Download as pptx, pdf, or txt
You might also like
- HA-RLE-WS # 10 Assessing Nutritional StatusDocument4 pagesHA-RLE-WS # 10 Assessing Nutritional StatusJULIE ANNE CORTEZNo ratings yet
- Miracle of Lymph - John DouillardDocument41 pagesMiracle of Lymph - John DouillardAnne Marie Surlin100% (6)
- Lymphatic SystemDocument4 pagesLymphatic Systempriya garciaNo ratings yet
- Case Study Pressure Ulcer StudentDocument8 pagesCase Study Pressure Ulcer StudentKuro HanabusaNo ratings yet
- Cast and BracesDocument58 pagesCast and BracesNikki M. Arapol100% (1)
- P.A. 1Document6 pagesP.A. 1SamSarah BongolanNo ratings yet
- Principles of Patient PositioningDocument62 pagesPrinciples of Patient PositioningMelody JusticeNo ratings yet
- Nursing Care Plan: Interaction Immediate Cause Goal: Effectivenes SDocument6 pagesNursing Care Plan: Interaction Immediate Cause Goal: Effectivenes SCatherine Kaye Marquez RoxasNo ratings yet
- Assessment Tool - Nursing History Format SummaryDocument4 pagesAssessment Tool - Nursing History Format SummaryKeid Reuma100% (1)
- 20.lymphatic DisordersDocument16 pages20.lymphatic DisordersShrestha Anjiv100% (2)
- B. SC Nursing Syllabus INC PDFDocument183 pagesB. SC Nursing Syllabus INC PDFSathya Palanisamy76% (29)
- Equilibrium The Art of Mastering SelfDocument131 pagesEquilibrium The Art of Mastering SelfSarim Ibn Salahadhin100% (1)
- Assessment of Peripheral Vascular SystemDocument25 pagesAssessment of Peripheral Vascular Systemtabarek100% (3)
- Assessment of The Peripheral Vascular SystemDocument3 pagesAssessment of The Peripheral Vascular SystemTrisha Andrea DavaNo ratings yet
- Assessment of The Peripheral Vascular SystemDocument11 pagesAssessment of The Peripheral Vascular SystemGVHHNo ratings yet
- Medical Surgical Nursing OrthopedicDocument22 pagesMedical Surgical Nursing Orthopedicroger80% (5)
- Skeletal TractionDocument7 pagesSkeletal TractionAnnalyn Austria100% (2)
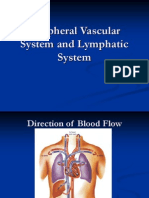
- Assessment of Peripheral Vascular System and Lymphatic SystemDocument37 pagesAssessment of Peripheral Vascular System and Lymphatic SystemSuzanne Rush100% (4)
- NCM103A W3 Range of Motion Module - 1774822568Document9 pagesNCM103A W3 Range of Motion Module - 1774822568Esvinch EsvinchNo ratings yet
- Procedure in Turning Client To Side-Lying PositionDocument1 pageProcedure in Turning Client To Side-Lying PositioncrrfrncNo ratings yet
- Coronary Circulation PhysiologyDocument25 pagesCoronary Circulation PhysiologyDerrick Ezra Ng100% (1)
- Blood Supply of HeartDocument20 pagesBlood Supply of HeartPraneethaNo ratings yet
- Performing Nutritional AssessmentDocument1 pagePerforming Nutritional AssessmentJoslyn GrossNo ratings yet
- AbdomenDocument7 pagesAbdomenShayne Lyrrie Pajela100% (1)
- Open Note TestDocument9 pagesOpen Note TestDean JezerNo ratings yet
- Ambulation Aids and Assistive DevicesDocument4 pagesAmbulation Aids and Assistive DevicesDiane Joy Mi-Hi BanaagNo ratings yet
- Common Surgical Instruments ModuleDocument5 pagesCommon Surgical Instruments ModuleAlokKumarNo ratings yet
- Anatomy & Physiology of The Cardiovascular SystemDocument3 pagesAnatomy & Physiology of The Cardiovascular SystemluaNo ratings yet
- 3&4&5-Assessment of Peripheral Vascular SystemDocument43 pages3&4&5-Assessment of Peripheral Vascular SystemKhaled Mohamed AssemNo ratings yet
- Breath Sounds: ConsiderationsDocument10 pagesBreath Sounds: ConsiderationsKarl RobleNo ratings yet
- Head To AssessmentDocument10 pagesHead To AssessmentUtayde Cassey FaithNo ratings yet
- Kinesiology of Movements: Understanding Planes and Axes of MovementDocument3 pagesKinesiology of Movements: Understanding Planes and Axes of MovementTessa Kaye - Rumol AlfaroNo ratings yet
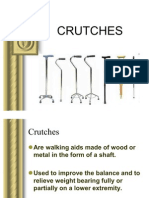
- CRUTCHESDocument35 pagesCRUTCHESBebing CostinianoNo ratings yet
- Perception and CoordinationDocument21 pagesPerception and Coordinationsimouny100% (28)
- Orthopedic NursingDocument46 pagesOrthopedic Nursingposh0038No ratings yet
- Fundamentals or Nursing ExamDocument13 pagesFundamentals or Nursing ExamJOki EstebanNo ratings yet
- Craniotomy Case ReportDocument19 pagesCraniotomy Case ReportElizar MercadoNo ratings yet
- NCM 120 Unit 1Document5 pagesNCM 120 Unit 1marlou agananNo ratings yet
- Assessing The Heart and Neck VesselsDocument6 pagesAssessing The Heart and Neck VesselsA R F I J U LNo ratings yet
- Geriatric Assistive DevicesDocument26 pagesGeriatric Assistive DevicesBrixter Greyson SencronoNo ratings yet
- Medical Surgical Nursing Orthopedic NursingDocument141 pagesMedical Surgical Nursing Orthopedic Nursingroger92% (12)
- Basic Nursing NotesDocument4 pagesBasic Nursing Notesbonggoi100% (1)
- Turning A Client To A Lateral or ProneDocument11 pagesTurning A Client To A Lateral or ProneTwinkle Salonga33% (3)
- Orthopedic HardwareDocument36 pagesOrthopedic HardwareMarivic Diano100% (1)
- Nursing Interview Guide - HA - VIOSDocument9 pagesNursing Interview Guide - HA - VIOSIra Velle ViosNo ratings yet
- FyhffDocument44 pagesFyhffRico Torregosa Jr.No ratings yet
- Spinal Cord Injury: Mrs. Zaida ZaracenaDocument36 pagesSpinal Cord Injury: Mrs. Zaida ZaracenaArdhel LoslosoNo ratings yet
- Assessing The Abdomen: Prepared By: Mary Ann F. Rubio, RN, MNDocument54 pagesAssessing The Abdomen: Prepared By: Mary Ann F. Rubio, RN, MNWilma Acorin OrillinedaNo ratings yet
- Bilateral Knee OADocument35 pagesBilateral Knee OAMu'iz Beatforteen50% (2)
- Discharge Care PlanDocument2 pagesDischarge Care PlanCecilio Singzon AguirreNo ratings yet
- Potts Report KoDocument6 pagesPotts Report Kobsn2011No ratings yet
- Questions 2Document20 pagesQuestions 2Ahwen 'ahwenism'No ratings yet
- The Thorax and Lungs Assessment (Autosaved)Document49 pagesThe Thorax and Lungs Assessment (Autosaved)Arlyn Mendenilla67% (3)
- Fall Prevention LectureDocument31 pagesFall Prevention Lecturedigracia manatigaNo ratings yet
- Transfer of A PatientDocument8 pagesTransfer of A Patienttrupti patelNo ratings yet
- Abdominal Aortic AneurysmDocument2 pagesAbdominal Aortic AneurysmSuhailah Mohd JamilNo ratings yet
- CastDocument2 pagesCastpoppysmic11No ratings yet
- Narrative ReportDocument1 pageNarrative ReportIrish Nicole DCNo ratings yet
- Comprehensive Edited)Document82 pagesComprehensive Edited)mikrobyo_ng_wmsuNo ratings yet
- Textbook of Medical Surgical NursingDocument1 pageTextbook of Medical Surgical NursingJenny Tran100% (1)
- Deep Veins of The LegsDocument11 pagesDeep Veins of The LegsnormalitaNo ratings yet
- Assessing The Peripheral Vascular System, Breast, AxillaeDocument52 pagesAssessing The Peripheral Vascular System, Breast, AxillaeAlyssa Mae RuizNo ratings yet
- Varicose VeinsDocument12 pagesVaricose Veinscheo sealyNo ratings yet
- Circulatory SystemDocument72 pagesCirculatory SystemJulia krizzea CristobalNo ratings yet
- Biology RevisionDocument11 pagesBiology RevisionifratsubhaNo ratings yet
- Topic 1 Revision NotesDocument6 pagesTopic 1 Revision NotesAldrin Tom100% (1)
- Practicum On Health Teaching (Draft)Document4 pagesPracticum On Health Teaching (Draft)Keid ReumaNo ratings yet
- Assessment of AbdomenDocument99 pagesAssessment of AbdomenKeid ReumaNo ratings yet
- Answers For Lab Exercise 4 Cell AnatomyDocument2 pagesAnswers For Lab Exercise 4 Cell AnatomyKeid ReumaNo ratings yet
- Lab Exercise 8 AnswersDocument3 pagesLab Exercise 8 AnswersKeid ReumaNo ratings yet
- PDF Class 11 Body Fluids Circulation BiologyDocument92 pagesPDF Class 11 Body Fluids Circulation BiologyNiharika SharmaNo ratings yet
- Lymphatic SystemDocument25 pagesLymphatic Systemumar khanNo ratings yet
- Gross Anatomy of Uterus: D R. Vibhash Kumar Vaidya Department of AnatomyDocument25 pagesGross Anatomy of Uterus: D R. Vibhash Kumar Vaidya Department of AnatomyAhsan TariqNo ratings yet
- The LIVERDocument5 pagesThe LIVERJennica Monique Tiu CequinaNo ratings yet
- Animal TransportDocument20 pagesAnimal TransportFeranmi AkinboboyeNo ratings yet
- The Radiation Protection KitDocument32 pagesThe Radiation Protection KitJayanth Bv100% (1)
- Lecture 4 - Mine DustDocument63 pagesLecture 4 - Mine DustBial100% (1)
- The LIVING MATRIX - American Academy of Osteopathy (PDFDrive)Document69 pagesThe LIVING MATRIX - American Academy of Osteopathy (PDFDrive)RukaphuongNo ratings yet
- Leaving Cert Religion Coursework 2017Document8 pagesLeaving Cert Religion Coursework 2017pqdgddifg100% (2)
- WL-ES700 Manual Preso en InglesDocument10 pagesWL-ES700 Manual Preso en InglesVerónica Barría JerezNo ratings yet
- Mastering Biology BK1B NotesDocument20 pagesMastering Biology BK1B NotesAlva WongNo ratings yet
- Lymphatic SystemDocument44 pagesLymphatic SystemAzizaNo ratings yet
- Negm Et Al 2024 MR Lymphangiography in Lymphatic Disorders Clinical Applications Institutional Experience and PracticeDocument19 pagesNegm Et Al 2024 MR Lymphangiography in Lymphatic Disorders Clinical Applications Institutional Experience and PracticeSahana RNo ratings yet
- MAAP Set 2Document86 pagesMAAP Set 2AaronMaroonFive100% (1)
- SinulDocument38 pagesSinulCucos NataliaNo ratings yet
- Healthmeans 3 Interview Transcripts From The Lymphatic Rescue SummitDocument34 pagesHealthmeans 3 Interview Transcripts From The Lymphatic Rescue SummitPatriciaPedroGomesNo ratings yet
- 22 Lymphatic System and ImmunityDocument42 pages22 Lymphatic System and Immunityrendra boyke2023No ratings yet
- Ana Phy LEC Activity - CHAPTER 14Document3 pagesAna Phy LEC Activity - CHAPTER 14dinson123No ratings yet
- Guide Questions Answers: 14.01A. Describe The Functions of The Lymphatic System. 14.01B. Explain How Lymph Is FormedDocument5 pagesGuide Questions Answers: 14.01A. Describe The Functions of The Lymphatic System. 14.01B. Explain How Lymph Is FormedPrancheska Abigayle Peneyra SantiagoNo ratings yet
- 13 OCTOBER, 2021 Wednesday Biology Transport SystemDocument12 pages13 OCTOBER, 2021 Wednesday Biology Transport SystemOyasor Ikhapo AnthonyNo ratings yet
- Summary Assessment HISTO LABDocument8 pagesSummary Assessment HISTO LABARAH DE OCAMPONo ratings yet
- Blood Vessels, AnatomyDocument20 pagesBlood Vessels, AnatomyAbu BakarNo ratings yet
- Lesson Plan - Immune SystemDocument37 pagesLesson Plan - Immune Systemsonyblank0% (1)
- Shivan Fascia Lymph 2023Document54 pagesShivan Fascia Lymph 2023Carol MontielNo ratings yet
- Urinary System Test BankDocument30 pagesUrinary System Test BankVinz TombocNo ratings yet