
Basic Mechanism of Disease Nutritonal Persepectives
Basic Mechanism of Disease Nutritonal Persepectives
You might also like
- Industrial Galactomannan Polysaccharides - CRC Press (2011) - N. K. MathurDocument179 pagesIndustrial Galactomannan Polysaccharides - CRC Press (2011) - N. K. MathurMichelle AzevedoNo ratings yet
- Nutritiondiettherapy Lectureprelimstomidterm 191112061026Document138 pagesNutritiondiettherapy Lectureprelimstomidterm 191112061026Augustine chandigaNo ratings yet
- CarbohydratesDocument25 pagesCarbohydratesSpa DNo ratings yet
- Macronutrients PDocument83 pagesMacronutrients PBelayneh Tadesse100% (2)
- Role of Carbohydrate in Health and DiseasesDocument41 pagesRole of Carbohydrate in Health and Diseasesuttarasingh100% (2)
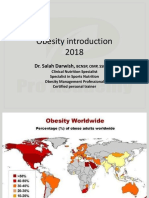
- Obesity Introduction 2018: Dr. Salah DarwishDocument17 pagesObesity Introduction 2018: Dr. Salah DarwishMahmoud ShabbanNo ratings yet
- G10 Qtr2 BiomoleculesDocument35 pagesG10 Qtr2 BiomoleculesclaudiaNo ratings yet
- Carbohydrate ChemistryDocument58 pagesCarbohydrate ChemistryAleeha MaryamNo ratings yet
- NCM 105 Lesson 1 - 1 - MacronutrientsDocument44 pagesNCM 105 Lesson 1 - 1 - MacronutrientspgumbanNo ratings yet
- Nutrition and MetabolismDocument179 pagesNutrition and MetabolismTuTit100% (1)
- LECT 1&2 - CHO & Energy BalanceDocument22 pagesLECT 1&2 - CHO & Energy BalancenorshaheeraNo ratings yet
- Nutrition and MetabolismDocument179 pagesNutrition and Metabolismnursereview100% (9)
- 6 BiomoleculesDocument78 pages6 BiomoleculesPrecious Ryza G. BautistaNo ratings yet
- 2 CarbohydratesDocument36 pages2 Carbohydratestalidah binselimNo ratings yet
- CarbohydratesDocument76 pagesCarbohydratesMaria HarisNo ratings yet
- Student Copy CARBSDocument46 pagesStudent Copy CARBSRomeo DiestaNo ratings yet
- ChoDocument44 pagesChosunielgowdaNo ratings yet
- Handouts - CarbohydratesDocument9 pagesHandouts - CarbohydratesJerrold CruzNo ratings yet
- Carbohydrates: Jameston S. Adorable, RND InstructorDocument51 pagesCarbohydrates: Jameston S. Adorable, RND InstructorMj AñascoNo ratings yet
- CarbohydratesDocument41 pagesCarbohydratesStrange Me100% (3)
- Carbohydrate Metabolism 08-02-24Document113 pagesCarbohydrate Metabolism 08-02-24Saloni SaloniNo ratings yet
- Nmfa EbookDocument70 pagesNmfa EbookFrank YagaNo ratings yet
- CH 7Document29 pagesCH 7Àhmâd ÂqéłNo ratings yet
- Chapter 4 - CARBOHYDRATESDocument47 pagesChapter 4 - CARBOHYDRATESKinjal100% (1)
- Ilmu Gizi Dasar - MakroDocument69 pagesIlmu Gizi Dasar - MakroliaNo ratings yet
- 3 Macronutrients Part 2 - CarbohydratesDocument10 pages3 Macronutrients Part 2 - CarbohydratesHarmanveer BrarNo ratings yet
- Digestion of Corbohydrate Semester 7thDocument52 pagesDigestion of Corbohydrate Semester 7thFadi SalahNo ratings yet
- Unit TwoDocument31 pagesUnit TwoRenad Q.No ratings yet
- Digestion and Absorption By-Dr. Suntia Saxena Part 2Document41 pagesDigestion and Absorption By-Dr. Suntia Saxena Part 2Divya AgarawalNo ratings yet
- NDT Module 1Document97 pagesNDT Module 1Fhei Lya Dee TioNo ratings yet
- Carbohydrates: Simple Sugars and Complex ChainsDocument44 pagesCarbohydrates: Simple Sugars and Complex ChainsBundi Gonzalez MartinNo ratings yet
- RSC Digestive SystemDocument4 pagesRSC Digestive SystemDan Rey OsiasNo ratings yet
- Chapter 4 CarbohydratesDocument24 pagesChapter 4 Carbohydratesgus peepNo ratings yet
- Charbohydrate: Unit - IiDocument8 pagesCharbohydrate: Unit - IiHemant SharmaNo ratings yet
- Nutrition Nursing: CarbohydratesDocument36 pagesNutrition Nursing: CarbohydratesAngelyka Nicole Bengco DavidNo ratings yet
- Chap 4Document48 pagesChap 4vchan318No ratings yet
- Human Nutrition: DR Kim Bell-Anderson School of Life and Environmental Sciences, Charles Perkins CentreDocument29 pagesHuman Nutrition: DR Kim Bell-Anderson School of Life and Environmental Sciences, Charles Perkins Centresebba3112No ratings yet
- CarbohydrateDocument17 pagesCarbohydratesahabchauhan611No ratings yet
- CarbsDocument40 pagesCarbsAnonymous eDD0YqzPMNo ratings yet
- Nutritional Importance of Carbohydrates FinalDocument6 pagesNutritional Importance of Carbohydrates FinalMuqeet ButtNo ratings yet
- Biochemical Digestive and Absorption Process of Dietary-Sunarti-Biochemistry (2015)Document36 pagesBiochemical Digestive and Absorption Process of Dietary-Sunarti-Biochemistry (2015)nayanikatesalonikaNo ratings yet
- Nutrition LectureDocument109 pagesNutrition LectureEshetu MollaNo ratings yet
- Functions of CarbohydratesDocument14 pagesFunctions of CarbohydratesRenu SharmaNo ratings yet
- CHEL 4248 Food Chemistry (2023)Document75 pagesCHEL 4248 Food Chemistry (2023)John Fritz FestejoNo ratings yet
- Chapter 4 - CARBOHYDRATESDocument47 pagesChapter 4 - CARBOHYDRATESGlenn ClementeNo ratings yet
- 2, CARBOHYDRATE MPH 2023 (1) - 1Document148 pages2, CARBOHYDRATE MPH 2023 (1) - 1NaolShamsuNo ratings yet
- Carbohydrates, Sugars, Starches and Fiber: © 2010 Pearson Education, IncDocument54 pagesCarbohydrates, Sugars, Starches and Fiber: © 2010 Pearson Education, IncRafi Noval100% (1)
- 9 Nutrition-and-dietetics-IntroDocument51 pages9 Nutrition-and-dietetics-IntroPratiksha JhareeNo ratings yet
- 2 - Carbohydrates (Part 2)Document25 pages2 - Carbohydrates (Part 2)Sean Polo MallariNo ratings yet
- 2 Digestion and Absorption PDFDocument54 pages2 Digestion and Absorption PDFAhmad Akram NatshehNo ratings yet
- The Gastrointestinal System: Digestion and Absorption: Irawan Yusuf Department of PhysiologyDocument20 pagesThe Gastrointestinal System: Digestion and Absorption: Irawan Yusuf Department of PhysiologyagungNo ratings yet
- Digestion, Absorption and Metabolism of CarbohydratesDocument28 pagesDigestion, Absorption and Metabolism of CarbohydratesIzzuddienNo ratings yet
- CarbohydratesDocument44 pagesCarbohydratesApril Jean Cahoy100% (4)
- Food Science Word SoftDocument8 pagesFood Science Word SoftZipporah D. NideaNo ratings yet
- Carbohydrate DigestionDocument36 pagesCarbohydrate DigestionardiansyahNo ratings yet
- 6 - Macromolecules - 3UDocument47 pages6 - Macromolecules - 3UPT - 09SL 728582 John Fraser SSNo ratings yet
- Biochemistry Midterm Carbohydrates: ClassificationsDocument21 pagesBiochemistry Midterm Carbohydrates: ClassificationsArah Lyn ApiagNo ratings yet
- Digestion in RuminantsDocument59 pagesDigestion in RuminantsPrakash PanthiNo ratings yet
- Chap 2 Unit 2Document39 pagesChap 2 Unit 2harshit khareNo ratings yet
- The Science of Tastes - Introduction to Food Chemistry for Kids | Children's Chemistry BooksFrom EverandThe Science of Tastes - Introduction to Food Chemistry for Kids | Children's Chemistry BooksNo ratings yet
- Penjelasan Praktikum KardiovaskulerDocument54 pagesPenjelasan Praktikum KardiovaskulerQuswah MaharaniNo ratings yet
- Obat-Obatan KardiovaskulerDocument51 pagesObat-Obatan KardiovaskulerQuswah MaharaniNo ratings yet
- AntibioticsDocument9 pagesAntibioticsQuswah MaharaniNo ratings yet
- The Digestive System: Physiology Departement Medical Faculty, Hasanuddin UniversityDocument71 pagesThe Digestive System: Physiology Departement Medical Faculty, Hasanuddin UniversityQuswah MaharaniNo ratings yet
- 2.glycolysis Kreb O.PDocument33 pages2.glycolysis Kreb O.PAMad SiDdiqNo ratings yet
- Digestion: Proteins Fats CarbohydratesDocument42 pagesDigestion: Proteins Fats CarbohydratesVal Kay HeikeNo ratings yet
- Feedback Mechanisms 2Document14 pagesFeedback Mechanisms 2Jade Mark PantuaNo ratings yet
- Setiadi 2019 J. Phys. Conf. Ser. 1146 012009Document8 pagesSetiadi 2019 J. Phys. Conf. Ser. 1146 012009Nelli Nur Indah SariNo ratings yet
- In Vitro Model For Anti Diabetic AssemntDocument4 pagesIn Vitro Model For Anti Diabetic AssemntHaleema SultanNo ratings yet
- Cmcchapter23 100613135130 Phpapp02 PDFDocument104 pagesCmcchapter23 100613135130 Phpapp02 PDFRicki HanNo ratings yet
- Recent Advances in The Production and Applications of Ellagic Acid and Its Derivatives. A ReviewDocument20 pagesRecent Advances in The Production and Applications of Ellagic Acid and Its Derivatives. A ReviewSandraNo ratings yet
- Cold Drink AnalysisDocument19 pagesCold Drink Analysisravi50% (2)
- Exam Qs HWDocument11 pagesExam Qs HWMiguel Oubiña SánchezNo ratings yet
- Citric Acid-PEDDocument32 pagesCitric Acid-PEDJomhel CalluengNo ratings yet
- 4753-Article Text-10548-3-10-20191214Document5 pages4753-Article Text-10548-3-10-20191214MARY ROSE HERNANDEZNo ratings yet
- 3.1.1 List The Macronutrients and Micronutrients: Energy SystemsDocument42 pages3.1.1 List The Macronutrients and Micronutrients: Energy Systemslauzark gashbellNo ratings yet
- Intertek Article - Honey Authenticity - SonderdruckDocument8 pagesIntertek Article - Honey Authenticity - SonderdruckmaralexNo ratings yet
- Stryer Chapter 9 CarbohydratesDocument5 pagesStryer Chapter 9 CarbohydratesDyamond SantiagoNo ratings yet
- Physical and Chemical Principles CompiledDocument75 pagesPhysical and Chemical Principles Compiledsiams fadnierhsaNo ratings yet
- Home WorkDocument8 pagesHome Work송준혁No ratings yet
- Sbt1102 - Biochemistry Unit 1 CarbohydratesDocument22 pagesSbt1102 - Biochemistry Unit 1 CarbohydratesJeremy CorrenNo ratings yet
- 4 - Choubane S., Khelil O. Et Cheba B. 2015, African Journal of BiotechnologyDocument6 pages4 - Choubane S., Khelil O. Et Cheba B. 2015, African Journal of BiotechnologyOmar KHELILNo ratings yet
- AgappeDocument1 pageAgappeNur CholisNo ratings yet
- AP EdCET Syllabus and Exam PatternDocument28 pagesAP EdCET Syllabus and Exam PatterngayathriNo ratings yet
- Parameters of Quality ControlDocument36 pagesParameters of Quality ControlAngelo Jude CobachaNo ratings yet
- 5090 Workshop 2024 by Miss Iram HabibDocument39 pages5090 Workshop 2024 by Miss Iram Habibmalikrayan76No ratings yet
- Bitter Melon Bioactive Composition and Health Benefits A Review - Tan Et Al. 2015Document23 pagesBitter Melon Bioactive Composition and Health Benefits A Review - Tan Et Al. 2015Fatima HerreraNo ratings yet
- Biology Experiment Glucose and Carbon Dioxide Fermentation 8642-37602-1-PBDocument4 pagesBiology Experiment Glucose and Carbon Dioxide Fermentation 8642-37602-1-PBmarcelocarcamoNo ratings yet
- AAPS PharmSciTech Volume 10, Number 2 6.09a PDFDocument386 pagesAAPS PharmSciTech Volume 10, Number 2 6.09a PDFAchi'fsc'No ratings yet
- Ginger Rhizomes (Zingiber Officinale) A Spice With Multiple Healthbeneficial PotentialsDocument11 pagesGinger Rhizomes (Zingiber Officinale) A Spice With Multiple Healthbeneficial PotentialsRabeea NasirNo ratings yet
- CBSE Class XII Chemistry ProjectDocument23 pagesCBSE Class XII Chemistry Projecttrishabhagawati93% (14)
- 1 - Photosynthesis and AssimilationDocument19 pages1 - Photosynthesis and AssimilationJasmine VS032689No ratings yet
- A B C D Biology: Nama Pelajar: Kelas: MarkahDocument4 pagesA B C D Biology: Nama Pelajar: Kelas: Markahke2No ratings yet


























































































Download as pptx, pdf, or txt
You might also like
- Industrial Galactomannan Polysaccharides - CRC Press (2011) - N. K. MathurDocument179 pagesIndustrial Galactomannan Polysaccharides - CRC Press (2011) - N. K. MathurMichelle AzevedoNo ratings yet
- Nutritiondiettherapy Lectureprelimstomidterm 191112061026Document138 pagesNutritiondiettherapy Lectureprelimstomidterm 191112061026Augustine chandigaNo ratings yet
- CarbohydratesDocument25 pagesCarbohydratesSpa DNo ratings yet
- Macronutrients PDocument83 pagesMacronutrients PBelayneh Tadesse100% (2)
- Role of Carbohydrate in Health and DiseasesDocument41 pagesRole of Carbohydrate in Health and Diseasesuttarasingh100% (2)
- Obesity Introduction 2018: Dr. Salah DarwishDocument17 pagesObesity Introduction 2018: Dr. Salah DarwishMahmoud ShabbanNo ratings yet
- G10 Qtr2 BiomoleculesDocument35 pagesG10 Qtr2 BiomoleculesclaudiaNo ratings yet
- Carbohydrate ChemistryDocument58 pagesCarbohydrate ChemistryAleeha MaryamNo ratings yet
- NCM 105 Lesson 1 - 1 - MacronutrientsDocument44 pagesNCM 105 Lesson 1 - 1 - MacronutrientspgumbanNo ratings yet
- Nutrition and MetabolismDocument179 pagesNutrition and MetabolismTuTit100% (1)
- LECT 1&2 - CHO & Energy BalanceDocument22 pagesLECT 1&2 - CHO & Energy BalancenorshaheeraNo ratings yet
- Nutrition and MetabolismDocument179 pagesNutrition and Metabolismnursereview100% (9)
- 6 BiomoleculesDocument78 pages6 BiomoleculesPrecious Ryza G. BautistaNo ratings yet
- 2 CarbohydratesDocument36 pages2 Carbohydratestalidah binselimNo ratings yet
- CarbohydratesDocument76 pagesCarbohydratesMaria HarisNo ratings yet
- Student Copy CARBSDocument46 pagesStudent Copy CARBSRomeo DiestaNo ratings yet
- ChoDocument44 pagesChosunielgowdaNo ratings yet
- Handouts - CarbohydratesDocument9 pagesHandouts - CarbohydratesJerrold CruzNo ratings yet
- Carbohydrates: Jameston S. Adorable, RND InstructorDocument51 pagesCarbohydrates: Jameston S. Adorable, RND InstructorMj AñascoNo ratings yet
- CarbohydratesDocument41 pagesCarbohydratesStrange Me100% (3)
- Carbohydrate Metabolism 08-02-24Document113 pagesCarbohydrate Metabolism 08-02-24Saloni SaloniNo ratings yet
- Nmfa EbookDocument70 pagesNmfa EbookFrank YagaNo ratings yet
- CH 7Document29 pagesCH 7Àhmâd ÂqéłNo ratings yet
- Chapter 4 - CARBOHYDRATESDocument47 pagesChapter 4 - CARBOHYDRATESKinjal100% (1)
- Ilmu Gizi Dasar - MakroDocument69 pagesIlmu Gizi Dasar - MakroliaNo ratings yet
- 3 Macronutrients Part 2 - CarbohydratesDocument10 pages3 Macronutrients Part 2 - CarbohydratesHarmanveer BrarNo ratings yet
- Digestion of Corbohydrate Semester 7thDocument52 pagesDigestion of Corbohydrate Semester 7thFadi SalahNo ratings yet
- Unit TwoDocument31 pagesUnit TwoRenad Q.No ratings yet
- Digestion and Absorption By-Dr. Suntia Saxena Part 2Document41 pagesDigestion and Absorption By-Dr. Suntia Saxena Part 2Divya AgarawalNo ratings yet
- NDT Module 1Document97 pagesNDT Module 1Fhei Lya Dee TioNo ratings yet
- Carbohydrates: Simple Sugars and Complex ChainsDocument44 pagesCarbohydrates: Simple Sugars and Complex ChainsBundi Gonzalez MartinNo ratings yet
- RSC Digestive SystemDocument4 pagesRSC Digestive SystemDan Rey OsiasNo ratings yet
- Chapter 4 CarbohydratesDocument24 pagesChapter 4 Carbohydratesgus peepNo ratings yet
- Charbohydrate: Unit - IiDocument8 pagesCharbohydrate: Unit - IiHemant SharmaNo ratings yet
- Nutrition Nursing: CarbohydratesDocument36 pagesNutrition Nursing: CarbohydratesAngelyka Nicole Bengco DavidNo ratings yet
- Chap 4Document48 pagesChap 4vchan318No ratings yet
- Human Nutrition: DR Kim Bell-Anderson School of Life and Environmental Sciences, Charles Perkins CentreDocument29 pagesHuman Nutrition: DR Kim Bell-Anderson School of Life and Environmental Sciences, Charles Perkins Centresebba3112No ratings yet
- CarbohydrateDocument17 pagesCarbohydratesahabchauhan611No ratings yet
- CarbsDocument40 pagesCarbsAnonymous eDD0YqzPMNo ratings yet
- Nutritional Importance of Carbohydrates FinalDocument6 pagesNutritional Importance of Carbohydrates FinalMuqeet ButtNo ratings yet
- Biochemical Digestive and Absorption Process of Dietary-Sunarti-Biochemistry (2015)Document36 pagesBiochemical Digestive and Absorption Process of Dietary-Sunarti-Biochemistry (2015)nayanikatesalonikaNo ratings yet
- Nutrition LectureDocument109 pagesNutrition LectureEshetu MollaNo ratings yet
- Functions of CarbohydratesDocument14 pagesFunctions of CarbohydratesRenu SharmaNo ratings yet
- CHEL 4248 Food Chemistry (2023)Document75 pagesCHEL 4248 Food Chemistry (2023)John Fritz FestejoNo ratings yet
- Chapter 4 - CARBOHYDRATESDocument47 pagesChapter 4 - CARBOHYDRATESGlenn ClementeNo ratings yet
- 2, CARBOHYDRATE MPH 2023 (1) - 1Document148 pages2, CARBOHYDRATE MPH 2023 (1) - 1NaolShamsuNo ratings yet
- Carbohydrates, Sugars, Starches and Fiber: © 2010 Pearson Education, IncDocument54 pagesCarbohydrates, Sugars, Starches and Fiber: © 2010 Pearson Education, IncRafi Noval100% (1)
- 9 Nutrition-and-dietetics-IntroDocument51 pages9 Nutrition-and-dietetics-IntroPratiksha JhareeNo ratings yet
- 2 - Carbohydrates (Part 2)Document25 pages2 - Carbohydrates (Part 2)Sean Polo MallariNo ratings yet
- 2 Digestion and Absorption PDFDocument54 pages2 Digestion and Absorption PDFAhmad Akram NatshehNo ratings yet
- The Gastrointestinal System: Digestion and Absorption: Irawan Yusuf Department of PhysiologyDocument20 pagesThe Gastrointestinal System: Digestion and Absorption: Irawan Yusuf Department of PhysiologyagungNo ratings yet
- Digestion, Absorption and Metabolism of CarbohydratesDocument28 pagesDigestion, Absorption and Metabolism of CarbohydratesIzzuddienNo ratings yet
- CarbohydratesDocument44 pagesCarbohydratesApril Jean Cahoy100% (4)
- Food Science Word SoftDocument8 pagesFood Science Word SoftZipporah D. NideaNo ratings yet
- Carbohydrate DigestionDocument36 pagesCarbohydrate DigestionardiansyahNo ratings yet
- 6 - Macromolecules - 3UDocument47 pages6 - Macromolecules - 3UPT - 09SL 728582 John Fraser SSNo ratings yet
- Biochemistry Midterm Carbohydrates: ClassificationsDocument21 pagesBiochemistry Midterm Carbohydrates: ClassificationsArah Lyn ApiagNo ratings yet
- Digestion in RuminantsDocument59 pagesDigestion in RuminantsPrakash PanthiNo ratings yet
- Chap 2 Unit 2Document39 pagesChap 2 Unit 2harshit khareNo ratings yet
- The Science of Tastes - Introduction to Food Chemistry for Kids | Children's Chemistry BooksFrom EverandThe Science of Tastes - Introduction to Food Chemistry for Kids | Children's Chemistry BooksNo ratings yet
- Penjelasan Praktikum KardiovaskulerDocument54 pagesPenjelasan Praktikum KardiovaskulerQuswah MaharaniNo ratings yet
- Obat-Obatan KardiovaskulerDocument51 pagesObat-Obatan KardiovaskulerQuswah MaharaniNo ratings yet
- AntibioticsDocument9 pagesAntibioticsQuswah MaharaniNo ratings yet
- The Digestive System: Physiology Departement Medical Faculty, Hasanuddin UniversityDocument71 pagesThe Digestive System: Physiology Departement Medical Faculty, Hasanuddin UniversityQuswah MaharaniNo ratings yet
- 2.glycolysis Kreb O.PDocument33 pages2.glycolysis Kreb O.PAMad SiDdiqNo ratings yet
- Digestion: Proteins Fats CarbohydratesDocument42 pagesDigestion: Proteins Fats CarbohydratesVal Kay HeikeNo ratings yet
- Feedback Mechanisms 2Document14 pagesFeedback Mechanisms 2Jade Mark PantuaNo ratings yet
- Setiadi 2019 J. Phys. Conf. Ser. 1146 012009Document8 pagesSetiadi 2019 J. Phys. Conf. Ser. 1146 012009Nelli Nur Indah SariNo ratings yet
- In Vitro Model For Anti Diabetic AssemntDocument4 pagesIn Vitro Model For Anti Diabetic AssemntHaleema SultanNo ratings yet
- Cmcchapter23 100613135130 Phpapp02 PDFDocument104 pagesCmcchapter23 100613135130 Phpapp02 PDFRicki HanNo ratings yet
- Recent Advances in The Production and Applications of Ellagic Acid and Its Derivatives. A ReviewDocument20 pagesRecent Advances in The Production and Applications of Ellagic Acid and Its Derivatives. A ReviewSandraNo ratings yet
- Cold Drink AnalysisDocument19 pagesCold Drink Analysisravi50% (2)
- Exam Qs HWDocument11 pagesExam Qs HWMiguel Oubiña SánchezNo ratings yet
- Citric Acid-PEDDocument32 pagesCitric Acid-PEDJomhel CalluengNo ratings yet
- 4753-Article Text-10548-3-10-20191214Document5 pages4753-Article Text-10548-3-10-20191214MARY ROSE HERNANDEZNo ratings yet
- 3.1.1 List The Macronutrients and Micronutrients: Energy SystemsDocument42 pages3.1.1 List The Macronutrients and Micronutrients: Energy Systemslauzark gashbellNo ratings yet
- Intertek Article - Honey Authenticity - SonderdruckDocument8 pagesIntertek Article - Honey Authenticity - SonderdruckmaralexNo ratings yet
- Stryer Chapter 9 CarbohydratesDocument5 pagesStryer Chapter 9 CarbohydratesDyamond SantiagoNo ratings yet
- Physical and Chemical Principles CompiledDocument75 pagesPhysical and Chemical Principles Compiledsiams fadnierhsaNo ratings yet
- Home WorkDocument8 pagesHome Work송준혁No ratings yet
- Sbt1102 - Biochemistry Unit 1 CarbohydratesDocument22 pagesSbt1102 - Biochemistry Unit 1 CarbohydratesJeremy CorrenNo ratings yet
- 4 - Choubane S., Khelil O. Et Cheba B. 2015, African Journal of BiotechnologyDocument6 pages4 - Choubane S., Khelil O. Et Cheba B. 2015, African Journal of BiotechnologyOmar KHELILNo ratings yet
- AgappeDocument1 pageAgappeNur CholisNo ratings yet
- AP EdCET Syllabus and Exam PatternDocument28 pagesAP EdCET Syllabus and Exam PatterngayathriNo ratings yet
- Parameters of Quality ControlDocument36 pagesParameters of Quality ControlAngelo Jude CobachaNo ratings yet
- 5090 Workshop 2024 by Miss Iram HabibDocument39 pages5090 Workshop 2024 by Miss Iram Habibmalikrayan76No ratings yet
- Bitter Melon Bioactive Composition and Health Benefits A Review - Tan Et Al. 2015Document23 pagesBitter Melon Bioactive Composition and Health Benefits A Review - Tan Et Al. 2015Fatima HerreraNo ratings yet
- Biology Experiment Glucose and Carbon Dioxide Fermentation 8642-37602-1-PBDocument4 pagesBiology Experiment Glucose and Carbon Dioxide Fermentation 8642-37602-1-PBmarcelocarcamoNo ratings yet
- AAPS PharmSciTech Volume 10, Number 2 6.09a PDFDocument386 pagesAAPS PharmSciTech Volume 10, Number 2 6.09a PDFAchi'fsc'No ratings yet
- Ginger Rhizomes (Zingiber Officinale) A Spice With Multiple Healthbeneficial PotentialsDocument11 pagesGinger Rhizomes (Zingiber Officinale) A Spice With Multiple Healthbeneficial PotentialsRabeea NasirNo ratings yet
- CBSE Class XII Chemistry ProjectDocument23 pagesCBSE Class XII Chemistry Projecttrishabhagawati93% (14)
- 1 - Photosynthesis and AssimilationDocument19 pages1 - Photosynthesis and AssimilationJasmine VS032689No ratings yet
- A B C D Biology: Nama Pelajar: Kelas: MarkahDocument4 pagesA B C D Biology: Nama Pelajar: Kelas: Markahke2No ratings yet