Download as ppt, pdf, or txt
You might also like
- General Biology 2 Quarter 4Document48 pagesGeneral Biology 2 Quarter 4Kishly Concepcion78% (9)
- Chapter 8: The Mammalian Transport System: SummaryDocument4 pagesChapter 8: The Mammalian Transport System: SummaryMerimaNo ratings yet
- Disorders of Blood Pressure Regulation - 10Document31 pagesDisorders of Blood Pressure Regulation - 10Cres Padua QuinzonNo ratings yet
- Secondary Hypertension: S Ystolic-Diastolic Arterial HypetrtensionDocument9 pagesSecondary Hypertension: S Ystolic-Diastolic Arterial HypetrtensionvifawuduNo ratings yet
- Hypertension: Margaret Xaira R. Mercado RNDocument36 pagesHypertension: Margaret Xaira R. Mercado RNMargaret Xaira Rubio MercadoNo ratings yet
- Integrated Therapeutics IiiDocument160 pagesIntegrated Therapeutics IiiSalahadinNo ratings yet
- HYPERTENSIONDocument10 pagesHYPERTENSIONChelsea Faith SarandiNo ratings yet
- 5.06 - HypertensionDocument3 pages5.06 - HypertensionJason JungNo ratings yet
- Hypertension: Hypertension Is One of The Most Common Worldwide Diseases Afflicting Humans. BecauseDocument8 pagesHypertension: Hypertension Is One of The Most Common Worldwide Diseases Afflicting Humans. BecauseKramojNo ratings yet
- Hypertension - CH 33 (Lewis)Document4 pagesHypertension - CH 33 (Lewis)Marisol AaronsNo ratings yet
- Kuliah Hipertensi KMB1 2018Document43 pagesKuliah Hipertensi KMB1 2018Ainu RamadhaniNo ratings yet
- HypertensionDocument12 pagesHypertensionDr. PARMINDER NAINNo ratings yet
- Scenario ThreeDocument25 pagesScenario Threeapi-3831474No ratings yet
- Chapter 31 HypertensionDocument3 pagesChapter 31 HypertensionVen SemillaNo ratings yet
- Hypertension and Antihypertensives (Iniaghe) Physiotherapy Students Oct 2021Document15 pagesHypertension and Antihypertensives (Iniaghe) Physiotherapy Students Oct 2021s9hdy4gsqrNo ratings yet
- Hypertension OutlineDocument14 pagesHypertension OutlineMaria CayacoNo ratings yet
- HypertensionDocument55 pagesHypertensionSr.Jyothy SABSNo ratings yet
- Antihypertensive Drugs Lecture-1Document94 pagesAntihypertensive Drugs Lecture-1onyeukwudaniel12No ratings yet
- 1 - HypertensionDocument35 pages1 - HypertensionLobna ElkilanyNo ratings yet
- HypertensionDocument11 pagesHypertensionJyoti singhNo ratings yet
- Hypertension FinalDocument64 pagesHypertension FinalrameshbmcNo ratings yet
- Cardiac Failure: Definition: Compensatory Changes in Heart FailureDocument5 pagesCardiac Failure: Definition: Compensatory Changes in Heart FailureMatyie SmkasNo ratings yet
- Elevated Arterial Pressure Is Called HypertensionDocument27 pagesElevated Arterial Pressure Is Called Hypertensionsaurabhv89No ratings yet
- HypertensionDocument10 pagesHypertensionRima HannaniNo ratings yet
- Hypertension: Prepared By: Eden Marie D. Francisco Lorraine Nicolne B. CortejoDocument27 pagesHypertension: Prepared By: Eden Marie D. Francisco Lorraine Nicolne B. CortejoAlecNo ratings yet
- Blood Pressure: Dr. Dev K Shah Assistant Professor Dept of PhysiologyDocument23 pagesBlood Pressure: Dr. Dev K Shah Assistant Professor Dept of Physiologysapana shresthaNo ratings yet
- Hypertension Definition:: Nitric OxideDocument5 pagesHypertension Definition:: Nitric OxideAnonymous bbeAZHxZNo ratings yet
- Hypertensive Crisis: Megat Mohd Azman Bin AdzmiDocument34 pagesHypertensive Crisis: Megat Mohd Azman Bin AdzmiMegat Mohd Azman AdzmiNo ratings yet
- K19 - Kuliah HipertensiDocument49 pagesK19 - Kuliah HipertensiRahma Dhita FitrianiNo ratings yet
- Krisis HipertensiDocument27 pagesKrisis HipertensiAmanda Padma100% (1)
- HCVDDocument99 pagesHCVDMiguel CuevasNo ratings yet
- HypertensionDocument42 pagesHypertensionMohamed BamashmoosNo ratings yet
- Laporan Pendahuluan Hipertensi Emergency: Disusun Oleh: Annisa Yuli Pratiwi NIM. SN171024Document20 pagesLaporan Pendahuluan Hipertensi Emergency: Disusun Oleh: Annisa Yuli Pratiwi NIM. SN171024Annisa Yuli PratiwiNo ratings yet
- Hypertensive CrisisDocument23 pagesHypertensive CrisisJayarani Ashok100% (1)
- Askep HipertensiDocument23 pagesAskep HipertensiTikaNo ratings yet
- Ipertensione Arteriosa PolmonareDocument33 pagesIpertensione Arteriosa PolmonareCarlo MaxiaNo ratings yet
- 03 AntihypertensiveDocument89 pages03 Antihypertensive2nnfpjy5yvNo ratings yet
- Drugs Acting in CVSDocument63 pagesDrugs Acting in CVSMeghan Norico Cristuta100% (1)
- Secondary HypertensionDocument34 pagesSecondary HypertensionSumaiya AlhaliyahNo ratings yet
- Chapter 33 HypertensionDocument5 pagesChapter 33 HypertensiongytmbiuiNo ratings yet
- Hipertensi: DR M. Arman Nasution SPPDDocument101 pagesHipertensi: DR M. Arman Nasution SPPDDian PuspaNo ratings yet
- Classification: HypertensionDocument13 pagesClassification: HypertensiontermskipopNo ratings yet
- HTNDocument54 pagesHTNapi-232466940No ratings yet
- HTN Majdi FinalDocument87 pagesHTN Majdi FinalYaacoub ChahineNo ratings yet
- 5 Nutrition Therapy For Cardiovascular DiseasesDocument74 pages5 Nutrition Therapy For Cardiovascular Diseaseskarinablanca adranedaNo ratings yet
- Week 2 Blpressoureoduph - 20 Februari 2012week 2 Blpressoureoduph - 20 Februari 2012Document43 pagesWeek 2 Blpressoureoduph - 20 Februari 2012week 2 Blpressoureoduph - 20 Februari 2012Maria Dini AdmiratiNo ratings yet
- Hypertension: Detection, Evaluation and Non-Pharmacologic InterventionDocument42 pagesHypertension: Detection, Evaluation and Non-Pharmacologic InterventionLullaby HunterNo ratings yet
- Pharma Notes 17-18Document4 pagesPharma Notes 17-18flixiexpressNo ratings yet
- CA ReviewerDocument16 pagesCA ReviewerJheanAlphonsineT.MeansNo ratings yet
- CardioDocument9 pagesCardioVirgilio Reyes ManuelNo ratings yet
- Vasucular DiseasesDocument43 pagesVasucular DiseasesSufiyan AbduramanNo ratings yet
- Patofisiologi HipertensiDocument18 pagesPatofisiologi HipertensiZebyyNo ratings yet
- 11A Drugs Acting On The Cardiovascular SystemDocument85 pages11A Drugs Acting On The Cardiovascular SystemJaps De la CruzNo ratings yet
- Hypertensiveemergencies RullDocument60 pagesHypertensiveemergencies RullagustinaNo ratings yet
- General Internal Medicine Hour: HypertensionDocument33 pagesGeneral Internal Medicine Hour: HypertensionRadley Jed C. PelagioNo ratings yet
- HypertensionDocument39 pagesHypertensionapi-648595816No ratings yet
- Pa Tho Physiology of HypertensionDocument2 pagesPa Tho Physiology of HypertensionBenedict SyNo ratings yet
- Arterial HypertentionDocument32 pagesArterial HypertentionNijesh KannaNo ratings yet
- PathophysiologyDocument24 pagesPathophysiologyVikash KushwahaNo ratings yet
- BAB 2 OkDocument19 pagesBAB 2 OkHelny TariganNo ratings yet
- Cardiovascular DiseaseDocument14 pagesCardiovascular DiseasenonameNo ratings yet
- Ex, 2a, B, C, 3, 4a, B, Pages 50-51 (SB) 2a.: 1. Most Advertising in Ancient Times Was Word-Of-Mouth, That Is, PeopleDocument4 pagesEx, 2a, B, C, 3, 4a, B, Pages 50-51 (SB) 2a.: 1. Most Advertising in Ancient Times Was Word-Of-Mouth, That Is, PeopleRodriguez Vivanco Kevin DanielNo ratings yet
- Disappearing LanguagesDocument4 pagesDisappearing LanguagesRodriguez Vivanco Kevin DanielNo ratings yet
- Англ тести фармDocument138 pagesАнгл тести фармRodriguez Vivanco Kevin DanielNo ratings yet
- Pathphys ModuleDocument102 pagesPathphys ModuleRodriguez Vivanco Kevin DanielNo ratings yet
- 6 Krok GitDocument14 pages6 Krok GitRodriguez Vivanco Kevin DanielNo ratings yet
- Red Blood Cells PathologyDocument47 pagesRed Blood Cells PathologyRodriguez Vivanco Kevin DanielNo ratings yet
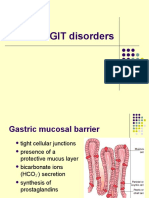
- 14-GIT and LiverDocument36 pages14-GIT and LiverRodriguez Vivanco Kevin DanielNo ratings yet
- Example of Practical Work 3Document5 pagesExample of Practical Work 3Rodriguez Vivanco Kevin DanielNo ratings yet
- Pathophysiology of Endocrine SystemDocument37 pagesPathophysiology of Endocrine SystemRodriguez Vivanco Kevin DanielNo ratings yet
- Pathology of Pregnancy and Delivery: Lecture On Pathological Anatomy For The 3-rd Year StudentsDocument35 pagesPathology of Pregnancy and Delivery: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
- Liver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsDocument27 pagesLiver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
- 13 - Lung PathologyDocument38 pages13 - Lung PathologyRodriguez Vivanco Kevin DanielNo ratings yet
- Endocrine Pathology: Lecture On Pathomorphology For 3-rd Year StudentsDocument44 pagesEndocrine Pathology: Lecture On Pathomorphology For 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
- Topic - Operation, AnesthesiaDocument5 pagesTopic - Operation, AnesthesiaRodriguez Vivanco Kevin DanielNo ratings yet
- Tuberculosis:: - Classification - Morphology - Clinical FeaturesDocument28 pagesTuberculosis:: - Classification - Morphology - Clinical FeaturesRodriguez Vivanco Kevin DanielNo ratings yet
- Age PeriodsDocument12 pagesAge PeriodsRodriguez Vivanco Kevin DanielNo ratings yet
- Nursing Practice 2019Document87 pagesNursing Practice 2019Rodriguez Vivanco Kevin DanielNo ratings yet
- Nanorobots The Heart SurgeonDocument7 pagesNanorobots The Heart SurgeonPoonguzhali MadhavanNo ratings yet
- Roman Medicine: (Santiago, Posadas, Mallari)Document6 pagesRoman Medicine: (Santiago, Posadas, Mallari)Monsour SalazarNo ratings yet
- Body Fluids and CirculationsDocument14 pagesBody Fluids and CirculationsNikhil SharmaNo ratings yet
- Hypoxia and Its Types SaleemDocument19 pagesHypoxia and Its Types SaleemSanwan NaichNo ratings yet
- Histology of Circulatory SystemDocument82 pagesHistology of Circulatory SystemFebriana Ramdhani SNo ratings yet
- Blair ScienceDocument6 pagesBlair ScienceJanelle SatinNo ratings yet
- EDTA Chelation Therapy ArticlesDocument46 pagesEDTA Chelation Therapy ArticlesBhalchandra Gokhale100% (1)
- New PE 1 MODULEDocument52 pagesNew PE 1 MODULECyrus De LeonNo ratings yet
- Technology Integration Lesson Plan 1Document4 pagesTechnology Integration Lesson Plan 1api-320427440No ratings yet
- Life ProcessesDocument2 pagesLife ProcessesAnkita AgarwalNo ratings yet
- Cambridge International General Certificate of Secondary EducationDocument20 pagesCambridge International General Certificate of Secondary EducationLast MadanhireNo ratings yet
- Anatomy Review: Blood Vessel Structure & Function: Page 1. Introduction Page 2. GoalsDocument6 pagesAnatomy Review: Blood Vessel Structure & Function: Page 1. Introduction Page 2. GoalsUta Provinsiana SukmaraNo ratings yet
- Pulmo Physio-Transport 2Document35 pagesPulmo Physio-Transport 2Mich Therese AbejeroNo ratings yet
- U N I T I I Diseases of Organ Systems 1 4 8: Escherichia ColiDocument25 pagesU N I T I I Diseases of Organ Systems 1 4 8: Escherichia ColiHerbert YNo ratings yet
- O Level 5090 Scheme of WorkDocument50 pagesO Level 5090 Scheme of WorkBalakrishnan Marappan100% (2)
- Preoperative Management of Arteriovenous Fistula (AVF) For HemodialysisDocument14 pagesPreoperative Management of Arteriovenous Fistula (AVF) For HemodialysisRafael CellestineNo ratings yet
- Parts of The HeartDocument18 pagesParts of The HeartCHRISTOPHER FAYLONNo ratings yet
- Alcapa FinalDocument22 pagesAlcapa FinalCardiacCareCenterMCHNo ratings yet
- Kami Export - Cardiovascular System Lecture Outline 1st PeriodDocument16 pagesKami Export - Cardiovascular System Lecture Outline 1st PeriodJada NovakNo ratings yet
- Laboratory Investigation in Respiratory DiseasesDocument46 pagesLaboratory Investigation in Respiratory DiseasesWin Indra Wicaksono100% (2)
- 2nd Day OF Exams in 1st QTR 2016Document9 pages2nd Day OF Exams in 1st QTR 2016John RoasaNo ratings yet
- Https - App - Oswaalbooks.com - Download - Sample-Qp - Subsolution - 411SAP 4Document11 pagesHttps - App - Oswaalbooks.com - Download - Sample-Qp - Subsolution - 411SAP 4AdityaNo ratings yet
- Standard Five Term - ScienceDocument40 pagesStandard Five Term - ScienceJigna PatelNo ratings yet
- Hempel 2020 Sci30 Bio Video SheetsDocument11 pagesHempel 2020 Sci30 Bio Video SheetsticoninxNo ratings yet
- Describe Effects of Tar and Carcinogens in Smoke On The Respiratory SystemDocument4 pagesDescribe Effects of Tar and Carcinogens in Smoke On The Respiratory SystemNathuAndrewsNo ratings yet
- Section 5. Atherosclerotic Peripheral Vascular Disease and Aortic AneurysmDocument23 pagesSection 5. Atherosclerotic Peripheral Vascular Disease and Aortic AneurysmsidoniavidicanNo ratings yet
- Case Study Secon EditDocument42 pagesCase Study Secon EditAbegail PolicarpioNo ratings yet
- A Case Study On Cerebrovascular Accident With Kristy Garvez Genward 2023 Goods Na Guro NiDocument61 pagesA Case Study On Cerebrovascular Accident With Kristy Garvez Genward 2023 Goods Na Guro NiJoshua GrafiaNo ratings yet