Download as ppt, pdf, or txt
You might also like
- 6 Diabetic FootDocument28 pages6 Diabetic FootPraneetha NouduriNo ratings yet
- General Principles of Geriatric RehabilitationDocument5 pagesGeneral Principles of Geriatric RehabilitationPraneetha Nouduri100% (2)
- OXYGENATIONDocument8 pagesOXYGENATIONJo Marchianne Pigar0% (1)
- 0fcfcc PDFDocument288 pages0fcfcc PDFDick Jonhnson100% (2)
- Pleura: Pleura Is A Serous Membrane Covering of The LungsDocument10 pagesPleura: Pleura Is A Serous Membrane Covering of The LungsSyeda SapnaNo ratings yet
- PLEURAEDocument9 pagesPLEURAEvaibhavdeshmukh0724No ratings yet
- Overview of Visceral Thorax - PleuraDocument33 pagesOverview of Visceral Thorax - PleuraHrishikesh BirjeNo ratings yet
- Anatomy Ii: by Dr. Ziyad M. Al Zeer Orthopedic Surgeon Assistant Professor MD - PHDDocument64 pagesAnatomy Ii: by Dr. Ziyad M. Al Zeer Orthopedic Surgeon Assistant Professor MD - PHDMOHAMMAD ALSWEITYNo ratings yet
- THORAX Part 2Document59 pagesTHORAX Part 2idrimuha333No ratings yet
- Pluera and LungsDocument105 pagesPluera and LungsueumanaNo ratings yet
- 20-Trachea, Bronchi & BPSDocument37 pages20-Trachea, Bronchi & BPSpm7197362No ratings yet
- Pneumothorax (Collapsed Lung)Document34 pagesPneumothorax (Collapsed Lung)james garcia100% (3)
- Pleura & LungsDocument26 pagesPleura & Lungswashma SoomroNo ratings yet
- Anatomy PleuraDocument7 pagesAnatomy PleuraLuminita A-LumyNo ratings yet
- The Pleurae and Pleural CavitiesDocument3 pagesThe Pleurae and Pleural Cavitiesoseko anthonyNo ratings yet
- Lower Resp TractDocument32 pagesLower Resp TractTakshikaNo ratings yet
- Anatomy of Pluera, Lungs and The Tracheobroncial TreeDocument108 pagesAnatomy of Pluera, Lungs and The Tracheobroncial TreeTahleel AltafNo ratings yet
- Pleural EffusionDocument53 pagesPleural EffusionZhyraine Iraj D. CaluzaNo ratings yet
- Thorax LungsDocument128 pagesThorax LungsVernon MasakayanNo ratings yet
- Hemothorax HandoutsDocument2 pagesHemothorax HandoutsJunathan L. DelgadoNo ratings yet
- Seminar On: Pulmonary TuberculosisDocument33 pagesSeminar On: Pulmonary TuberculosisPriyaranjan Jose88% (8)
- Embryology, Gross Anatomy and Histology of Lungs and Pleura: For PC-II Medicine Students By: Zelalem ADocument58 pagesEmbryology, Gross Anatomy and Histology of Lungs and Pleura: For PC-II Medicine Students By: Zelalem AAmanuel MaruNo ratings yet
- Pleural CavityDocument8 pagesPleural CavityKina KinaNo ratings yet
- Structure of The Pleurae: Parietal PleuraDocument7 pagesStructure of The Pleurae: Parietal PleuraGeorge WinchesterNo ratings yet
- Pleural Anatomy 1st Year Clinical by DR MuzaffarDocument22 pagesPleural Anatomy 1st Year Clinical by DR MuzaffarKashar SaeedNo ratings yet
- The Respiratory System: Anatomy and Physiology ReviewDocument3 pagesThe Respiratory System: Anatomy and Physiology ReviewTerry Mae Atilazal SarciaNo ratings yet
- Bronchial AsthmaDocument21 pagesBronchial AsthmaMoonNo ratings yet
- General Anatomy 4 Thoracic Cavity: Dr. Wesam BaderDocument46 pagesGeneral Anatomy 4 Thoracic Cavity: Dr. Wesam BaderAhmadNo ratings yet
- Respiratory: Welcome!Document119 pagesRespiratory: Welcome!Majo ParagasNo ratings yet
- Anatomy Lec 13 (Lungs)Document28 pagesAnatomy Lec 13 (Lungs)afzal sulemaniNo ratings yet
- Respiratory SystemDocument42 pagesRespiratory SystemSohailriazNo ratings yet
- Respiratory SystemDocument56 pagesRespiratory SystemSalma NawazNo ratings yet
- Anat Case 2Document8 pagesAnat Case 2AnanaaNo ratings yet
- Lungs and PleuraDocument7 pagesLungs and PleuraArvin ArliandoNo ratings yet
- HemothoraxDocument3 pagesHemothoraxkrz05No ratings yet
- Respiratory Notes (Chris Andersen, ICUPrimaryPrep - Com)Document14 pagesRespiratory Notes (Chris Andersen, ICUPrimaryPrep - Com)PkernNo ratings yet
- The Thorax Part Ii - The Thoracic Cavity: Juan Guido G. Joyo, PTRP Juvi G. Alicabo, PTRP, CCP, CTMBP, CTTTPDocument98 pagesThe Thorax Part Ii - The Thoracic Cavity: Juan Guido G. Joyo, PTRP Juvi G. Alicabo, PTRP, CCP, CTMBP, CTTTPFerjie Angelica DalandaoNo ratings yet
- Thoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دDocument18 pagesThoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دMuhammad UsmanNo ratings yet
- Case Study: Pleural Effusion: Union Christian CollegeDocument8 pagesCase Study: Pleural Effusion: Union Christian CollegeJobelle AcenaNo ratings yet
- LUNGSDocument14 pagesLUNGSNaman MishraNo ratings yet
- Pleura Space Anatomy: Review ArticleDocument6 pagesPleura Space Anatomy: Review ArticleRohitNo ratings yet
- Anatomy and Physiology of The Respiratory SystemDocument5 pagesAnatomy and Physiology of The Respiratory SystemLek Bassig ReyesNo ratings yet
- RespiratoryDocument249 pagesRespiratoryBulborea MihaelaNo ratings yet
- Respiratory LectureDocument17 pagesRespiratory Lecturemichellechapman0804No ratings yet
- Null 4Document47 pagesNull 4Kenyan MillanNo ratings yet
- BY Ifenna Nnachi Salvator REG NO: 2019070000636Document35 pagesBY Ifenna Nnachi Salvator REG NO: 2019070000636nnachi ifennaNo ratings yet
- Respiratory System Bullet PointsDocument5 pagesRespiratory System Bullet PointsArun KumarNo ratings yet
- Trachea, Bronchial Tree and Bronchopulmonary Segments: by Nitisha GuptaDocument15 pagesTrachea, Bronchial Tree and Bronchopulmonary Segments: by Nitisha GuptaNITISHA GUPTANo ratings yet
- LUNG-OVERVIEW (Autosaved)Document132 pagesLUNG-OVERVIEW (Autosaved)Thivashinie Kandy Nazan VelloNo ratings yet
- Anatomy Notes 4Document2 pagesAnatomy Notes 4Nia IarajuliNo ratings yet
- Anatomy of The Respiratory SystemDocument8 pagesAnatomy of The Respiratory Systemsuharti2365No ratings yet
- 1-The Respiratory SystemDocument7 pages1-The Respiratory SystemEma FröhlichováNo ratings yet
- Azygous VeinDocument12 pagesAzygous VeinLorenz SmallNo ratings yet
- A19. Anatomy of The PleuraDocument15 pagesA19. Anatomy of The PleuraUmerNo ratings yet
- Bronco Pulmonary SegmentDocument24 pagesBronco Pulmonary SegmentAnkit PancholiNo ratings yet
- Anatomy and PhysiologyDocument4 pagesAnatomy and Physiologyshanelle Lynn PalenNo ratings yet
- Respiratory SystemDocument38 pagesRespiratory SystemdjokerNo ratings yet
- Pleura: (1) Parietal Pleura (Parietal Layer)Document10 pagesPleura: (1) Parietal Pleura (Parietal Layer)Shimmering MoonNo ratings yet
- Thorax Lecture - 3Document46 pagesThorax Lecture - 3Amanuel mekonnenNo ratings yet
- PAin and Oxygenation HandoutsPRELIMSDocument7 pagesPAin and Oxygenation HandoutsPRELIMSJhoanna de ChavezNo ratings yet
- PleuraDocument6 pagesPleurasjs6r8wwv9No ratings yet
- PleuraDocument6 pagesPleuratejaschinchkarNo ratings yet
- Acute Respiratory Distres SyndromeDocument17 pagesAcute Respiratory Distres SyndromeLalrinchhani PautuNo ratings yet
- Pleurisy, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleurisy, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Meherbaan SinghDocument24 pagesMeherbaan SinghPraneetha NouduriNo ratings yet
- Role of Hospital AdministratorDocument6 pagesRole of Hospital AdministratorPraneetha NouduriNo ratings yet
- Terms Referring To The LayersDocument23 pagesTerms Referring To The LayersPraneetha NouduriNo ratings yet
- The Meninges and Blood Vessels of Brain and Spinal Cord, and The Cerebrospinal FluidDocument39 pagesThe Meninges and Blood Vessels of Brain and Spinal Cord, and The Cerebrospinal FluidPraneetha NouduriNo ratings yet
- Spinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PuneDocument43 pagesSpinal Cord: DR Ganesh Khemnar Assistant Professor Dept. of Anatomy BVDUMC, PunePraneetha NouduriNo ratings yet
- Interstitial Lung DiseaseDocument31 pagesInterstitial Lung DiseasePraneetha NouduriNo ratings yet
- Sciatic Nerve - IipptDocument21 pagesSciatic Nerve - IipptPraneetha NouduriNo ratings yet
- TENS (Transcutaneous Electrical Nerve Stimulation)Document34 pagesTENS (Transcutaneous Electrical Nerve Stimulation)Praneetha NouduriNo ratings yet
- Anthropometrical Characteristics and Somatotype of Young Soccer Players and Their Comparison With The General PopulationDocument9 pagesAnthropometrical Characteristics and Somatotype of Young Soccer Players and Their Comparison With The General PopulationPraneetha NouduriNo ratings yet
- Neuro ProformaDocument20 pagesNeuro ProformaPraneetha NouduriNo ratings yet
- FATOUROS2000Document7 pagesFATOUROS2000Praneetha NouduriNo ratings yet
- Chest X-RayDocument31 pagesChest X-RayPraneetha NouduriNo ratings yet
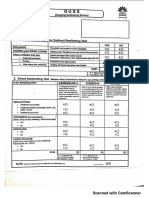
- Guss 20200107161739 PDFDocument2 pagesGuss 20200107161739 PDFPraneetha NouduriNo ratings yet
- General SurgeriesDocument26 pagesGeneral SurgeriesPraneetha NouduriNo ratings yet
- Cardiac ExaminationDocument21 pagesCardiac ExaminationPraneetha NouduriNo ratings yet
- Burn ManagementDocument15 pagesBurn ManagementPraneetha NouduriNo ratings yet
- Proprioceptive Neuromuscular Facilitation: Vicky S. WardlawDocument44 pagesProprioceptive Neuromuscular Facilitation: Vicky S. WardlawPraneetha Nouduri100% (1)
- Arterial Blood GasesDocument16 pagesArterial Blood GasesPraneetha NouduriNo ratings yet
- Basics of Electrotherapy 2nd PDFDocument175 pagesBasics of Electrotherapy 2nd PDFPraneetha Nouduri100% (1)
- BASMI ScaleDocument1 pageBASMI ScalePraneetha NouduriNo ratings yet
- Indication For BronchosDocument2 pagesIndication For BronchosdarsunaddictedNo ratings yet
- Airway ManagementDocument83 pagesAirway ManagementBerliany L Ganie FhatwaNo ratings yet
- Brochure MEDBRYT Ultrasonic Inhaler TajFUN 1 MU 1Document2 pagesBrochure MEDBRYT Ultrasonic Inhaler TajFUN 1 MU 1StevanusNo ratings yet
- # Davidson - Review # Respiratory - MedicineDocument18 pages# Davidson - Review # Respiratory - Medicineemtiaz zamanNo ratings yet
- Detailed Note On Speech Organ and Their Function. THR112Document18 pagesDetailed Note On Speech Organ and Their Function. THR112Samson BlessedNo ratings yet
- PCCPDocument1 pagePCCPOliver TabagNo ratings yet
- Zoology Finals ReviewerDocument18 pagesZoology Finals ReviewerZian Lei MienNo ratings yet
- End Blok Respi SoalDocument6 pagesEnd Blok Respi Soalanz_4191No ratings yet
- SpirometerDocument4 pagesSpirometerRicardo EstradaNo ratings yet
- Equine Infectious Diseases, 2nd Edition (VetBooks - Ir)Document930 pagesEquine Infectious Diseases, 2nd Edition (VetBooks - Ir)Dana UrueñaNo ratings yet
- Severe Asthma-Pathogenesis and Clinical ManagementDocument706 pagesSevere Asthma-Pathogenesis and Clinical ManagementNatia Demetradze0% (1)
- GUJCET2016T01 SolutionDocument12 pagesGUJCET2016T01 SolutionvuppalasampathNo ratings yet
- Mastering The Art of ArdsDocument69 pagesMastering The Art of ArdsRsc LmdNo ratings yet
- 1-First Aid Training Khmer & English (Basic)Document40 pages1-First Aid Training Khmer & English (Basic)Sor SethNo ratings yet
- TESIS Fernández MartínezDocument168 pagesTESIS Fernández MartínezKriistian Rene QuintanaNo ratings yet
- Breathing and Exchange of Gases: Class 11 Biology Ch. 17Document16 pagesBreathing and Exchange of Gases: Class 11 Biology Ch. 17Angelin JacobNo ratings yet
- Gaseous ExchangeDocument41 pagesGaseous Exchangeapi-202349222No ratings yet
- ICD Reference CodesDocument2 pagesICD Reference CodesRavi Pal100% (1)
- NCP Impaired Gas Exchange STROKEDocument2 pagesNCP Impaired Gas Exchange STROKEMa. Elaine Carla TatingNo ratings yet
- Massage TherapyDocument7 pagesMassage TherapyDan ZkyNo ratings yet
- Respiratory ExaminationDocument18 pagesRespiratory Examinationsuganthi rajesh kannaNo ratings yet
- Notes IV Polygraph InstrumnetDocument4 pagesNotes IV Polygraph InstrumnetKristine Ann QuiñonesNo ratings yet
- Life Processes TutionDocument37 pagesLife Processes Tutionmanpreet kaurNo ratings yet
- System Wise Physiological ChangesDocument24 pagesSystem Wise Physiological ChangesKinjal VasavaNo ratings yet
- PUFF Expert SystemsDocument12 pagesPUFF Expert SystemsjuampiinNo ratings yet
- Modul Science F3 DLPDocument36 pagesModul Science F3 DLPChuahSiewHoonNo ratings yet
- Spinal Cord Injury Rehabilitation - Jane L. WetzelDocument32 pagesSpinal Cord Injury Rehabilitation - Jane L. WetzelFajrin GumilarNo ratings yet
- Breath Biopsy Complete GuideDocument110 pagesBreath Biopsy Complete Guidemadimadi11No ratings yet