Download as pptx, pdf, or txt
You might also like
- Biology Cheatsheet PDFDocument21 pagesBiology Cheatsheet PDFAhmad Mubashar67% (6)
- Don Tolman - FDR3 - WholeFoodMedicines PDFDocument176 pagesDon Tolman - FDR3 - WholeFoodMedicines PDFLerere Allala100% (4)
- New Anatomy and Physiology of MaculaDocument51 pagesNew Anatomy and Physiology of MaculaPragnya Rao Donthineni75% (4)
- AP Psychology Notes Chapter 6Document4 pagesAP Psychology Notes Chapter 6Danny MeehanNo ratings yet
- Khan Academy Psychology and Sociology Notes Updated EdiitonDocument330 pagesKhan Academy Psychology and Sociology Notes Updated EdiitonDaniel Rusiecki0% (2)
- Biochem Presentation 1 ...Document12 pagesBiochem Presentation 1 ...Rabia HussainNo ratings yet
- Retina Group1 120601041708 Phpapp01Document39 pagesRetina Group1 120601041708 Phpapp01Arpit McWanNo ratings yet
- Lecture 8 Special Senses Part 3-VisionDocument32 pagesLecture 8 Special Senses Part 3-VisionMoses Jr KazevuNo ratings yet
- K4. Aspek Biokimia MataDocument74 pagesK4. Aspek Biokimia MataSarahGustiaWoromboniNo ratings yet
- Retina Monika Pallan & Afasana Pathan: Anatomy & PhysiologyDocument45 pagesRetina Monika Pallan & Afasana Pathan: Anatomy & PhysiologyAsyifaPrellaNo ratings yet
- EyrthrokineticsDocument4 pagesEyrthrokineticsKenneth Jake BatiduanNo ratings yet
- Giai-Phau-Sinh-Ly EnglishDocument29 pagesGiai-Phau-Sinh-Ly EnglishTrang BuiNo ratings yet
- Red Cell.1Document25 pagesRed Cell.1Jude ChinecheremNo ratings yet
- Cell StructureDocument66 pagesCell StructureLiza AmmarNo ratings yet
- Patholo Le2Document31 pagesPatholo Le2bitangyarahNo ratings yet
- Function RpeDocument4 pagesFunction RpeKristine Ramos100% (1)
- Physiology of The Vitreous: - Moderator: Dr. Sangi Jelkeba, MD, Ophthalmologist)Document61 pagesPhysiology of The Vitreous: - Moderator: Dr. Sangi Jelkeba, MD, Ophthalmologist)abo kooNo ratings yet
- CorneaDocument41 pagesCorneaNikhil KorripatiNo ratings yet
- Blood: Erythropoeisis by U.SivakumarDocument41 pagesBlood: Erythropoeisis by U.SivakumarAkash JaatNo ratings yet
- Anatomi Fisiologi MataDocument70 pagesAnatomi Fisiologi MataRisalatulNo ratings yet
- Physiology of The Eye: Khorrami PH.DDocument130 pagesPhysiology of The Eye: Khorrami PH.Dkhorrami4No ratings yet
- Anatomy and Physiology of The Eye Opthalmology LectureDocument64 pagesAnatomy and Physiology of The Eye Opthalmology LectureJaikrit SinghNo ratings yet
- Li LBM 4 Mata 2Document30 pagesLi LBM 4 Mata 2Salma SavitaNo ratings yet
- ERYTHROPOISISDocument22 pagesERYTHROPOISISW.F KareemNo ratings yet
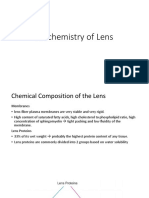
- Biochemistry of LensDocument24 pagesBiochemistry of LensriskhapangestikaNo ratings yet
- Cellular PhysiologyDocument32 pagesCellular Physiologyانس ابوهيبة0% (1)
- Aqueous Humor Dynamics (DR Poonam)Document28 pagesAqueous Humor Dynamics (DR Poonam)Sampitroda DesaiNo ratings yet
- Cor NeaDocument43 pagesCor NeaAdarsh KeshariNo ratings yet
- Human Vision: Physical Apparatus: Nisheeth 8 February 2019Document12 pagesHuman Vision: Physical Apparatus: Nisheeth 8 February 2019Ahsan BarkatiNo ratings yet
- Erythrocytes Red Blood CellsDocument54 pagesErythrocytes Red Blood Cellsclarence fernandezNo ratings yet
- Anatomy-Physiology Eyeball 2023Document75 pagesAnatomy-Physiology Eyeball 2023debdeepbhattacharya411No ratings yet
- Cell 1Document47 pagesCell 1JeniNo ratings yet
- Structural Components of The Cell MembraneDocument2 pagesStructural Components of The Cell MembraneYumiNo ratings yet
- Special SensesDocument23 pagesSpecial SensesÑäd ÉèmNo ratings yet
- Cell 2Document45 pagesCell 2Majd HusseinNo ratings yet
- Cell Organelles by Dr. M. JawedDocument26 pagesCell Organelles by Dr. M. Jawedrv9v7r6fjjNo ratings yet
- Mechanisms of Macular Edema Beyond The SurfaceDocument49 pagesMechanisms of Macular Edema Beyond The SurfaceGustavo RiveraNo ratings yet
- Topic 3Document12 pagesTopic 3Ria AccadNo ratings yet
- Feline Nonregenerative Anemia Pathophysiology and ErilologiesDocument7 pagesFeline Nonregenerative Anemia Pathophysiology and ErilologiesTORRES GUTIERREZ JOYNY RAQUEL catedraticoNo ratings yet
- Cell Strucure & Functions - Part - 1Document23 pagesCell Strucure & Functions - Part - 1Sree Harini SNo ratings yet
- Cell 1Document34 pagesCell 1Majd HusseinNo ratings yet
- Kami Export - F4 C2Document1 pageKami Export - F4 C2Ernice HengNo ratings yet
- AVICENNIA LBM 4 Mata SGD 20Document28 pagesAVICENNIA LBM 4 Mata SGD 20Maylinda Putri100% (1)
- AVICENNIA LBM 4 Mata SGD 20Document28 pagesAVICENNIA LBM 4 Mata SGD 20Maylinda PutriNo ratings yet
- AddDocument3 pagesAddasdfasdfawefawefNo ratings yet
- Retinal Diseases 230210 210855Document108 pagesRetinal Diseases 230210 210855RgdNo ratings yet
- Week 4 5 - Cell Structure - Function (1) (Final)Document44 pagesWeek 4 5 - Cell Structure - Function (1) (Final)hhhhNo ratings yet
- Cell 2Document57 pagesCell 2JeniNo ratings yet
- Ocr A Level Biology CheatsheetDocument21 pagesOcr A Level Biology CheatsheetminaNo ratings yet
- Fluorescein AngiographyDocument81 pagesFluorescein Angiographyeng_25122147100% (4)
- 2 Cell Membrane 20210908Document83 pages2 Cell Membrane 20210908Sayan KonarNo ratings yet
- Retinal Pigment Epithelium (RPE)Document16 pagesRetinal Pigment Epithelium (RPE)ali nazzalNo ratings yet
- Rosemary: Pemicu 2 Kel 15Document151 pagesRosemary: Pemicu 2 Kel 15Rosemary FebrianiNo ratings yet
- The Eye: How Would You Define It?Document9 pagesThe Eye: How Would You Define It?juliaNo ratings yet
- 1.3 Membranes StructureDocument43 pages1.3 Membranes StructuregvreevrevNo ratings yet
- Hema311 Lec - Week 5 - Red Cell Structure, Metabolism, Destruction and FunctionDocument6 pagesHema311 Lec - Week 5 - Red Cell Structure, Metabolism, Destruction and FunctionJayvhie Gulane LayanNo ratings yet
- ANATOMY of Retina, Bruch Membrane, Ora Serrata, Vitreous - Dhita, Dr.Document40 pagesANATOMY of Retina, Bruch Membrane, Ora Serrata, Vitreous - Dhita, Dr.Dhita Dewi AlvianeNo ratings yet
- Membranes Organize The Chemical Activities of CellsDocument31 pagesMembranes Organize The Chemical Activities of CellsShalsa ShafiraNo ratings yet
- Haem Lecture 2.2016 PDFDocument12 pagesHaem Lecture 2.2016 PDFdorsa koraeiNo ratings yet
- Cell MembraneDocument14 pagesCell MembraneGabriel RamosNo ratings yet
- Membrane Structure PDFDocument7 pagesMembrane Structure PDFHyunji KimNo ratings yet
- Cell Motility: From Molecules to OrganismsFrom EverandCell Motility: From Molecules to OrganismsAnne RidleyNo ratings yet
- Red Blood Cells, Functions, Diseases A Simple Guide To The Condition, Diagnosis, Treatment, And Related ConditionsFrom EverandRed Blood Cells, Functions, Diseases A Simple Guide To The Condition, Diagnosis, Treatment, And Related ConditionsNo ratings yet
- Veno Occlusive Disease of RetinaDocument81 pagesVeno Occlusive Disease of RetinaPreetiNo ratings yet
- Age Related Macular Degeneration: Dr. Sriniwas Atal MD. Resident Ophthalmology BpklcosDocument75 pagesAge Related Macular Degeneration: Dr. Sriniwas Atal MD. Resident Ophthalmology BpklcosPreetiNo ratings yet
- Anatomy of Cornea MyDocument59 pagesAnatomy of Cornea MyPreeti100% (1)
- Corneal Scrapping, Gram Stain and CultureDocument62 pagesCorneal Scrapping, Gram Stain and CulturePreetiNo ratings yet
- FM 8-50 Prevention and Medical Management of Laser InjuriesDocument29 pagesFM 8-50 Prevention and Medical Management of Laser InjuriesMark CheneyNo ratings yet
- Clinical Neuro-Ophthalmology-A Practical Guide-2007Document23 pagesClinical Neuro-Ophthalmology-A Practical Guide-2007joaquin mellaNo ratings yet
- What Is ColorDocument8 pagesWhat Is ColorCyprian ObiokoyeNo ratings yet
- DIP Full Notes1 ASH-1Document134 pagesDIP Full Notes1 ASH-1digital love100% (1)
- (English) Vision - Crash Course A&P #18 (DownSub - Com)Document8 pages(English) Vision - Crash Course A&P #18 (DownSub - Com)bank townNo ratings yet
- ADLC Science 8 - Light & Optical Systems PDFDocument33 pagesADLC Science 8 - Light & Optical Systems PDFLizaNo ratings yet
- The Human EyeDocument10 pagesThe Human Eyemargaretziaja1997No ratings yet
- Pra PTS Xi SMS 2Document11 pagesPra PTS Xi SMS 2Ammar KhadafiNo ratings yet
- Physiology of Human EyeDocument6 pagesPhysiology of Human EyeJim Jose AntonyNo ratings yet
- Mariap 1 PDFDocument453 pagesMariap 1 PDFxDragono10No ratings yet
- In Uence of Light Intensity, Spectrum and Orientation On Sea Bass Plasma and Ocular MelatoninDocument7 pagesIn Uence of Light Intensity, Spectrum and Orientation On Sea Bass Plasma and Ocular MelatoninMarko PotočnikNo ratings yet
- Text Book Vision SceinciesDocument316 pagesText Book Vision SceinciesCarpetali GatitaNo ratings yet
- TIF Ch03 10e 41912Document108 pagesTIF Ch03 10e 41912mariseNo ratings yet
- Histology of The EyeDocument5 pagesHistology of The EyeshindyNo ratings yet
- AVR Unit 1 Part 3Document25 pagesAVR Unit 1 Part 3Honey BeeNo ratings yet
- Colour TechnologyDocument38 pagesColour TechnologylthyaguNo ratings yet
- Evolution of Vertebrate EyesDocument14 pagesEvolution of Vertebrate Eyeslurolu1060No ratings yet
- S6 BIO General Principles of Reception and Response in Animalspart1Document31 pagesS6 BIO General Principles of Reception and Response in Animalspart1johnchupa50No ratings yet
- Week 9. PSYC1101 Perception Lecture 1.Document20 pagesWeek 9. PSYC1101 Perception Lecture 1.Billy TherionNo ratings yet
- Genesis Class 4Document14 pagesGenesis Class 4communityfreechurchNo ratings yet
- CHAPTER 3 - SensationDocument59 pagesCHAPTER 3 - Sensationflammy07100% (1)
- Autonomous Street Lighting System Based On Solar Energy and LEDs PDFDocument6 pagesAutonomous Street Lighting System Based On Solar Energy and LEDs PDFlspam89No ratings yet
- Unit Plan Overview: Teacher Candidate Danielle Hickman School Elementry (3rd)Document25 pagesUnit Plan Overview: Teacher Candidate Danielle Hickman School Elementry (3rd)api-372340240No ratings yet
- The Eye The Eyeball Has Three TunicsDocument6 pagesThe Eye The Eyeball Has Three TunicsLara ShayaNo ratings yet
- Psych 101 ReviewerDocument19 pagesPsych 101 ReviewerAngeli Jean Koreen CorpuzNo ratings yet
- Research Statement GabrielleGutierrezDocument6 pagesResearch Statement GabrielleGutierrezGabrielle GutierrezNo ratings yet
- Unit 2 Sense Organs Eyes Skin and TongueDocument33 pagesUnit 2 Sense Organs Eyes Skin and TongueBONGISIPHO HLOPHENo ratings yet