Download as ppt, pdf, or txt
You might also like
- SAFE-T Protocoal With Columbia Suicide Severity Rating ScaleDocument3 pagesSAFE-T Protocoal With Columbia Suicide Severity Rating ScaleMuniandy Ramachandran100% (1)
- Nursing OB Exam Q & ADocument173 pagesNursing OB Exam Q & Ajoerobinson8889323100% (8)
- Delivery Room Write UpDocument15 pagesDelivery Room Write UpDavid Calalo0% (1)
- Ass Ectopic PregnancyDocument10 pagesAss Ectopic PregnancyPriyaNo ratings yet
- NSVD Case StudyDocument11 pagesNSVD Case StudyMichael UrrutiaNo ratings yet
- Case Study - Ectopic PregnancyDocument10 pagesCase Study - Ectopic Pregnancykristine keen buanNo ratings yet
- Ectopic PregnancyDocument26 pagesEctopic PregnancyCHryz TinNo ratings yet
- Nstemi PathoDocument2 pagesNstemi PathoSheana TmplNo ratings yet
- Gynaecology TextbookDocument35 pagesGynaecology Textbooktkimbini95No ratings yet
- Case Study - CS With BTLDocument16 pagesCase Study - CS With BTLAJ Roze Holmes100% (2)
- Case Study of Cesarean SectionDocument9 pagesCase Study of Cesarean SectionErika Joy Imperio0% (1)
- PATHOPHYSIOLOGY ECTOPIC PREGNANCY SoftDocument11 pagesPATHOPHYSIOLOGY ECTOPIC PREGNANCY SoftJann ericka JaoNo ratings yet
- Involution of The UterusDocument13 pagesInvolution of The Uteruslandegre KNo ratings yet
- Lague - Case Analysis ReportDocument43 pagesLague - Case Analysis Reportinah krizia lagueNo ratings yet
- Mechanism of LabourDocument10 pagesMechanism of LabourMithlesh Dewangan100% (4)
- Ectopic PregnancyDocument18 pagesEctopic PregnancyMc_Lopez_1761No ratings yet
- Iko 2 VbacDocument7 pagesIko 2 VbacHusen AliNo ratings yet
- Maternal and Child Health IDocument772 pagesMaternal and Child Health Ikarendelarosa06100% (6)
- Displacement of The UterusDocument32 pagesDisplacement of The UterusRaja100% (1)
- SEMINAR ON Antepartum HaemorrageDocument18 pagesSEMINAR ON Antepartum Haemorragekathyayani arraNo ratings yet
- Unit 2Document73 pagesUnit 2Bharat ThapaNo ratings yet
- Presentasi Blok 2.3 Modul 3Document34 pagesPresentasi Blok 2.3 Modul 3Andrew StewartNo ratings yet
- Congenital Abnormalities of The UterusDocument7 pagesCongenital Abnormalities of The Uterusمحمود الموسويNo ratings yet
- Obgyn SL4Document31 pagesObgyn SL4mustafe omarNo ratings yet
- UntitledDocument43 pagesUntitledDakshayini MbNo ratings yet
- Those Related To The Pregnant State: AbortionDocument43 pagesThose Related To The Pregnant State: AbortionJohannah DaroNo ratings yet
- A 3.1 Sudden Pregnancy Complications PDFDocument47 pagesA 3.1 Sudden Pregnancy Complications PDFCamille Joy BaliliNo ratings yet
- Rle FinalsDocument31 pagesRle FinalsMae Arra Lecobu-anNo ratings yet
- OR Write-Up CSDocument13 pagesOR Write-Up CSalex_tan1981No ratings yet
- Sites of An Ectopic Pregnancy AreDocument11 pagesSites of An Ectopic Pregnancy AreLouie Kem Anthony BabaranNo ratings yet
- RACE Annotated ObsDocument35 pagesRACE Annotated ObsIsmath JahangirNo ratings yet
- Bleeding in Early PregnancyDocument20 pagesBleeding in Early Pregnancynanapet80No ratings yet
- 2 Physiology of LaborDocument56 pages2 Physiology of LaborkajramirezcaNo ratings yet
- Postpartum Complications: Ahmed AliDocument36 pagesPostpartum Complications: Ahmed AliPeter Osundwa KitekiNo ratings yet
- Anatomical and Physiological Changes During PregnancyDocument25 pagesAnatomical and Physiological Changes During Pregnancyqaleeq100% (1)
- Pregnancy 1Document70 pagesPregnancy 1Annapurna DangetiNo ratings yet
- Case Study of Abruptio PlacentaDocument14 pagesCase Study of Abruptio PlacentaLexy Milante80% (10)
- 178 Anatomy Reproductive SystemDocument25 pages178 Anatomy Reproductive SystemJUVY ANN PATOSANo ratings yet
- Obstetrics V10 Common Obstetric Conditions Chapter Pathology of The Placenta 1663285373Document11 pagesObstetrics V10 Common Obstetric Conditions Chapter Pathology of The Placenta 1663285373Nurliana NingsihNo ratings yet
- Institute of Nursing Intrapartum Care Handouts: Labor and Delivery Theories of Labor OnsetDocument7 pagesInstitute of Nursing Intrapartum Care Handouts: Labor and Delivery Theories of Labor OnsetTimi BCNo ratings yet
- Reporductive SystemDocument31 pagesReporductive SystemEmma Joel OtaiNo ratings yet
- Ectopic Ana PhysioDocument5 pagesEctopic Ana PhysioblubrinNo ratings yet
- 5 - Abortion or MiscarriageDocument43 pages5 - Abortion or Miscarriageasifdawar2011No ratings yet
- PregnancyDocument34 pagesPregnancyNamrata patelNo ratings yet
- Ectopic Pregnancy ImportantDocument42 pagesEctopic Pregnancy Importantﻣﻠﻚ عيسىNo ratings yet
- Case 5Document18 pagesCase 5Brian Arthur LeysonNo ratings yet
- Family Case Study 1Document12 pagesFamily Case Study 1Mark Anthony Torcino AbianNo ratings yet
- Abortion and Ectopic PregnancyDocument3 pagesAbortion and Ectopic PregnancyJefelson Eu Palaña NahidNo ratings yet
- Laporan Pendahuluan Asuhan Keperawatan Persalinan NormalDocument25 pagesLaporan Pendahuluan Asuhan Keperawatan Persalinan NormalBernadine AveliaNo ratings yet
- Anatomical and Physiological ChangesDocument25 pagesAnatomical and Physiological ChangespoojasolNo ratings yet
- Unit 4 Obg SubmissionDocument35 pagesUnit 4 Obg SubmissionSavita HanamsagarNo ratings yet
- Chapter 9: Nursing Care During Normal Pregnancy and Care of The Developing FetusDocument8 pagesChapter 9: Nursing Care During Normal Pregnancy and Care of The Developing FetusAlyssaGrandeMontimor100% (1)
- Labor DystociaDocument100 pagesLabor DystociaAnonymous kChMIy7tXNo ratings yet
- Feb 19. CA 2 - 1681737641118Document9 pagesFeb 19. CA 2 - 1681737641118HANNAH BANGKILINGNo ratings yet
- Anatomy and Physiology-Case 5Document5 pagesAnatomy and Physiology-Case 5JasminKate SutacioNo ratings yet
- Powerpoint Case Study of MiscarriageDocument25 pagesPowerpoint Case Study of MiscarriageAngel CauilanNo ratings yet
- Physiologic Changes of Pregnancy (Normal) : Local (I.e., Confined To The Systemic (I.e., Affecting TheDocument9 pagesPhysiologic Changes of Pregnancy (Normal) : Local (I.e., Confined To The Systemic (I.e., Affecting TheAli Longasa CortezNo ratings yet
- MCN Nursing 1Document107 pagesMCN Nursing 1Fau Fau DheoboNo ratings yet
- Vaginal Bleeding in Early PregnancyDocument8 pagesVaginal Bleeding in Early PregnancyBal Ri Mekoleu100% (1)
- Displacement of The Uterus: DR Sahar Anwar RizkDocument32 pagesDisplacement of The Uterus: DR Sahar Anwar RizkWida Ratna SariNo ratings yet
- Early Pregnancy Complications: by Harvir Singh Supervised by DR Ranjit and DR SyafiqahDocument33 pagesEarly Pregnancy Complications: by Harvir Singh Supervised by DR Ranjit and DR SyafiqahShre RanjithamNo ratings yet
- Last Minute Embryology: Human embryology made easy and digestible for medical and nursing studentsFrom EverandLast Minute Embryology: Human embryology made easy and digestible for medical and nursing studentsNo ratings yet
- Ex, 2a, B, C, 3, 4a, B, Pages 50-51 (SB) 2a.: 1. Most Advertising in Ancient Times Was Word-Of-Mouth, That Is, PeopleDocument4 pagesEx, 2a, B, C, 3, 4a, B, Pages 50-51 (SB) 2a.: 1. Most Advertising in Ancient Times Was Word-Of-Mouth, That Is, PeopleRodriguez Vivanco Kevin DanielNo ratings yet
- Disappearing LanguagesDocument4 pagesDisappearing LanguagesRodriguez Vivanco Kevin DanielNo ratings yet
- Pathphys ModuleDocument102 pagesPathphys ModuleRodriguez Vivanco Kevin DanielNo ratings yet
- 14-GIT and LiverDocument36 pages14-GIT and LiverRodriguez Vivanco Kevin DanielNo ratings yet
- 6 Krok GitDocument14 pages6 Krok GitRodriguez Vivanco Kevin DanielNo ratings yet
- Англ тести фармDocument138 pagesАнгл тести фармRodriguez Vivanco Kevin DanielNo ratings yet
- Red Blood Cells PathologyDocument47 pagesRed Blood Cells PathologyRodriguez Vivanco Kevin DanielNo ratings yet
- Pathophysiology of Endocrine SystemDocument37 pagesPathophysiology of Endocrine SystemRodriguez Vivanco Kevin DanielNo ratings yet
- 12-Blood Vessels PathologyDocument37 pages12-Blood Vessels PathologyRodriguez Vivanco Kevin DanielNo ratings yet
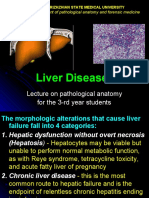
- Liver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsDocument27 pagesLiver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
- Endocrine Pathology: Lecture On Pathomorphology For 3-rd Year StudentsDocument44 pagesEndocrine Pathology: Lecture On Pathomorphology For 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
- 13 - Lung PathologyDocument38 pages13 - Lung PathologyRodriguez Vivanco Kevin DanielNo ratings yet
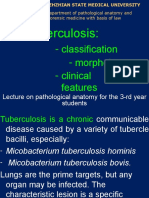
- Tuberculosis:: - Classification - Morphology - Clinical FeaturesDocument28 pagesTuberculosis:: - Classification - Morphology - Clinical FeaturesRodriguez Vivanco Kevin DanielNo ratings yet
- Nursing Practice 2019Document87 pagesNursing Practice 2019Rodriguez Vivanco Kevin DanielNo ratings yet
- Topic - Operation, AnesthesiaDocument5 pagesTopic - Operation, AnesthesiaRodriguez Vivanco Kevin DanielNo ratings yet
- Example of Practical Work 3Document5 pagesExample of Practical Work 3Rodriguez Vivanco Kevin DanielNo ratings yet
- Age PeriodsDocument12 pagesAge PeriodsRodriguez Vivanco Kevin DanielNo ratings yet
- VP Sales Medical Devices in Nashville TN Resume David MartinezDocument2 pagesVP Sales Medical Devices in Nashville TN Resume David MartinezDavidMartinezNo ratings yet
- ELECTROLYTESDocument8 pagesELECTROLYTESvarshith gandlaNo ratings yet
- Fusidic Acid - Wikipedia, The Free EncyclopediaDocument6 pagesFusidic Acid - Wikipedia, The Free EncyclopediaAnkan PalNo ratings yet
- Bls Study GuideDocument2 pagesBls Study GuideJohnNo ratings yet
- Wound InfectionDocument2 pagesWound InfectionMary Anjeanette Ramos VardeleonNo ratings yet
- Blood Gases and Acid-Base BalanceDocument11 pagesBlood Gases and Acid-Base BalanceREMAN ALINGASANo ratings yet
- CardionotesDocument5 pagesCardionotesNichole Coletta100% (1)
- 4.radiolucent Inflammatory Jaw Lesions A TwentyyearDocument7 pages4.radiolucent Inflammatory Jaw Lesions A TwentyyearMihaela TuculinaNo ratings yet
- Hope 1Document3 pagesHope 1Hasmine Lara RiveroNo ratings yet
- Probiotics, Prebiotics and Synbiotics - A ReviewDocument12 pagesProbiotics, Prebiotics and Synbiotics - A ReviewluthfikhairulNo ratings yet
- Pyogenic Liver AbscessDocument10 pagesPyogenic Liver AbscessFergie Erazo BeltránNo ratings yet
- Hulda Clark - ZapperDocument113 pagesHulda Clark - ZapperCarlosNo ratings yet
- GoutDocument16 pagesGoutfzee13No ratings yet
- The Esc Textbook of Intensive and Acute Cardiovascular Care 3Rd Edition Marco Tubaro Editor Full Download ChapterDocument51 pagesThe Esc Textbook of Intensive and Acute Cardiovascular Care 3Rd Edition Marco Tubaro Editor Full Download Chaptergilbert.spinney923100% (7)
- Pneumonia PathophysiologyDocument1 pagePneumonia PathophysiologyDee Sarajan100% (3)
- dm2020 0123Document47 pagesdm2020 0123Franchise AlienNo ratings yet
- LEC#34 Anti Helimintic DrugsDocument17 pagesLEC#34 Anti Helimintic Drugsalihyderabro166No ratings yet
- International Journal of Surgery: Nikolaos S. Salemis, Stavros Gourgiotis, Georgios KaralisDocument4 pagesInternational Journal of Surgery: Nikolaos S. Salemis, Stavros Gourgiotis, Georgios KaralisKinandanaNo ratings yet
- Fistulectomy: - Prepared byDocument65 pagesFistulectomy: - Prepared byMonette Abalos MendovaNo ratings yet
- CLR 12021Document63 pagesCLR 12021Eliza DNNo ratings yet
- Health MateDocument3 pagesHealth MateAnisah AquilaNo ratings yet
- Handbook of OrthodonticsDocument1 pageHandbook of OrthodonticsCarlos Alberto CastañedaNo ratings yet
- Antimicrobial PANCE ReviewDocument40 pagesAntimicrobial PANCE ReviewFlora LawrenceNo ratings yet
- H N O S CH N: Indication DosageDocument2 pagesH N O S CH N: Indication DosagehelloaNo ratings yet
- Haemnatology and Blood BiochemnistryDocument11 pagesHaemnatology and Blood BiochemnistryValentina SuescunNo ratings yet
- An Update On The New Investigations in Our ClinicDocument17 pagesAn Update On The New Investigations in Our ClinickhanasifalamNo ratings yet
- Pemanfaatan Epas Pada LBPDocument134 pagesPemanfaatan Epas Pada LBPBesa Erlin PukaNo ratings yet
- Brain Tumors: Primary BTDocument5 pagesBrain Tumors: Primary BTMohamed Al-zichrawyNo ratings yet