Download as pptx, pdf, or txt
You might also like
- Chapter 13: Schizophrenia and Other Psychotic Disorders: Multiple ChoiceDocument24 pagesChapter 13: Schizophrenia and Other Psychotic Disorders: Multiple ChoicesnowyznNo ratings yet
- Schizophrenia Case StudyDocument13 pagesSchizophrenia Case StudyAnonymous Hfrl594No ratings yet
- Myeloproliferative DisordersDocument33 pagesMyeloproliferative DisordersDhera Charles100% (1)
- Last Minute MRCP RevisionDocument737 pagesLast Minute MRCP RevisionSherif Elbadrawy100% (8)
- DR Nilukshi Perera Consultant HaematologistDocument68 pagesDR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- Personal StatementDocument2 pagesPersonal StatementSabha RabayaNo ratings yet
- Excerpt: "Fat Chance" by Robert LustigDocument3 pagesExcerpt: "Fat Chance" by Robert Lustigwamu885067% (3)
- Hema RecallDocument11 pagesHema Recallmkct111100% (1)
- CBT Dams Paper 1Document129 pagesCBT Dams Paper 1Gajeshwar Bahekar100% (1)
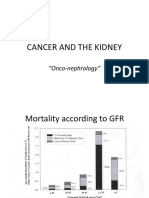
- Cancer and The KidneyDocument29 pagesCancer and The Kidney[ qιlα ]No ratings yet
- Hyperleukositosis: Bidasari Lubis-Olga Rasiyanti SiregarDocument26 pagesHyperleukositosis: Bidasari Lubis-Olga Rasiyanti SiregarYogiPrimaZulkifliNo ratings yet
- Polycythaemia Y3 R6Document18 pagesPolycythaemia Y3 R6azahirNo ratings yet
- Anemia Workshop1Document80 pagesAnemia Workshop1api-3762917No ratings yet
- Approach To Patients With Thrombocytosis and Polycythemia-En SonDocument52 pagesApproach To Patients With Thrombocytosis and Polycythemia-En SoncerenblgstrNo ratings yet
- Mielodisplasia, Neoplasia Maligna Hematopoyetica y Anemia AplasicaDocument24 pagesMielodisplasia, Neoplasia Maligna Hematopoyetica y Anemia AplasicakevinrdrixNo ratings yet
- Mielodisplasia, Neoplasia Maligna Hematopoyetica y Anemia AplasicaDocument24 pagesMielodisplasia, Neoplasia Maligna Hematopoyetica y Anemia AplasicakevinrdrixNo ratings yet
- Myelodysplasia (Definition/Incidence)Document10 pagesMyelodysplasia (Definition/Incidence)IlyasHasanNo ratings yet
- MDS and MPNDocument41 pagesMDS and MPNsamaNo ratings yet
- Handout 2 1522436248 PDFDocument82 pagesHandout 2 1522436248 PDFHarnadi WonogiriNo ratings yet
- Chronic Myeloproliferative DiseasesDocument84 pagesChronic Myeloproliferative DiseasesKayzee CruzNo ratings yet
- Polycythemia Vera ReportDocument31 pagesPolycythemia Vera ReportAdrianNo ratings yet
- Clinical Features Investigations: Aplastic Anaemia Primary Idiopathic Acquiredaplastic AnaemiaDocument5 pagesClinical Features Investigations: Aplastic Anaemia Primary Idiopathic Acquiredaplastic AnaemiaananNo ratings yet
- Haemolytic Anaemias 1Document40 pagesHaemolytic Anaemias 1HetaNo ratings yet
- Chronic Myeloproliferative DisorderDocument25 pagesChronic Myeloproliferative DisorderJilycamae COSMODNo ratings yet
- Anemia-Dr Moses KazevuDocument86 pagesAnemia-Dr Moses KazevuMoses Jr KazevuNo ratings yet
- Differences Between Diseases of Platelets/Vessel Wall or of Coagulation FactorsDocument10 pagesDifferences Between Diseases of Platelets/Vessel Wall or of Coagulation FactorsIlyasHasanNo ratings yet
- Leukamia and Transfusion MedicineDocument26 pagesLeukamia and Transfusion MedicineSamuel kuriaNo ratings yet
- #27 Myeloproliferative UpdateDocument31 pages#27 Myeloproliferative UpdateasclswisconsinNo ratings yet
- POLYCYTHEMIADocument45 pagesPOLYCYTHEMIAVISHAL DUBEYNo ratings yet
- Polycythemiaverarumana 160328080829Document24 pagesPolycythemiaverarumana 160328080829interna MANADONo ratings yet
- PolycythaemiaDocument7 pagesPolycythaemiaazahirNo ratings yet
- 8bone Marrow FailureDocument30 pages8bone Marrow FailureanonacadsNo ratings yet
- Aplastic Anaemia: DR Sandeep M R Physician Jayanagar General Hospial BangaloreDocument26 pagesAplastic Anaemia: DR Sandeep M R Physician Jayanagar General Hospial BangaloreSandeep m rNo ratings yet
- Tutori - Anemia MhsDocument38 pagesTutori - Anemia Mhszaky ariandyNo ratings yet
- Polycythemia Vera: BY Rumana Hameed 1703108200 21 Phamr D InternDocument24 pagesPolycythemia Vera: BY Rumana Hameed 1703108200 21 Phamr D Interninterna MANADONo ratings yet
- Approach To Hemolytic AnemiasDocument41 pagesApproach To Hemolytic AnemiasAmit KinareNo ratings yet
- Penyakit Pada Anak. KP 37Document55 pagesPenyakit Pada Anak. KP 37Risma RonauliNo ratings yet
- Lecture INST-100473 2023 08 05 10 30 19Document85 pagesLecture INST-100473 2023 08 05 10 30 19ashmangalNo ratings yet
- Aplastic Anemia Lecture 1aDocument39 pagesAplastic Anemia Lecture 1aniaaseta100% (2)
- Thalassemia Major: College of Health Sciences Nursing Division WHO Collaborating Center For Nursing DevelopmentDocument21 pagesThalassemia Major: College of Health Sciences Nursing Division WHO Collaborating Center For Nursing DevelopmentyasernetNo ratings yet
- PCV and Myeloproliferative IllnessDocument34 pagesPCV and Myeloproliferative Illnessswathi bsNo ratings yet
- How I Treat Polycythemia VeraDocument11 pagesHow I Treat Polycythemia Veraayu_cicuuNo ratings yet
- Polycythemia Rubra VeraDocument10 pagesPolycythemia Rubra VeraMardhiyyah MazlanNo ratings yet
- Akmal - Hematology Individual WorkDocument16 pagesAkmal - Hematology Individual WorkAkmal SharafNo ratings yet
- Myeloproliferative Disorders (Bhs Inggris)Document57 pagesMyeloproliferative Disorders (Bhs Inggris)Denny DedenNo ratings yet
- ThrombophiliaDocument46 pagesThrombophiliaNabelle MarieNo ratings yet
- Thalassaemia Hereditary Haem DisordersDocument12 pagesThalassaemia Hereditary Haem DisordersRawan HamzaNo ratings yet
- Polycythemia Vera: DR - Karthik.S Moderator:Dr - Sumedh ShettyDocument51 pagesPolycythemia Vera: DR - Karthik.S Moderator:Dr - Sumedh ShettyDr. Apoorva KottaryNo ratings yet
- Journal Reading Pathobiology - Evita Febriyanti - 156070122011009Document16 pagesJournal Reading Pathobiology - Evita Febriyanti - 156070122011009EvitaFebriyantiPNo ratings yet
- Hemoglobinopati: Dr. Charles Antoni S.,M.Kes, Sp.ADocument26 pagesHemoglobinopati: Dr. Charles Antoni S.,M.Kes, Sp.AKaren PatriciaNo ratings yet
- CaseDocument10 pagesCaseMohamed Al-zichrawyNo ratings yet
- Hema - Guide Notes PDFDocument21 pagesHema - Guide Notes PDFVanessa Ladra100% (1)
- Ha I by AbdifatahDocument109 pagesHa I by AbdifatahAbdifatah AhmedNo ratings yet
- Case Presentation: Giorgi Kochiashvili, Rupesh Mohanadas, Mohammed Bilal, AbivarmaDocument29 pagesCase Presentation: Giorgi Kochiashvili, Rupesh Mohanadas, Mohammed Bilal, AbivarmaRupesh MohandasNo ratings yet
- Haematopathology 3:: Leucocytosis/LeucopeniaDocument113 pagesHaematopathology 3:: Leucocytosis/LeucopeniaarwaNo ratings yet
- 9a. Red Cell DisordersDocument46 pages9a. Red Cell DisordersMuhammad DaviqNo ratings yet
- Article of Macrocytosis NewDocument9 pagesArticle of Macrocytosis NewMominah MayamNo ratings yet
- DR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDocument30 pagesDR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDabogski FranceNo ratings yet
- DR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDocument30 pagesDR Vishu P Bhasin DCP Resident, Santosh Medical CollegeDabogski FranceNo ratings yet
- Haematology Handbook: Division of Specialty MedicineDocument30 pagesHaematology Handbook: Division of Specialty MedicineAlina DumitracheNo ratings yet
- LO TambahanDocument5 pagesLO TambahanDapot SianiparNo ratings yet
- Leukemias 2Document56 pagesLeukemias 2Y. Beatrice AbigailNo ratings yet
- AA in ClassDocument20 pagesAA in ClassRonaldoNo ratings yet
- Lec 1 MedDocument54 pagesLec 1 Medm kuNo ratings yet
- Acute Myeloblastic Leukaemia: BY DR Halima Talba Consultant Haematologist Department of Haematology and BtsDocument44 pagesAcute Myeloblastic Leukaemia: BY DR Halima Talba Consultant Haematologist Department of Haematology and BtsMuhammad Modu BulamaNo ratings yet
- Polycythemia Vera: Kimberly Truong Wendy YangDocument22 pagesPolycythemia Vera: Kimberly Truong Wendy YangAdeena RayNo ratings yet
- Uts Reviewer Cover To CoverDocument19 pagesUts Reviewer Cover To Covermyungsoo100% (2)
- Examiners' Report Principal Examiner Feedback January 2020Document8 pagesExaminers' Report Principal Examiner Feedback January 2020Laura Welsh100% (1)
- Pant Cell CultureDocument6 pagesPant Cell CulturegichkimahikanNo ratings yet
- Classification of Veneer PreparationsDocument11 pagesClassification of Veneer PreparationsVinisha Vipin SharmaNo ratings yet
- What Is Canavan BrochureDocument4 pagesWhat Is Canavan BrochureYamihush MuthuKumarNo ratings yet
- BIO095 Chapter 2: Gene Technology Compiled By: Noor Akmal Abd WahabDocument4 pagesBIO095 Chapter 2: Gene Technology Compiled By: Noor Akmal Abd WahabnazirafitriNo ratings yet
- 9700 s13 QP 11Document16 pages9700 s13 QP 11Joyce GohNo ratings yet
- Neurological HistoryDocument9 pagesNeurological HistorysamiNo ratings yet
- Parkinson's Disease Pathogenesis and Clinical AspectsDocument194 pagesParkinson's Disease Pathogenesis and Clinical AspectsSachin Raut100% (1)
- Introduction To Drug Discovery and DevelopmentDocument25 pagesIntroduction To Drug Discovery and Developmentafnanosman2002No ratings yet
- Encyclopedia of Anti Doping 2000 2015 PDFDocument4,506 pagesEncyclopedia of Anti Doping 2000 2015 PDFLeandro NascimentoNo ratings yet
- 12th Cbse Biology Board Paper 2008 To 2012 SolvedDocument299 pages12th Cbse Biology Board Paper 2008 To 2012 Solvedvivekjoseph9578% (18)
- Anatomy & Physiology of CellDocument14 pagesAnatomy & Physiology of CellBrianna ValerioNo ratings yet
- Pediatric Nursing: Narayan Swami College of NursingDocument10 pagesPediatric Nursing: Narayan Swami College of NursingAnkit KotnalaNo ratings yet
- Early HumanDocument4 pagesEarly HumanPeem JatabutNo ratings yet
- VocabDocument3 pagesVocabssasasNo ratings yet
- Cell SpecializationDocument12 pagesCell Specializationapi-324822024No ratings yet
- Pemeriksaan Terkini Hepatitis Virus: Prof. Dr. Jusak Nugraha, DR, MS, SPPK (K) Lab Patologi Klinik FK UnairDocument53 pagesPemeriksaan Terkini Hepatitis Virus: Prof. Dr. Jusak Nugraha, DR, MS, SPPK (K) Lab Patologi Klinik FK UnairMuh YunusNo ratings yet
- Molecular Biology of The CellDocument129 pagesMolecular Biology of The CellAndres Sanchez EscobedoNo ratings yet
- On Vision An: Asian Eye Institute 9X27 FCDocument5 pagesOn Vision An: Asian Eye Institute 9X27 FCAudreyNo ratings yet
- Digestive System Disorders Research AssignmentDocument2 pagesDigestive System Disorders Research Assignmentapi-305436791No ratings yet
- Stop AIDS. Keep The Promise.: L'Automédicat-ion Au Liban NordDocument13 pagesStop AIDS. Keep The Promise.: L'Automédicat-ion Au Liban Nordhussein bitarNo ratings yet
- Seminar On Preventive ObstetricsDocument49 pagesSeminar On Preventive ObstetricsRini Robert100% (3)