
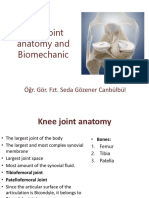
Knee Joint
Knee Joint
You might also like
- Shoulder Dislocation and Reduction - UpToDateDocument64 pagesShoulder Dislocation and Reduction - UpToDateCatedra 2018No ratings yet
- L - Lower Extremity (Bones and Joints)Document45 pagesL - Lower Extremity (Bones and Joints)Riyadh Ali nasser Al.Sharekh 0252No ratings yet
- 6 Diabetic FootDocument28 pages6 Diabetic FootPraneetha NouduriNo ratings yet
- General Principles of Geriatric RehabilitationDocument5 pagesGeneral Principles of Geriatric RehabilitationPraneetha Nouduri100% (2)
- Biomechanics of Knee JointDocument123 pagesBiomechanics of Knee JointSIBASIS PATTANAYAKNo ratings yet
- Anatomy of The Knee JointDocument26 pagesAnatomy of The Knee JointSaghar AbroNo ratings yet
- Knee Ankle JointsDocument38 pagesKnee Ankle JointsmaggieNo ratings yet
- Therapeutic Exercise: Foundation & Techniques: Resource Person: Dr. Rahat Ayub PT SHS.326.Lec.15Document31 pagesTherapeutic Exercise: Foundation & Techniques: Resource Person: Dr. Rahat Ayub PT SHS.326.Lec.15Fatima YasirNo ratings yet
- Anatomy of Knee Joint and Popliteal Fossa: Prof. Dr. Nabil Khouri MDDocument37 pagesAnatomy of Knee Joint and Popliteal Fossa: Prof. Dr. Nabil Khouri MDBadria Al-najiNo ratings yet
- Knee MechanicsDocument107 pagesKnee MechanicsAhmed El goharyNo ratings yet
- Anatomy of Hip and Knee Joint and Popliteal Fossa: Prof. Dr. Nabil KhourDocument49 pagesAnatomy of Hip and Knee Joint and Popliteal Fossa: Prof. Dr. Nabil KhourBadria Al-najiNo ratings yet
- Di̇z Eklemi̇ni̇n Anatomi̇si̇ Ve Bi̇yomekani̇ği̇ - Bau (1) - 2Document67 pagesDi̇z Eklemi̇ni̇n Anatomi̇si̇ Ve Bi̇yomekani̇ği̇ - Bau (1) - 2erfan mohammadiNo ratings yet
- Biomechanics of Knee COMPLEX: Dr. Sumit Raghav (PT)Document52 pagesBiomechanics of Knee COMPLEX: Dr. Sumit Raghav (PT)Kavya MittalNo ratings yet
- 2 - Knee JointDocument46 pages2 - Knee Jointnoor.komalNo ratings yet
- Hipjointppt 140903215412 Phpapp01Document23 pagesHipjointppt 140903215412 Phpapp01Ashraf SidrahNo ratings yet
- Knee JointDocument49 pagesKnee JointRiaz SialNo ratings yet
- Anatomy of Knee JointDocument17 pagesAnatomy of Knee JointSiti AisyahNo ratings yet
- Anatomy of Knee JointDocument91 pagesAnatomy of Knee Jointzmk KNo ratings yet
- Knee PresentationDocument56 pagesKnee PresentationKushie GuezyNo ratings yet
- Biomechanics of Knee - 1Document43 pagesBiomechanics of Knee - 1mahiNo ratings yet
- Lec 14 THE KNEE JOINTDocument17 pagesLec 14 THE KNEE JOINTMaheen IrfanNo ratings yet
- Lower LimbDocument24 pagesLower LimbKhadija AbouslimaNo ratings yet
- Sport Traumatology-III Knee Complex-7Document24 pagesSport Traumatology-III Knee Complex-7kamran aliNo ratings yet
- Knee 05102018Document24 pagesKnee 05102018Dk KNo ratings yet
- Hip JointDocument25 pagesHip JointHashim OmarNo ratings yet
- Lec - 2 - Knee, Ankle & FootDocument65 pagesLec - 2 - Knee, Ankle & Foot丘嘉豪No ratings yet
- Hip JointDocument25 pagesHip JointHashim OmarNo ratings yet
- Knee Joint and Popliteal FossaDocument71 pagesKnee Joint and Popliteal FossaEsdras DountioNo ratings yet
- Biomechanics & Joint Replacement of The Knee: PGI Balisi JI Cabalza JI Feliciano JI Fernandez A. JI Fernandez KDocument46 pagesBiomechanics & Joint Replacement of The Knee: PGI Balisi JI Cabalza JI Feliciano JI Fernandez A. JI Fernandez KGio BalisiNo ratings yet
- Joints of Lower Limb 2017Document77 pagesJoints of Lower Limb 2017yasrul izadNo ratings yet
- Hip JointDocument23 pagesHip Jointmariajaved0089No ratings yet
- Femerotibial JointDocument58 pagesFemerotibial JointGalaxyNo ratings yet
- Joints of Lower LimbDocument55 pagesJoints of Lower LimbHanis ZahirahNo ratings yet
- Joints of Lower LimbsDocument12 pagesJoints of Lower LimbsMohammed SheikhNo ratings yet
- XX Popliteal Fossa and Knee JointDocument43 pagesXX Popliteal Fossa and Knee JointAlistair WalkerNo ratings yet
- Anatomy of KneeDocument47 pagesAnatomy of Kneehanuman kannaNo ratings yet
- The Biomechanics of The Human Lower Extremity: BSPT, PP - DPT. M.PhilDocument59 pagesThe Biomechanics of The Human Lower Extremity: BSPT, PP - DPT. M.PhilKinzaNo ratings yet
- Dr. Nabil Khouri MD, MSC - PHDDocument63 pagesDr. Nabil Khouri MD, MSC - PHDmaniagfeNo ratings yet
- Biomechanics of KneeDocument48 pagesBiomechanics of KneeGavi Krishna100% (1)
- Back and Hip Pain (Materi Anatomy Dr. Maria)Document33 pagesBack and Hip Pain (Materi Anatomy Dr. Maria)mariaNo ratings yet
- Pectoral Girdle and Shoulder JointDocument55 pagesPectoral Girdle and Shoulder JointGaurav ThapaNo ratings yet
- The Knee Joint and Popliteal FossaDocument18 pagesThe Knee Joint and Popliteal Fossaolamidealapa2608No ratings yet
- Biomech of Hip JointDocument68 pagesBiomech of Hip JointkashifNo ratings yet
- CH 07Document33 pagesCH 07Khadim ShahNo ratings yet
- The Ligamentum Flavum:: Present Throughout Vertebral ColumnDocument9 pagesThe Ligamentum Flavum:: Present Throughout Vertebral ColumnUmar JawadNo ratings yet
- Biomechanics of KneeDocument78 pagesBiomechanics of KneeDr. Sabari ManokaranNo ratings yet
- Knee JointDocument28 pagesKnee JointRaj Shekhar Singh100% (1)
- Chapter 19Document10 pagesChapter 19poNo ratings yet
- Naik, S. - Biomechanics of Knee ComplexDocument25 pagesNaik, S. - Biomechanics of Knee ComplexKyle Bois100% (4)
- Hip Joint.Document32 pagesHip Joint.Rida fatimaNo ratings yet
- Joints of Limbs - 2015-RuanDocument61 pagesJoints of Limbs - 2015-RuanKw ChanNo ratings yet
- Biomechanics of Hip Joint - DevadriDocument22 pagesBiomechanics of Hip Joint - DevadriDevadri DeyNo ratings yet
- Hip Joint 2Document25 pagesHip Joint 2justin sundayNo ratings yet
- 2013 - Lower Limb-HIP JointDocument14 pages2013 - Lower Limb-HIP Jointmarina_shawkyNo ratings yet
- 1 Lower Limb BONESDocument79 pages1 Lower Limb BONESZaid AbdulqadirNo ratings yet
- Joints of The Lower LimbDocument54 pagesJoints of The Lower LimbCupid MohNo ratings yet
- 7 MS Anatomy and PhysiologyDocument5 pages7 MS Anatomy and PhysiologyJanah CalitNo ratings yet
- Knee Biomechanics: by Amrita..Document57 pagesKnee Biomechanics: by Amrita..Chanda NathaniNo ratings yet
- Shoulder JointDocument82 pagesShoulder JointRajesh SahaNo ratings yet
- Radioanatomy of Shoulder Joint-Dr - NaziyaDocument82 pagesRadioanatomy of Shoulder Joint-Dr - Naziyaraghavmaster100% (1)
- Anatomy of Hip JointDocument5 pagesAnatomy of Hip JointSneha ParveenNo ratings yet
- Healthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesFrom EverandHealthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesNo ratings yet
- Terms Referring To The LayersDocument23 pagesTerms Referring To The LayersPraneetha NouduriNo ratings yet
- Meherbaan SinghDocument24 pagesMeherbaan SinghPraneetha NouduriNo ratings yet
- Role of Hospital AdministratorDocument6 pagesRole of Hospital AdministratorPraneetha NouduriNo ratings yet
- The Meninges and Blood Vessels of Brain and Spinal Cord, and The Cerebrospinal FluidDocument39 pagesThe Meninges and Blood Vessels of Brain and Spinal Cord, and The Cerebrospinal FluidPraneetha NouduriNo ratings yet
- Spinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PuneDocument43 pagesSpinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PunePraneetha NouduriNo ratings yet
- TENS (Transcutaneous Electrical Nerve Stimulation)Document34 pagesTENS (Transcutaneous Electrical Nerve Stimulation)Praneetha NouduriNo ratings yet
- Interstitial Lung DiseaseDocument31 pagesInterstitial Lung DiseasePraneetha NouduriNo ratings yet
- Cardiac ExaminationDocument21 pagesCardiac ExaminationPraneetha NouduriNo ratings yet
- Anthropometrical Characteristics and Somatotype of Young Soccer Players and Their Comparison With The General PopulationDocument9 pagesAnthropometrical Characteristics and Somatotype of Young Soccer Players and Their Comparison With The General PopulationPraneetha NouduriNo ratings yet
- Pleura 1Document37 pagesPleura 1Praneetha NouduriNo ratings yet
- Neuro ProformaDocument20 pagesNeuro ProformaPraneetha NouduriNo ratings yet
- Sciatic Nerve - IipptDocument21 pagesSciatic Nerve - IipptPraneetha NouduriNo ratings yet
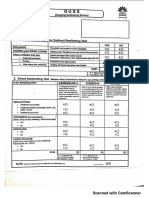
- Guss 20200107161739 PDFDocument2 pagesGuss 20200107161739 PDFPraneetha NouduriNo ratings yet
- FATOUROS2000Document7 pagesFATOUROS2000Praneetha NouduriNo ratings yet
- Chest X-RayDocument31 pagesChest X-RayPraneetha NouduriNo ratings yet
- Basics of Electrotherapy 2nd PDFDocument175 pagesBasics of Electrotherapy 2nd PDFPraneetha Nouduri100% (1)
- General SurgeriesDocument26 pagesGeneral SurgeriesPraneetha NouduriNo ratings yet
- Burn ManagementDocument15 pagesBurn ManagementPraneetha NouduriNo ratings yet
- Arterial Blood GasesDocument16 pagesArterial Blood GasesPraneetha NouduriNo ratings yet
- Proprioceptive Neuromuscular Facilitation: Vicky S. WardlawDocument44 pagesProprioceptive Neuromuscular Facilitation: Vicky S. WardlawPraneetha Nouduri100% (1)
- BASMI ScaleDocument1 pageBASMI ScalePraneetha NouduriNo ratings yet
- 0 - Knee Joint AssessmentDocument4 pages0 - Knee Joint AssessmentAndrei MariusNo ratings yet
- Case Report A Rare Acromioclavicular Joint Injury in A Twelve-Year-Old Boy. ADocument5 pagesCase Report A Rare Acromioclavicular Joint Injury in A Twelve-Year-Old Boy. AKirubakaran Saraswathy PattabiramanNo ratings yet
- Hip HepDocument3 pagesHip HepRicardo RosaNo ratings yet
- AmputationDocument52 pagesAmputationShobhit SharmaNo ratings yet
- Shoulder Pain 3Document8 pagesShoulder Pain 3sitialimahNo ratings yet
- 2021 4.2.3 Muscle ListDocument2 pages2021 4.2.3 Muscle ListAlyssa JacobsNo ratings yet
- Tabel Rehab Fraktur (Hoppenfeld) PDFDocument2 pagesTabel Rehab Fraktur (Hoppenfeld) PDFJerry Kurnia WahyudiNo ratings yet
- Tendon Transfers and Upper Limb Disorders: Aws KhanfarDocument41 pagesTendon Transfers and Upper Limb Disorders: Aws KhanfarRaghu Nadh100% (1)
- श्री महागणपति मन्त्र जपः॥ Śrī Mahāgaṇapati Mantra JapaḥDocument4 pagesश्री महागणपति मन्त्र जपः॥ Śrī Mahāgaṇapati Mantra JapaḥFull CreamNo ratings yet
- LSC Seo ReportDocument5 pagesLSC Seo Reportgicogap739100% (1)
- Posterior Malleolar Fractures: A Critical Analysis ReviewDocument17 pagesPosterior Malleolar Fractures: A Critical Analysis ReviewJohn Sebastian ValenciaNo ratings yet
- Phases of The PushupDocument2 pagesPhases of The PushupMaryane AngelaNo ratings yet
- Splinting Pocket Guide PDFDocument16 pagesSplinting Pocket Guide PDFMohd Khairil Anwar Ramli100% (1)
- GSC - DDH LCPD SCFE and OthersDocument3 pagesGSC - DDH LCPD SCFE and OthersJulia SalvioNo ratings yet
- O Hā Nyāsa : IAST and MalayalamDocument37 pagesO Hā Nyāsa : IAST and MalayalamPundarikakshasarma VedamNo ratings yet
- Ziran 2007Document6 pagesZiran 2007fhqybd88y4No ratings yet
- E1 Muscle AnatomyDocument30 pagesE1 Muscle AnatomyRay Sophia CuberoNo ratings yet
- Biomechanical Considerations For Rehabilitation of The KneeDocument38 pagesBiomechanical Considerations For Rehabilitation of The KneeStefan VladNo ratings yet
- Leg and Foot PDFDocument7 pagesLeg and Foot PDFStephen Subiera MiayoNo ratings yet
- Upper LimbDocument65 pagesUpper Limblotusmeekurns100% (1)
- GBG Weight WorkDocument12 pagesGBG Weight Workdretoure9No ratings yet
- Kerangka Fikir Chondromalacia PatellaDocument10 pagesKerangka Fikir Chondromalacia PatellaAfifah NurNo ratings yet
- Shoulder Rehabilitation Strategies, Guidelines, and PracticeDocument10 pagesShoulder Rehabilitation Strategies, Guidelines, and PracticeoscarNo ratings yet
- BestbodyeverDocument6 pagesBestbodyeverCeikaNo ratings yet
- Müller AO Classification of FracturesDocument4 pagesMüller AO Classification of FracturesAnkit KarkiNo ratings yet
- Lower Extremity Detailed Skill SheetDocument2 pagesLower Extremity Detailed Skill SheetMuhammed ElgasimNo ratings yet
- Surgical Approaches For Tibial Plateau Fractures: Utku Kandemir, MD Jeffrey Maclean, MS, MDDocument9 pagesSurgical Approaches For Tibial Plateau Fractures: Utku Kandemir, MD Jeffrey Maclean, MS, MDGustavoBecerraNo ratings yet
- Fugl-Meyer Assessment Lower Extremity (Fma-Le) Assessment of Sensorimotor FunctionDocument2 pagesFugl-Meyer Assessment Lower Extremity (Fma-Le) Assessment of Sensorimotor FunctionFlorin MarinescuNo ratings yet
- Starting PositionsDocument63 pagesStarting PositionsThopu UmamaheswariNo ratings yet














































































































Download as pptx, pdf, or txt
You might also like
- Shoulder Dislocation and Reduction - UpToDateDocument64 pagesShoulder Dislocation and Reduction - UpToDateCatedra 2018No ratings yet
- L - Lower Extremity (Bones and Joints)Document45 pagesL - Lower Extremity (Bones and Joints)Riyadh Ali nasser Al.Sharekh 0252No ratings yet
- 6 Diabetic FootDocument28 pages6 Diabetic FootPraneetha NouduriNo ratings yet
- General Principles of Geriatric RehabilitationDocument5 pagesGeneral Principles of Geriatric RehabilitationPraneetha Nouduri100% (2)
- Biomechanics of Knee JointDocument123 pagesBiomechanics of Knee JointSIBASIS PATTANAYAKNo ratings yet
- Anatomy of The Knee JointDocument26 pagesAnatomy of The Knee JointSaghar AbroNo ratings yet
- Knee Ankle JointsDocument38 pagesKnee Ankle JointsmaggieNo ratings yet
- Therapeutic Exercise: Foundation & Techniques: Resource Person: Dr. Rahat Ayub PT SHS.326.Lec.15Document31 pagesTherapeutic Exercise: Foundation & Techniques: Resource Person: Dr. Rahat Ayub PT SHS.326.Lec.15Fatima YasirNo ratings yet
- Anatomy of Knee Joint and Popliteal Fossa: Prof. Dr. Nabil Khouri MDDocument37 pagesAnatomy of Knee Joint and Popliteal Fossa: Prof. Dr. Nabil Khouri MDBadria Al-najiNo ratings yet
- Knee MechanicsDocument107 pagesKnee MechanicsAhmed El goharyNo ratings yet
- Anatomy of Hip and Knee Joint and Popliteal Fossa: Prof. Dr. Nabil KhourDocument49 pagesAnatomy of Hip and Knee Joint and Popliteal Fossa: Prof. Dr. Nabil KhourBadria Al-najiNo ratings yet
- Di̇z Eklemi̇ni̇n Anatomi̇si̇ Ve Bi̇yomekani̇ği̇ - Bau (1) - 2Document67 pagesDi̇z Eklemi̇ni̇n Anatomi̇si̇ Ve Bi̇yomekani̇ği̇ - Bau (1) - 2erfan mohammadiNo ratings yet
- Biomechanics of Knee COMPLEX: Dr. Sumit Raghav (PT)Document52 pagesBiomechanics of Knee COMPLEX: Dr. Sumit Raghav (PT)Kavya MittalNo ratings yet
- 2 - Knee JointDocument46 pages2 - Knee Jointnoor.komalNo ratings yet
- Hipjointppt 140903215412 Phpapp01Document23 pagesHipjointppt 140903215412 Phpapp01Ashraf SidrahNo ratings yet
- Knee JointDocument49 pagesKnee JointRiaz SialNo ratings yet
- Anatomy of Knee JointDocument17 pagesAnatomy of Knee JointSiti AisyahNo ratings yet
- Anatomy of Knee JointDocument91 pagesAnatomy of Knee Jointzmk KNo ratings yet
- Knee PresentationDocument56 pagesKnee PresentationKushie GuezyNo ratings yet
- Biomechanics of Knee - 1Document43 pagesBiomechanics of Knee - 1mahiNo ratings yet
- Lec 14 THE KNEE JOINTDocument17 pagesLec 14 THE KNEE JOINTMaheen IrfanNo ratings yet
- Lower LimbDocument24 pagesLower LimbKhadija AbouslimaNo ratings yet
- Sport Traumatology-III Knee Complex-7Document24 pagesSport Traumatology-III Knee Complex-7kamran aliNo ratings yet
- Knee 05102018Document24 pagesKnee 05102018Dk KNo ratings yet
- Hip JointDocument25 pagesHip JointHashim OmarNo ratings yet
- Lec - 2 - Knee, Ankle & FootDocument65 pagesLec - 2 - Knee, Ankle & Foot丘嘉豪No ratings yet
- Hip JointDocument25 pagesHip JointHashim OmarNo ratings yet
- Knee Joint and Popliteal FossaDocument71 pagesKnee Joint and Popliteal FossaEsdras DountioNo ratings yet
- Biomechanics & Joint Replacement of The Knee: PGI Balisi JI Cabalza JI Feliciano JI Fernandez A. JI Fernandez KDocument46 pagesBiomechanics & Joint Replacement of The Knee: PGI Balisi JI Cabalza JI Feliciano JI Fernandez A. JI Fernandez KGio BalisiNo ratings yet
- Joints of Lower Limb 2017Document77 pagesJoints of Lower Limb 2017yasrul izadNo ratings yet
- Hip JointDocument23 pagesHip Jointmariajaved0089No ratings yet
- Femerotibial JointDocument58 pagesFemerotibial JointGalaxyNo ratings yet
- Joints of Lower LimbDocument55 pagesJoints of Lower LimbHanis ZahirahNo ratings yet
- Joints of Lower LimbsDocument12 pagesJoints of Lower LimbsMohammed SheikhNo ratings yet
- XX Popliteal Fossa and Knee JointDocument43 pagesXX Popliteal Fossa and Knee JointAlistair WalkerNo ratings yet
- Anatomy of KneeDocument47 pagesAnatomy of Kneehanuman kannaNo ratings yet
- The Biomechanics of The Human Lower Extremity: BSPT, PP - DPT. M.PhilDocument59 pagesThe Biomechanics of The Human Lower Extremity: BSPT, PP - DPT. M.PhilKinzaNo ratings yet
- Dr. Nabil Khouri MD, MSC - PHDDocument63 pagesDr. Nabil Khouri MD, MSC - PHDmaniagfeNo ratings yet
- Biomechanics of KneeDocument48 pagesBiomechanics of KneeGavi Krishna100% (1)
- Back and Hip Pain (Materi Anatomy Dr. Maria)Document33 pagesBack and Hip Pain (Materi Anatomy Dr. Maria)mariaNo ratings yet
- Pectoral Girdle and Shoulder JointDocument55 pagesPectoral Girdle and Shoulder JointGaurav ThapaNo ratings yet
- The Knee Joint and Popliteal FossaDocument18 pagesThe Knee Joint and Popliteal Fossaolamidealapa2608No ratings yet
- Biomech of Hip JointDocument68 pagesBiomech of Hip JointkashifNo ratings yet
- CH 07Document33 pagesCH 07Khadim ShahNo ratings yet
- The Ligamentum Flavum:: Present Throughout Vertebral ColumnDocument9 pagesThe Ligamentum Flavum:: Present Throughout Vertebral ColumnUmar JawadNo ratings yet
- Biomechanics of KneeDocument78 pagesBiomechanics of KneeDr. Sabari ManokaranNo ratings yet
- Knee JointDocument28 pagesKnee JointRaj Shekhar Singh100% (1)
- Chapter 19Document10 pagesChapter 19poNo ratings yet
- Naik, S. - Biomechanics of Knee ComplexDocument25 pagesNaik, S. - Biomechanics of Knee ComplexKyle Bois100% (4)
- Hip Joint.Document32 pagesHip Joint.Rida fatimaNo ratings yet
- Joints of Limbs - 2015-RuanDocument61 pagesJoints of Limbs - 2015-RuanKw ChanNo ratings yet
- Biomechanics of Hip Joint - DevadriDocument22 pagesBiomechanics of Hip Joint - DevadriDevadri DeyNo ratings yet
- Hip Joint 2Document25 pagesHip Joint 2justin sundayNo ratings yet
- 2013 - Lower Limb-HIP JointDocument14 pages2013 - Lower Limb-HIP Jointmarina_shawkyNo ratings yet
- 1 Lower Limb BONESDocument79 pages1 Lower Limb BONESZaid AbdulqadirNo ratings yet
- Joints of The Lower LimbDocument54 pagesJoints of The Lower LimbCupid MohNo ratings yet
- 7 MS Anatomy and PhysiologyDocument5 pages7 MS Anatomy and PhysiologyJanah CalitNo ratings yet
- Knee Biomechanics: by Amrita..Document57 pagesKnee Biomechanics: by Amrita..Chanda NathaniNo ratings yet
- Shoulder JointDocument82 pagesShoulder JointRajesh SahaNo ratings yet
- Radioanatomy of Shoulder Joint-Dr - NaziyaDocument82 pagesRadioanatomy of Shoulder Joint-Dr - Naziyaraghavmaster100% (1)
- Anatomy of Hip JointDocument5 pagesAnatomy of Hip JointSneha ParveenNo ratings yet
- Healthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesFrom EverandHealthy Hips Handbook: Exercises for Treating and Preventing Common Hip Joint InjuriesNo ratings yet
- Terms Referring To The LayersDocument23 pagesTerms Referring To The LayersPraneetha NouduriNo ratings yet
- Meherbaan SinghDocument24 pagesMeherbaan SinghPraneetha NouduriNo ratings yet
- Role of Hospital AdministratorDocument6 pagesRole of Hospital AdministratorPraneetha NouduriNo ratings yet
- The Meninges and Blood Vessels of Brain and Spinal Cord, and The Cerebrospinal FluidDocument39 pagesThe Meninges and Blood Vessels of Brain and Spinal Cord, and The Cerebrospinal FluidPraneetha NouduriNo ratings yet
- Spinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PuneDocument43 pagesSpinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PunePraneetha NouduriNo ratings yet
- TENS (Transcutaneous Electrical Nerve Stimulation)Document34 pagesTENS (Transcutaneous Electrical Nerve Stimulation)Praneetha NouduriNo ratings yet
- Interstitial Lung DiseaseDocument31 pagesInterstitial Lung DiseasePraneetha NouduriNo ratings yet
- Cardiac ExaminationDocument21 pagesCardiac ExaminationPraneetha NouduriNo ratings yet
- Anthropometrical Characteristics and Somatotype of Young Soccer Players and Their Comparison With The General PopulationDocument9 pagesAnthropometrical Characteristics and Somatotype of Young Soccer Players and Their Comparison With The General PopulationPraneetha NouduriNo ratings yet
- Pleura 1Document37 pagesPleura 1Praneetha NouduriNo ratings yet
- Neuro ProformaDocument20 pagesNeuro ProformaPraneetha NouduriNo ratings yet
- Sciatic Nerve - IipptDocument21 pagesSciatic Nerve - IipptPraneetha NouduriNo ratings yet
- Guss 20200107161739 PDFDocument2 pagesGuss 20200107161739 PDFPraneetha NouduriNo ratings yet
- FATOUROS2000Document7 pagesFATOUROS2000Praneetha NouduriNo ratings yet
- Chest X-RayDocument31 pagesChest X-RayPraneetha NouduriNo ratings yet
- Basics of Electrotherapy 2nd PDFDocument175 pagesBasics of Electrotherapy 2nd PDFPraneetha Nouduri100% (1)
- General SurgeriesDocument26 pagesGeneral SurgeriesPraneetha NouduriNo ratings yet
- Burn ManagementDocument15 pagesBurn ManagementPraneetha NouduriNo ratings yet
- Arterial Blood GasesDocument16 pagesArterial Blood GasesPraneetha NouduriNo ratings yet
- Proprioceptive Neuromuscular Facilitation: Vicky S. WardlawDocument44 pagesProprioceptive Neuromuscular Facilitation: Vicky S. WardlawPraneetha Nouduri100% (1)
- BASMI ScaleDocument1 pageBASMI ScalePraneetha NouduriNo ratings yet
- 0 - Knee Joint AssessmentDocument4 pages0 - Knee Joint AssessmentAndrei MariusNo ratings yet
- Case Report A Rare Acromioclavicular Joint Injury in A Twelve-Year-Old Boy. ADocument5 pagesCase Report A Rare Acromioclavicular Joint Injury in A Twelve-Year-Old Boy. AKirubakaran Saraswathy PattabiramanNo ratings yet
- Hip HepDocument3 pagesHip HepRicardo RosaNo ratings yet
- AmputationDocument52 pagesAmputationShobhit SharmaNo ratings yet
- Shoulder Pain 3Document8 pagesShoulder Pain 3sitialimahNo ratings yet
- 2021 4.2.3 Muscle ListDocument2 pages2021 4.2.3 Muscle ListAlyssa JacobsNo ratings yet
- Tabel Rehab Fraktur (Hoppenfeld) PDFDocument2 pagesTabel Rehab Fraktur (Hoppenfeld) PDFJerry Kurnia WahyudiNo ratings yet
- Tendon Transfers and Upper Limb Disorders: Aws KhanfarDocument41 pagesTendon Transfers and Upper Limb Disorders: Aws KhanfarRaghu Nadh100% (1)
- श्री महागणपति मन्त्र जपः॥ Śrī Mahāgaṇapati Mantra JapaḥDocument4 pagesश्री महागणपति मन्त्र जपः॥ Śrī Mahāgaṇapati Mantra JapaḥFull CreamNo ratings yet
- LSC Seo ReportDocument5 pagesLSC Seo Reportgicogap739100% (1)
- Posterior Malleolar Fractures: A Critical Analysis ReviewDocument17 pagesPosterior Malleolar Fractures: A Critical Analysis ReviewJohn Sebastian ValenciaNo ratings yet
- Phases of The PushupDocument2 pagesPhases of The PushupMaryane AngelaNo ratings yet
- Splinting Pocket Guide PDFDocument16 pagesSplinting Pocket Guide PDFMohd Khairil Anwar Ramli100% (1)
- GSC - DDH LCPD SCFE and OthersDocument3 pagesGSC - DDH LCPD SCFE and OthersJulia SalvioNo ratings yet
- O Hā Nyāsa : IAST and MalayalamDocument37 pagesO Hā Nyāsa : IAST and MalayalamPundarikakshasarma VedamNo ratings yet
- Ziran 2007Document6 pagesZiran 2007fhqybd88y4No ratings yet
- E1 Muscle AnatomyDocument30 pagesE1 Muscle AnatomyRay Sophia CuberoNo ratings yet
- Biomechanical Considerations For Rehabilitation of The KneeDocument38 pagesBiomechanical Considerations For Rehabilitation of The KneeStefan VladNo ratings yet
- Leg and Foot PDFDocument7 pagesLeg and Foot PDFStephen Subiera MiayoNo ratings yet
- Upper LimbDocument65 pagesUpper Limblotusmeekurns100% (1)
- GBG Weight WorkDocument12 pagesGBG Weight Workdretoure9No ratings yet
- Kerangka Fikir Chondromalacia PatellaDocument10 pagesKerangka Fikir Chondromalacia PatellaAfifah NurNo ratings yet
- Shoulder Rehabilitation Strategies, Guidelines, and PracticeDocument10 pagesShoulder Rehabilitation Strategies, Guidelines, and PracticeoscarNo ratings yet
- BestbodyeverDocument6 pagesBestbodyeverCeikaNo ratings yet
- Müller AO Classification of FracturesDocument4 pagesMüller AO Classification of FracturesAnkit KarkiNo ratings yet
- Lower Extremity Detailed Skill SheetDocument2 pagesLower Extremity Detailed Skill SheetMuhammed ElgasimNo ratings yet
- Surgical Approaches For Tibial Plateau Fractures: Utku Kandemir, MD Jeffrey Maclean, MS, MDDocument9 pagesSurgical Approaches For Tibial Plateau Fractures: Utku Kandemir, MD Jeffrey Maclean, MS, MDGustavoBecerraNo ratings yet
- Fugl-Meyer Assessment Lower Extremity (Fma-Le) Assessment of Sensorimotor FunctionDocument2 pagesFugl-Meyer Assessment Lower Extremity (Fma-Le) Assessment of Sensorimotor FunctionFlorin MarinescuNo ratings yet
- Starting PositionsDocument63 pagesStarting PositionsThopu UmamaheswariNo ratings yet