 pagesADF Health Manual Vol 20, Part8, Chp2Ahmad Usman Tahir100% (2)
- Parents ConsentDocument2 pagesParents ConsentkarlylNo ratings yet
- Zhao - An Intertextual Approach To Translation at The Macro-LevelDocument9 pagesZhao - An Intertextual Approach To Translation at The Macro-LevelangielskiajNo ratings yet
- MetalurgiaDocument5 pagesMetalurgiaAndjelkaStankovicNo ratings yet
- 101-0020 USB-RS485 Converter Manual R2Document8 pages101-0020 USB-RS485 Converter Manual R2Juan Pablo Villazon RichterNo ratings yet
- Basics and Applications of Induction FurnacesDocument54 pagesBasics and Applications of Induction Furnacespioneerinvincible100% (4)
- Translating Algebraic ExpressionsDocument2 pagesTranslating Algebraic ExpressionsSiti Inayya SavalianiNo ratings yet
- C 20 Aeronautical 1 2 SemDocument161 pagesC 20 Aeronautical 1 2 Semyamuna A0% (1)
- Speakout DVD Extra Intermediate Unit 10 PDFDocument1 pageSpeakout DVD Extra Intermediate Unit 10 PDFОксана МальцеваNo ratings yet
- 04 Measuring Sustainability and Sustainable LivelihoodsDocument27 pages04 Measuring Sustainability and Sustainable Livelihoodsahmed_1uk100% (1)
- Battery MSDSDocument3 pagesBattery MSDSAnkitNo ratings yet
- Distance Learning Programme: Jee (Main) : Leader Test Series / Joint Package CourseDocument32 pagesDistance Learning Programme: Jee (Main) : Leader Test Series / Joint Package Coursekraken monsterNo ratings yet
- Deepfake Is The Future of Content Creation'Document9 pagesDeepfake Is The Future of Content Creation'I IvaNo ratings yet
- Site Analysis Report - Mr. Reimond SilvestreDocument13 pagesSite Analysis Report - Mr. Reimond Silvestrechristian reyesNo ratings yet
- A Beginners Guide On How Paper Tubes Cores Are ManufacturedDocument7 pagesA Beginners Guide On How Paper Tubes Cores Are ManufacturedAjaysinh JadejaNo ratings yet
- Jurnal Fusi ProtoplasmaDocument10 pagesJurnal Fusi ProtoplasmaN. Beauregard이진기No ratings yet
- 1 - CV Bery Rizky GintingDocument3 pages1 - CV Bery Rizky GintingGerry SampetodingNo ratings yet
- G10-Science QTR 1Document5 pagesG10-Science QTR 1Leah Ampis Orcullo100% (1)
- NCERT Solutions For Class 3 Maths Chapter 12Document16 pagesNCERT Solutions For Class 3 Maths Chapter 12Prashant GuptaNo ratings yet
- Letter of Reference Angela Mathew 1Document3 pagesLetter of Reference Angela Mathew 1api-490106269No ratings yet
- Murat by Alexandre DumasDocument48 pagesMurat by Alexandre DumasEdina OrbánNo ratings yet
- MWT - Product Intro - Artsen Plus - ENDocument13 pagesMWT - Product Intro - Artsen Plus - ENBhumikaNo ratings yet
- Coolnomixac 1Document2 pagesCoolnomixac 1Eko AdiNo ratings yet
- Prevention of Sexual Harassment at WorkplaceDocument62 pagesPrevention of Sexual Harassment at WorkplaceNitesh kumar singhNo ratings yet