Download as ppt, pdf, or txt
You might also like
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Genetic Materia Medica - Vol-1 - by Parful Vijayakar - Typed PDFDocument278 pagesGenetic Materia Medica - Vol-1 - by Parful Vijayakar - Typed PDFvirag.patil100% (4)
- Chapter 2 Dyspnea-Harrison SummaryDocument5 pagesChapter 2 Dyspnea-Harrison SummaryLeang KarichakNo ratings yet
- Care Plan 3Document3 pagesCare Plan 3nyctotem50% (2)
- Sample Emergency Room ReportsDocument2 pagesSample Emergency Room ReportsErika Lm0% (2)
- Gagal NapasDocument49 pagesGagal NapasimaderadityaNo ratings yet
- 15 - Respiratory FailureDocument33 pages15 - Respiratory FailureSelin SakarNo ratings yet
- Clinical Physiology of Respiration: Dr. M Qathar RF TDocument76 pagesClinical Physiology of Respiration: Dr. M Qathar RF TTiwi Lestari TiwiNo ratings yet
- Sesak Napas Arimbi (PBL)Document50 pagesSesak Napas Arimbi (PBL)Endik SiswantoNo ratings yet
- Resp 180214084710Document72 pagesResp 180214084710Karla Geraldine Carhuas VeliNo ratings yet
- Sindromatologi DyspneuDocument18 pagesSindromatologi DyspneuMeylan TaebenuNo ratings yet
- Acute & Chronic Bronchitis & COPDDocument49 pagesAcute & Chronic Bronchitis & COPDHendraDarmawanNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document32 pagesChronic Obstructive Pulmonary Disease (COPD)matrixtrinityNo ratings yet
- Acute Respiratory FailureDocument51 pagesAcute Respiratory Failureigorhorenko15No ratings yet
- LI 8 - Differential Diagnosis of Acute Heart FailureDocument11 pagesLI 8 - Differential Diagnosis of Acute Heart Failure19-034 Jefry Junaidi PurbaNo ratings yet
- Acute Respiratory FailureDocument77 pagesAcute Respiratory FailureDeepika LingamNo ratings yet
- Pulmonary FailureDocument29 pagesPulmonary FailureWengel RedkissNo ratings yet
- Pemicu 6 KGD AldiDocument134 pagesPemicu 6 KGD AldiFirdaus AldyNo ratings yet
- Dyspnea (Sesak Nafas) FixDocument35 pagesDyspnea (Sesak Nafas) Fixamrul aliNo ratings yet
- Pathophysiologyofrespiratoryfailurefinal 130628075619 Phpapp01Document50 pagesPathophysiologyofrespiratoryfailurefinal 130628075619 Phpapp01Eller Tacud CollantesNo ratings yet
- Respiratory FailureDocument39 pagesRespiratory FailureMuntasir BashirNo ratings yet
- Acute Respiratory Distress DoxxDocument4 pagesAcute Respiratory Distress DoxxGenelyn MarquezNo ratings yet
- History Taking 2. Physical Examination 3. Diagnostic TestsDocument33 pagesHistory Taking 2. Physical Examination 3. Diagnostic TestsAmalNo ratings yet
- An Approach To A Patient With BreathlessnessDocument35 pagesAn Approach To A Patient With Breathlessnessgl tousifNo ratings yet
- Diagnostic Evaluation of Dyspnea: Am Fam Physician. 1998 Feb 15 57 (4) :711-716Document10 pagesDiagnostic Evaluation of Dyspnea: Am Fam Physician. 1998 Feb 15 57 (4) :711-716bellinasarsaNo ratings yet
- Respiratory FailureDocument52 pagesRespiratory FailureMohammad_Islam87100% (8)
- Resp InsuffDocument30 pagesResp InsuffCLEMENTNo ratings yet
- Resp System. ExamDocument145 pagesResp System. ExamIrina CornilovNo ratings yet
- FON oxygenationPPTDocument58 pagesFON oxygenationPPTSaeed khanNo ratings yet
- Explain The Classification of The Respiratory Failure?Document3 pagesExplain The Classification of The Respiratory Failure?anthy putrisriyantiNo ratings yet
- Critical CareDocument44 pagesCritical Caremohamedsharkawwy82No ratings yet
- DyspnoeaDocument1 pageDyspnoeaShubham TarapureNo ratings yet
- Patho Respiratory - KatherineDocument9 pagesPatho Respiratory - KatherineKayla MayerNo ratings yet
- Acute Respiratory Failure 1Document7 pagesAcute Respiratory Failure 1Trish 0019No ratings yet
- Respiratory FailureDocument41 pagesRespiratory FailureM HNo ratings yet
- Copd Pulmonary Edema: DR Sunil Arora Professor Deptt of PathologyDocument52 pagesCopd Pulmonary Edema: DR Sunil Arora Professor Deptt of PathologyMunesh SherawatNo ratings yet
- Kebutuhan Dasar Manusia OksigenasiDocument117 pagesKebutuhan Dasar Manusia Oksigenasiintanputri ramadhaniNo ratings yet
- It 14 ArdsDocument58 pagesIt 14 ArdsMohamad Fiqih ArrachmanNo ratings yet
- Basic Human Needs Oxygenation Ventilation/PerfusionDocument122 pagesBasic Human Needs Oxygenation Ventilation/PerfusionMichael BonillaNo ratings yet
- Respiratory ArrestDocument2 pagesRespiratory ArrestJesse FlingNo ratings yet
- Chronic Obstructive Pulmonary Disease: Christine Loren T. Laya BSN 3-1Document41 pagesChronic Obstructive Pulmonary Disease: Christine Loren T. Laya BSN 3-1Kristine CastilloNo ratings yet
- Sherif EL Hawary, MD Professor of Internal Medicine Kasr AL AiniDocument35 pagesSherif EL Hawary, MD Professor of Internal Medicine Kasr AL Aini670411No ratings yet
- ARFDocument50 pagesARFAme MehadiNo ratings yet
- Respiratory Failure: Dr. Sat Sharma Univ of ManitobaDocument38 pagesRespiratory Failure: Dr. Sat Sharma Univ of ManitobaGonzalo Venegas RojasNo ratings yet
- Respiratory Failure: by Amera GumamaDocument26 pagesRespiratory Failure: by Amera GumamaGumama AmeiyrhaNo ratings yet
- Acute Pulmonary Edema: Purwoko Sugeng HDocument25 pagesAcute Pulmonary Edema: Purwoko Sugeng HBee DanielNo ratings yet
- 3 Dyspnea, Palpitation, CyanosisDocument62 pages3 Dyspnea, Palpitation, CyanosisJoseph De JoyaNo ratings yet
- ACUTE Respiratory Distress Syndrome (ARDS)Document16 pagesACUTE Respiratory Distress Syndrome (ARDS)prayitno mulyaniNo ratings yet
- Respiratory Failure: by ArDocument39 pagesRespiratory Failure: by ArAleksei RomahovNo ratings yet
- DyspneaDocument29 pagesDyspneaBeNz ZodiazepinNo ratings yet
- Symptoms and Signs of Pulmonary DiseasesDocument29 pagesSymptoms and Signs of Pulmonary DiseasesDiana_anca6No ratings yet
- Dyspnea PresentationDocument37 pagesDyspnea PresentationamgoperaNo ratings yet
- COPD Bat NoteDocument6 pagesCOPD Bat NoteLankeshwaraNo ratings yet
- M V ICU: Echanical Entilation INDocument82 pagesM V ICU: Echanical Entilation INabhilashreddy45No ratings yet
- Respiratory enDocument92 pagesRespiratory enmayankmaheshwari.kzNo ratings yet
- Patofisiologi BatukDocument53 pagesPatofisiologi BatukGd PadmawijayaNo ratings yet
- Acute Respiratory Distress SyndromeDocument18 pagesAcute Respiratory Distress SyndromeJerinNo ratings yet
- Kuliah Pakar 2 Dyspnea PBLDocument35 pagesKuliah Pakar 2 Dyspnea PBLTrisya AksaraNo ratings yet
- COPDs Asthma Emphys and Chronic Bronchitis2024Document30 pagesCOPDs Asthma Emphys and Chronic Bronchitis2024Frolian MichaelNo ratings yet
- COPD:RLDDocument11 pagesCOPD:RLDKhiara Yapha AlfarNo ratings yet
- Dyspnea PDFDocument49 pagesDyspnea PDFUy FunkNo ratings yet
- Ena Respiratory EmergenciesDocument30 pagesEna Respiratory Emergencieseng78ineNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Ex, 2a, B, C, 3, 4a, B, Pages 50-51 (SB) 2a.: 1. Most Advertising in Ancient Times Was Word-Of-Mouth, That Is, PeopleDocument4 pagesEx, 2a, B, C, 3, 4a, B, Pages 50-51 (SB) 2a.: 1. Most Advertising in Ancient Times Was Word-Of-Mouth, That Is, PeopleRodriguez Vivanco Kevin DanielNo ratings yet
- Disappearing LanguagesDocument4 pagesDisappearing LanguagesRodriguez Vivanco Kevin DanielNo ratings yet
- Англ тести фармDocument138 pagesАнгл тести фармRodriguez Vivanco Kevin DanielNo ratings yet
- Pathphys ModuleDocument102 pagesPathphys ModuleRodriguez Vivanco Kevin DanielNo ratings yet
- 6 Krok GitDocument14 pages6 Krok GitRodriguez Vivanco Kevin DanielNo ratings yet
- 12-Blood Vessels PathologyDocument37 pages12-Blood Vessels PathologyRodriguez Vivanco Kevin DanielNo ratings yet
- Pathophysiology of Endocrine SystemDocument37 pagesPathophysiology of Endocrine SystemRodriguez Vivanco Kevin DanielNo ratings yet
- Example of Practical Work 3Document5 pagesExample of Practical Work 3Rodriguez Vivanco Kevin DanielNo ratings yet
- Red Blood Cells PathologyDocument47 pagesRed Blood Cells PathologyRodriguez Vivanco Kevin DanielNo ratings yet
- Pathology of Pregnancy and Delivery: Lecture On Pathological Anatomy For The 3-rd Year StudentsDocument35 pagesPathology of Pregnancy and Delivery: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
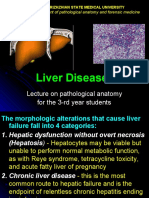
- Liver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsDocument27 pagesLiver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
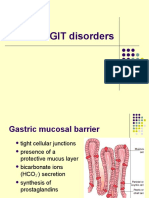
- 14-GIT and LiverDocument36 pages14-GIT and LiverRodriguez Vivanco Kevin DanielNo ratings yet
- Endocrine Pathology: Lecture On Pathomorphology For 3-rd Year StudentsDocument44 pagesEndocrine Pathology: Lecture On Pathomorphology For 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
- Topic - Operation, AnesthesiaDocument5 pagesTopic - Operation, AnesthesiaRodriguez Vivanco Kevin DanielNo ratings yet
- Tuberculosis:: - Classification - Morphology - Clinical FeaturesDocument28 pagesTuberculosis:: - Classification - Morphology - Clinical FeaturesRodriguez Vivanco Kevin DanielNo ratings yet
- Age PeriodsDocument12 pagesAge PeriodsRodriguez Vivanco Kevin DanielNo ratings yet
- Nursing Practice 2019Document87 pagesNursing Practice 2019Rodriguez Vivanco Kevin DanielNo ratings yet
- Edema Pathology by Asif AliDocument21 pagesEdema Pathology by Asif AliHassan AsifNo ratings yet
- AAFP and ISFM Guidelines For Diagnosing and Solving House-Soiling Behavior in CatsDocument20 pagesAAFP and ISFM Guidelines For Diagnosing and Solving House-Soiling Behavior in CatsElida LiraNo ratings yet
- HQ.89 - Exercise SheetDocument4 pagesHQ.89 - Exercise SheetsasaemNo ratings yet
- 5 Inglés BernardelliDocument1 page5 Inglés BernardellibenedettoNo ratings yet
- Carcinoma BreastDocument8 pagesCarcinoma BreastYeshvi s100% (1)
- Klebsiella Shigella Yersinia: Have Little Value in IDDocument6 pagesKlebsiella Shigella Yersinia: Have Little Value in IDKenneth Jake Batiduan100% (1)
- Curs Prim Ajutor 2023 - MG An V - Șocul Hemoragic - English-1Document18 pagesCurs Prim Ajutor 2023 - MG An V - Șocul Hemoragic - English-1hulia jokoNo ratings yet
- National Mastitis Council 2018Document137 pagesNational Mastitis Council 2018Lysett CoronaNo ratings yet
- MN580 Midterm Exam ReviewDocument17 pagesMN580 Midterm Exam ReviewAmanda CozzaNo ratings yet
- Diseases of Urinary System - Ayurveda ConceptsDocument48 pagesDiseases of Urinary System - Ayurveda ConceptskavindukarunarathnaNo ratings yet
- Bronchiolitis in Infants and Children - Clinical Features and Diagnosis - UpToDateDocument32 pagesBronchiolitis in Infants and Children - Clinical Features and Diagnosis - UpToDatedaniso12No ratings yet
- Linguistics and Literature Review (LLR) : Ambreen Shahriar Junaid G.MDocument11 pagesLinguistics and Literature Review (LLR) : Ambreen Shahriar Junaid G.MUMT JournalsNo ratings yet
- JUSTINE Medical-for-Athletes-2-1Document2 pagesJUSTINE Medical-for-Athletes-2-1joselito papa100% (1)
- SDHC San Diego Feasibility Report Final - 2017-01Document42 pagesSDHC San Diego Feasibility Report Final - 2017-01sawilson1No ratings yet
- Nursing Care Plan: Non-Pharmacological InterventionsDocument4 pagesNursing Care Plan: Non-Pharmacological InterventionsVivian PhamNo ratings yet
- English Quarter 3 - Week 3: Clarifying MeaningsDocument21 pagesEnglish Quarter 3 - Week 3: Clarifying MeaningsArianne TaylanNo ratings yet
- Yolk Gall EtcDocument5 pagesYolk Gall EtcNaveen BasudeNo ratings yet
- Panic Disorder & Somatoform DisorderDocument20 pagesPanic Disorder & Somatoform DisorderTHRESIAMA VINCE PNo ratings yet
- Filarial Worm: Richard David Silvestre, RMT, MSMT 9 C 0Document13 pagesFilarial Worm: Richard David Silvestre, RMT, MSMT 9 C 0Hearts heavy Moms spaghettiNo ratings yet
- Example Literature Review On Childhood ObesityDocument6 pagesExample Literature Review On Childhood Obesityc5praq5p100% (1)
- Predictive Value of National Early Warning Score 2 NEWS2 For Intensive Care Unit Admission in Patients With SARS CoV 2 InfectionDocument8 pagesPredictive Value of National Early Warning Score 2 NEWS2 For Intensive Care Unit Admission in Patients With SARS CoV 2 InfectionVictoria SalazarNo ratings yet
- Report On Drug AddictionDocument30 pagesReport On Drug AddictionChirag GoyalNo ratings yet
- NCP DiarrheaDocument2 pagesNCP DiarrheaElisha Faith Sevilla Espineli0% (1)
- Radiographic Positioning and Related Anatomy 8Th Edition Bontrager Test Bank Full Chapter PDFDocument35 pagesRadiographic Positioning and Related Anatomy 8Th Edition Bontrager Test Bank Full Chapter PDFdecagrambarrymfh100% (8)
- Journal Fajar Ahmad PrasetyaDocument22 pagesJournal Fajar Ahmad PrasetyaFajar Ahmad PrasetyaNo ratings yet
- IV InfiltrationDocument4 pagesIV InfiltrationMatthew Ryan100% (1)
- VIRAL Robin Cook ExcerptDocument18 pagesVIRAL Robin Cook ExcerptOtid DellmhalNo ratings yet