Download as pptx, pdf, or txt
You might also like
- Insulin Access ProgramDocument3 pagesInsulin Access ProgramErnest Jerome Malamion100% (1)
- Pediatrics in Review. Dehydration 2015Document14 pagesPediatrics in Review. Dehydration 2015Jorge Eduardo Espinoza Rios100% (2)
- Clinical Assessment and Diagnosis of Hypovolemia (Dehydration) in Children - UpToDateDocument12 pagesClinical Assessment and Diagnosis of Hypovolemia (Dehydration) in Children - UpToDateNedelcu MirunaNo ratings yet
- Concept Map of DMDocument2 pagesConcept Map of DMLeslie Marie Rendon100% (9)
- Dehydration Prevention and DiagnosisDocument7 pagesDehydration Prevention and DiagnosisdaliaNo ratings yet
- Journal of Geriatric Medicine and Gerontology JGMG 5 070Document7 pagesJournal of Geriatric Medicine and Gerontology JGMG 5 070Dilly NizaNo ratings yet
- DeshidratacionDocument14 pagesDeshidratacionAlvaro Andres Flores JimenezNo ratings yet
- Dehydration Isonatremic, Hyponatremic, andDocument15 pagesDehydration Isonatremic, Hyponatremic, andalfredoibcNo ratings yet
- Aged Care Brochure PDFDocument12 pagesAged Care Brochure PDFMuhammad ZubaidiNo ratings yet
- NCBI Bookshelf-Diabetes InsipidusDocument44 pagesNCBI Bookshelf-Diabetes InsipidusDiah Pradnya ParamitaNo ratings yet
- Hyponatremia and Hypernatremia in The ElderlyDocument15 pagesHyponatremia and Hypernatremia in The ElderlyStacey WoodsNo ratings yet
- Nutrition Noteworthy, 4 (1) Garcia, Marcela EsperanzaDocument7 pagesNutrition Noteworthy, 4 (1) Garcia, Marcela EsperanzadidikekoNo ratings yet
- Diagnosis of Polyuria and Diabetes Insipidus - UP To DATEDocument15 pagesDiagnosis of Polyuria and Diabetes Insipidus - UP To DATELuis Fernando Arias VillalobosNo ratings yet
- Ebp Summer 2014Document5 pagesEbp Summer 2014api-314483635No ratings yet
- Fluid Volume Deficit (Dehydration) Nursing Care Plan - NurseslabsDocument17 pagesFluid Volume Deficit (Dehydration) Nursing Care Plan - NurseslabsA.No ratings yet
- DehydrationDocument17 pagesDehydrationLaura Anghel-MocanuNo ratings yet
- Fluid Imbalance (NCP)Document9 pagesFluid Imbalance (NCP)Putry RainismNo ratings yet
- Case Report ..Document69 pagesCase Report ..sashadilanNo ratings yet
- Guidelines For Managing Acute Gastroenteritis Based On A Systematic Review of Published ResearchDocument7 pagesGuidelines For Managing Acute Gastroenteritis Based On A Systematic Review of Published ResearchnikopkunairNo ratings yet
- Fluids SummaryDocument3 pagesFluids Summarymicheal1960No ratings yet
- Acute Gastroenteritis: Roscheyl Berg Tutor Bsn3A ' 12/14/16Document11 pagesAcute Gastroenteritis: Roscheyl Berg Tutor Bsn3A ' 12/14/16Roscheen Berg TutorNo ratings yet
- Assessment of Hydration Status in A Large PopulationDocument12 pagesAssessment of Hydration Status in A Large PopulationAbdul Aziz WahyudinNo ratings yet
- Ajcn 119925Document11 pagesAjcn 119925Rahmanu ReztaputraNo ratings yet
- Case Study On DehydrationDocument4 pagesCase Study On DehydrationDustin Dela CruzNo ratings yet
- Diagnosis and Management of Dehydration in ChildrenDocument5 pagesDiagnosis and Management of Dehydration in ChildrenCitlalli MorenoNo ratings yet
- Diabetes InsipidusDocument18 pagesDiabetes InsipidusElena Patricia GonzálezNo ratings yet
- Deficient Fluid Volume Related To Fluid Loss To Subcutaneous TissueDocument2 pagesDeficient Fluid Volume Related To Fluid Loss To Subcutaneous TissueAillenne AlambraNo ratings yet
- DehydrationDocument27 pagesDehydrationDivika ShilvanaNo ratings yet
- 110-Dehydration and Disorders of Sodium BalanceDocument5 pages110-Dehydration and Disorders of Sodium BalancepelinNo ratings yet
- Acute GastroenteritisDocument11 pagesAcute GastroenteritisIneke PutriNo ratings yet
- Deshidratación y DisfaciaDocument13 pagesDeshidratación y DisfaciaALENo ratings yet
- Diabetes InsipidusDocument14 pagesDiabetes InsipidusTom BiusoNo ratings yet
- Medical Surgical Fluid and Electrolytes FVD FVEDocument7 pagesMedical Surgical Fluid and Electrolytes FVD FVEMichaelaKatrinaTrinidadNo ratings yet
- Anemia: Marcel E - ConradDocument6 pagesAnemia: Marcel E - ConradlacmftcNo ratings yet
- Assessment of Hypovolaemia in The Critically IllDocument10 pagesAssessment of Hypovolaemia in The Critically IllrjerezrNo ratings yet
- Perioperative Intravenous Fluid Therapy For Adults: Rob Mac Sweeney, Rachel Alexandra Mckendry, Amit BediDocument8 pagesPerioperative Intravenous Fluid Therapy For Adults: Rob Mac Sweeney, Rachel Alexandra Mckendry, Amit BediAnnisa Chaerani BurhanuddinNo ratings yet
- Sonia Nabila (P17220194050) Artikel B.InggrisDocument10 pagesSonia Nabila (P17220194050) Artikel B.InggrisSonia NabilaNo ratings yet
- Jonathan B. Edelson, MD Evan W. Orenstein, MD Lisa B. Zaoutis, MD Lawrence Copelovitch, MDDocument29 pagesJonathan B. Edelson, MD Evan W. Orenstein, MD Lisa B. Zaoutis, MD Lawrence Copelovitch, MDrifkiNo ratings yet
- There Are Two Main Types of GastritisDocument11 pagesThere Are Two Main Types of GastritisMike Faustino SolangonNo ratings yet
- Simulation Lab 20 Instructions With AnswersDocument5 pagesSimulation Lab 20 Instructions With AnswersChristine Mccombs100% (3)
- Art 38Document9 pagesArt 38Francesca BertaccaNo ratings yet
- Case Study 12Document7 pagesCase Study 12Steve MizzoNo ratings yet
- Dehydration in Children - Pediatrics - MSD Manual Professional EditionDocument5 pagesDehydration in Children - Pediatrics - MSD Manual Professional EditionA.No ratings yet
- Addison's DseDocument9 pagesAddison's DseKath RubioNo ratings yet
- Fluid Challenge Revisited. - 2006 - Vincent, Weil PDFDocument5 pagesFluid Challenge Revisited. - 2006 - Vincent, Weil PDFGiselle Baião100% (1)
- Diarrhea - StatPearls - NCBI BookshelfDocument4 pagesDiarrhea - StatPearls - NCBI BookshelfIndira SellyNo ratings yet
- Graziella Allana Serra Alves de Oliveira Olle 2018Document12 pagesGraziella Allana Serra Alves de Oliveira Olle 2018Anindya Laksmi LarasatiNo ratings yet
- Refeeding Syndrome A Literature Review KhanDocument7 pagesRefeeding Syndrome A Literature Review Khangw060qpy100% (1)
- Reading - Age With Moderate DehydrationDocument8 pagesReading - Age With Moderate DehydrationSophia IbuyanNo ratings yet
- Acute GastroenteritisDocument51 pagesAcute GastroenteritisuouoNo ratings yet
- DeshidratacionpedDocument6 pagesDeshidratacionpedKaren Alejandra RiveraNo ratings yet
- CASE STUDY of AGE With Moderate DehydrationDocument24 pagesCASE STUDY of AGE With Moderate DehydrationHikaru Takishima100% (2)
- Excess Fluid Volume - Nursing Diagnosis & Care Plan - NurseslabsDocument8 pagesExcess Fluid Volume - Nursing Diagnosis & Care Plan - NurseslabsEricsonMitraNo ratings yet
- Fluid Challenge RevisitedDocument5 pagesFluid Challenge RevisitedNinda DevitaNo ratings yet
- Evaluation and Treatment of HypernatremiaDocument9 pagesEvaluation and Treatment of HypernatremiaRESIDENTES MEDICINA INTERNANo ratings yet
- Ebr - F&e OxygenationDocument1 pageEbr - F&e OxygenationDARLENE ROSE BONGCAWILNo ratings yet
- Case Report - Diabetes InsipidusDocument4 pagesCase Report - Diabetes InsipidusSACHI DANIELLA TATOYNo ratings yet
- g2 9321 Alteration in Fluids ElectrolytesDocument88 pagesg2 9321 Alteration in Fluids ElectrolytesKRIZIELL KATE ALIGANNo ratings yet
- Diarrhoea in TravellersDocument5 pagesDiarrhoea in TravellersMazo KhanNo ratings yet
- Deshidratación en Ancianos Cuidado A Largo Plazo Con Disfagia Orofaríngea 2007Document6 pagesDeshidratación en Ancianos Cuidado A Largo Plazo Con Disfagia Orofaríngea 2007Natalia BeltranNo ratings yet
- IM Small Intestine HWDocument3 pagesIM Small Intestine HWArienne_Mae_A__6554No ratings yet
- Hepatorenal Syndrome: Causes, Tests, and Treatment OptionsFrom EverandHepatorenal Syndrome: Causes, Tests, and Treatment OptionsRating: 4.5 out of 5 stars4.5/5 (2)
- Diabetes Comprehensive T2DM Management: Hemi SinoritaDocument55 pagesDiabetes Comprehensive T2DM Management: Hemi SinoritaJipeeZedNo ratings yet
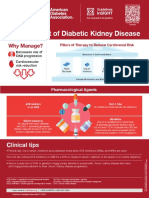
- Management of Diabetic Kidney Disease Updated 0Document1 pageManagement of Diabetic Kidney Disease Updated 0Jia-PeiWuNo ratings yet
- 13463-Article Text-25834-1-10-20210103Document3 pages13463-Article Text-25834-1-10-20210103Melly SyafridaNo ratings yet
- Understand Diabetes and Take Control - BanglaDocument23 pagesUnderstand Diabetes and Take Control - BanglaInternational Diabetes Federation100% (2)
- DiabenoDocument10 pagesDiabenoMeghna Porwal100% (1)
- Research ProposalDocument2 pagesResearch ProposalTANNER SMITHNo ratings yet
- Daftar Kunjungan Pasien Klinik Advanced Medical Center Februari 2023Document6,521 pagesDaftar Kunjungan Pasien Klinik Advanced Medical Center Februari 2023Ferdy AnsyahNo ratings yet
- Diabetic Gangrene 2Document3 pagesDiabetic Gangrene 2ShrutiNo ratings yet
- 47 Review Article - Sushmitha Ramona KarkadaDocument4 pages47 Review Article - Sushmitha Ramona KarkadaAnjali Rahul AjmeriNo ratings yet
- OET Peter DDocument2 pagesOET Peter DLorraine JohnsNo ratings yet
- Ispad 2022Document477 pagesIspad 2022hakimadnenNo ratings yet
- Nurs FPX 4030 Assessment 2 Determining The Credibility of Evidence and ResourcesDocument5 pagesNurs FPX 4030 Assessment 2 Determining The Credibility of Evidence and ResourcesEmma WatsonNo ratings yet
- Algorithm For Blood Glucose Lowering Therapy in Adults With Type 2 Diabetes PDF 2185604173Document1 pageAlgorithm For Blood Glucose Lowering Therapy in Adults With Type 2 Diabetes PDF 2185604173AlessioNavarraNo ratings yet
- DKA and HHS The Washington Manual of Critical CareDocument6 pagesDKA and HHS The Washington Manual of Critical Careمحمد عقيلي100% (1)
- DownloadDocument6 pagesDownloadNamasteNo ratings yet
- DAS Research Version 2.docx: Paper NameDocument43 pagesDAS Research Version 2.docx: Paper Namemiko balisiNo ratings yet
- Vanessa Fok - Project Overview Draft - 2970996Document2 pagesVanessa Fok - Project Overview Draft - 2970996api-552878628No ratings yet
- Javier1 ThemapDocument1 pageJavier1 Themapapi-253216868No ratings yet
- Ada-Montefiore Dka Protcol Version 3.0 5 22 20Document3 pagesAda-Montefiore Dka Protcol Version 3.0 5 22 20ibnuNo ratings yet
- Pengenalan DiabetesDocument57 pagesPengenalan DiabetesAsma MandaNo ratings yet
- Medical Emergencies Endocrine DisordersDocument97 pagesMedical Emergencies Endocrine DisordersKhadija VasiNo ratings yet
- ACC Handbook Ascvd Type 2 Diabetes: On andDocument10 pagesACC Handbook Ascvd Type 2 Diabetes: On andZH. omg sarNo ratings yet
- Activity - Intro To HA Lec 1Document2 pagesActivity - Intro To HA Lec 1Garth leigh CarbonellNo ratings yet
- Keto DietDocument100 pagesKeto Dietmillie1971No ratings yet
- Case Presentation - DM (Tantsa Tamia)Document58 pagesCase Presentation - DM (Tantsa Tamia)tantsaNo ratings yet
- Java Plum Stem Bark As Diabetes ControllerDocument11 pagesJava Plum Stem Bark As Diabetes ControllerSaimea Cliare Y. RodriguezNo ratings yet
- The Ketogenic Diet & Insulin ResistanceDocument2 pagesThe Ketogenic Diet & Insulin ResistanceSaurabh Pandey0% (1)
- GLUCOMETRO Glucocard 01-Mini PDFDocument76 pagesGLUCOMETRO Glucocard 01-Mini PDFclaudiaNo ratings yet