Download as ppt, pdf, or txt
You might also like
- Orthotic Intervention For The Hand and Upper Extremity Splinting PrinciplesDocument61 pagesOrthotic Intervention For The Hand and Upper Extremity Splinting Principleskevin.smart540No ratings yet
- Final ExamDocument7 pagesFinal ExamrileyNo ratings yet
- Physiotherapy MCQsDocument12 pagesPhysiotherapy MCQssurender_singh_4373% (11)
- Chest X-RayDocument101 pagesChest X-RayRizka RamadaniNo ratings yet
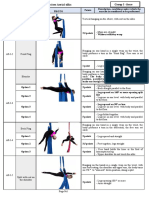
- Appendix 1 Compulsory Exercises Aerial Silk Eng 2018Document23 pagesAppendix 1 Compulsory Exercises Aerial Silk Eng 2018tito1628100% (6)
- Basic Steps in Hula DanceDocument2 pagesBasic Steps in Hula DanceEyn Herrera Granatin100% (1)
- Modul Skill MuskuloskeletalDocument37 pagesModul Skill MuskuloskeletalNI NYOMAN TRIANA WIDHIASTUTINo ratings yet
- Spine 2020Document1 pageSpine 2020fihimeh581No ratings yet
- Physical Examination of Musculoskeletal System 2021Document50 pagesPhysical Examination of Musculoskeletal System 2021RPMFA RPMFANo ratings yet
- Physical Examination of The SpineDocument33 pagesPhysical Examination of The SpineyudiNo ratings yet
- GALS AssessmentDocument46 pagesGALS AssessmentdrindrasNo ratings yet
- Exam KneeDocument11 pagesExam KneesingwongcsNo ratings yet
- Knee Assesment FullDocument17 pagesKnee Assesment FullwidhaNo ratings yet
- OSCE Shoulder Examination: Sunday, May 08, 2011 5:12 PMDocument6 pagesOSCE Shoulder Examination: Sunday, May 08, 2011 5:12 PMproflangaNo ratings yet
- (OSCE) (Checklist) Hip ExaminationDocument7 pages(OSCE) (Checklist) Hip ExaminationastarimediantoNo ratings yet
- Checklist Pemeriksaan Fisik Pada HIP (OSCE) : PendahuluanDocument3 pagesChecklist Pemeriksaan Fisik Pada HIP (OSCE) : PendahuluanFelix joviandiNo ratings yet
- Exploración Funcional CaderaDocument5 pagesExploración Funcional CaderaJosé Antonio MartinezNo ratings yet
- Pyshical Examination OrthopaediDocument67 pagesPyshical Examination OrthopaediSheryl ElitaNo ratings yet
- WK 6 Study QsDocument7 pagesWK 6 Study Qsapi-479720222No ratings yet
- Pengkajian MuskuloskeletalDocument35 pagesPengkajian MuskuloskeletalDEA ZUBAIDAHNo ratings yet
- Pengantar Pemeriksaan Fisik: Dr. Surya Darma, SPPD, FinasimDocument37 pagesPengantar Pemeriksaan Fisik: Dr. Surya Darma, SPPD, FinasimApriyani Supia DewiNo ratings yet
- Exam ShoulderDocument27 pagesExam ShouldersingwongcsNo ratings yet
- Ortho Neuro ExamsDocument0 pagesOrtho Neuro ExamsMaybs Palec Pamplona-ParreñoNo ratings yet
- Muhammad Aditya Alfarizki 71.2017.007: Pembimbing: Dr. Rizal Daulay, SP - OT, MARSDocument25 pagesMuhammad Aditya Alfarizki 71.2017.007: Pembimbing: Dr. Rizal Daulay, SP - OT, MARSaditNo ratings yet
- Physical Examination of The Shoulder FinalDocument28 pagesPhysical Examination of The Shoulder FinalAndinNo ratings yet
- Lec7 Assessment of SpineDocument35 pagesLec7 Assessment of Spinesana mumtazNo ratings yet
- TM Shoulder Exam-1Document36 pagesTM Shoulder Exam-1ratkhiaberNo ratings yet
- GALS Geeky MedicineDocument2 pagesGALS Geeky MedicineJOYBEE JAVIERNo ratings yet
- Upper & Lower Limb ExaminationDocument20 pagesUpper & Lower Limb Examinationcvmqx7yppd100% (1)
- Week 6Document8 pagesWeek 6api-479499469No ratings yet
- PTH 633 Clinical Education Final Group Presentation - GastrocnemiusDocument7 pagesPTH 633 Clinical Education Final Group Presentation - Gastrocnemiusapi-519385428No ratings yet
- Spine: HistoryDocument6 pagesSpine: HistorySham SundarNo ratings yet
- Checklist Hip ExaminationDocument8 pagesChecklist Hip Examinationhakuna matataNo ratings yet
- Workshop PPT (Final) Knee JointDocument127 pagesWorkshop PPT (Final) Knee Jointpasha100% (3)
- Checklist Hip ExaminationDocument7 pagesChecklist Hip ExaminationJavednNo ratings yet
- GALS Examination OSCE GuideDocument10 pagesGALS Examination OSCE GuideSandarekha PereraNo ratings yet
- Faber TestDocument8 pagesFaber TestHaura TsabitahNo ratings yet
- Approach To A Patient With Low Back Ache: DR - Ankur BatraDocument104 pagesApproach To A Patient With Low Back Ache: DR - Ankur BatraAnkur Batra100% (1)
- MED 2.7 Gait and StationDocument3 pagesMED 2.7 Gait and StationelleinasNo ratings yet
- Cerebellar+Examination+Guide+AY+20.21Document5 pagesCerebellar+Examination+Guide+AY+20.21truftybonesNo ratings yet
- Screening Checklist: The Musculoskeletal Screening ExaminationDocument36 pagesScreening Checklist: The Musculoskeletal Screening ExaminationArden GabrielNo ratings yet
- Assessment MusculoskeletalDocument6 pagesAssessment Musculoskeletaldd marshall100% (1)
- 9 Hip & Lumber DDDocument29 pages9 Hip & Lumber DDHeba Abo bakrNo ratings yet
- ShoulderDocument51 pagesShoulderIts LaraNo ratings yet
- Refer - Pdfped PracticalDocument10 pagesRefer - Pdfped PracticalNana BananaNo ratings yet
- Assessment of The Musculo-Skeletal SystemDocument46 pagesAssessment of The Musculo-Skeletal SystemRaquel M. MendozaNo ratings yet
- David Butler Neural Tissue Mobilisation-1Document11 pagesDavid Butler Neural Tissue Mobilisation-1Himani BhondgeNo ratings yet
- Spine ExaminationDocument30 pagesSpine ExaminationNadia SalwaniNo ratings yet
- SCSCSCDocument44 pagesSCSCSCHONGJYNo ratings yet
- Assessing The MusculoskeletalDocument5 pagesAssessing The MusculoskeletalYudi TrigunaNo ratings yet
- WK 3 Chiro TableDocument4 pagesWK 3 Chiro Tableapi-469904011No ratings yet
- Reading Knee - RamaDocument33 pagesReading Knee - RamavjhvghcghcghghNo ratings yet
- Mastering Your Musculoskeletal Exam: Laurel Short, MSN, FNP-CDocument46 pagesMastering Your Musculoskeletal Exam: Laurel Short, MSN, FNP-CPrathap Kumar0% (1)
- Checklist For Neurological Examination of The Lower Limb: Item Achieved Not AchievedDocument2 pagesChecklist For Neurological Examination of The Lower Limb: Item Achieved Not AchievedMohammad Abd-AlhafezNo ratings yet
- Spine ExamDocument4 pagesSpine ExamSaberNo ratings yet
- Lumbar Pain OpiDocument34 pagesLumbar Pain OpiAfifah Dienillah KhusnunNo ratings yet
- GALS ExamDocument6 pagesGALS ExamMaurensia MaurenNo ratings yet
- Examination of The Peripheral Neurological SystemDocument2 pagesExamination of The Peripheral Neurological Systemkenners100% (12)
- Physical Assessment On Musculosceletal SystemDocument14 pagesPhysical Assessment On Musculosceletal SystemilhamNo ratings yet
- Cerebellar DisordersDocument29 pagesCerebellar DisordersArslan Aslam100% (1)
- Cervical Ortho TestsDocument74 pagesCervical Ortho Testsjdavis3100% (1)
- Musculoskeletal SystemDocument5 pagesMusculoskeletal SystemDale Ros CollamatNo ratings yet
- Special Tests LeDocument9 pagesSpecial Tests Lenurasyikah0% (1)
- Gait and StationDocument17 pagesGait and Stationsarguss14100% (3)
- Achilles Tendon Rupture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAchilles Tendon Rupture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Popliteal Muscle Tear, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Popliteal Muscle Tear, Diagnosis, Treatment and Related ConditionsNo ratings yet
- The Genetic Aspect and Morphological Appearance of AchondrogenesisDocument10 pagesThe Genetic Aspect and Morphological Appearance of AchondrogenesisRizka RamadaniNo ratings yet
- Association Between Maternal Age and Birth Defects of Unknown Etiology United States, 1997 2007Document18 pagesAssociation Between Maternal Age and Birth Defects of Unknown Etiology United States, 1997 2007Rizka RamadaniNo ratings yet
- Evaluation of The Effect of Antenatal Betamethasone On Neonatal Respiratory Morbidities in Late Preterm Deliveries (34-37 Weeks)Document9 pagesEvaluation of The Effect of Antenatal Betamethasone On Neonatal Respiratory Morbidities in Late Preterm Deliveries (34-37 Weeks)Rizka RamadaniNo ratings yet
- Review Article: Maternal and Pediatric Health Outcomes in Relation To Gestational Vitamin D SufficiencyDocument10 pagesReview Article: Maternal and Pediatric Health Outcomes in Relation To Gestational Vitamin D SufficiencyRizka RamadaniNo ratings yet
- Headache Nyeri Kepala Vertigo Koma Coma Weakness Hemiparese Kuliah Pengantar Panum Algoritme 2018Document49 pagesHeadache Nyeri Kepala Vertigo Koma Coma Weakness Hemiparese Kuliah Pengantar Panum Algoritme 2018Rizka RamadaniNo ratings yet
- Diagnostic Skill - Visceralpain2018Document26 pagesDiagnostic Skill - Visceralpain2018Rizka RamadaniNo ratings yet
- Project LayoutDocument5 pagesProject LayoutMatthew MaxwellNo ratings yet
- L6. Muscular System (2021-22)Document32 pagesL6. Muscular System (2021-22)Ahmed AfashNo ratings yet
- Gymnastics and Rope ClimbingDocument84 pagesGymnastics and Rope Climbingeuan00100% (14)
- Iyengar Headstand PDFDocument15 pagesIyengar Headstand PDFFelice Chew100% (3)
- Kettlebell Sport Athlete Preparation 2014pdfDocument61 pagesKettlebell Sport Athlete Preparation 2014pdfAirson Negro Jr.67% (3)
- CLASS LCTURE 4 Fudamentals in Phil Folk DanceDocument4 pagesCLASS LCTURE 4 Fudamentals in Phil Folk DanceMarria FrancezcaNo ratings yet
- Medical TerminologyDocument33 pagesMedical TerminologyJJKNo ratings yet
- Canine Radiographs by Louisa White: Click Skeleton To EnterDocument455 pagesCanine Radiographs by Louisa White: Click Skeleton To EnteranacampsNo ratings yet
- Upper Limb AnatomyDocument15 pagesUpper Limb AnatomyAjennyKinoNo ratings yet
- Sukshma VyayamaDocument11 pagesSukshma VyayamaSubramanya SeshagiriNo ratings yet
- Teaching Ideas: Unit 1 Plants and Humans As Organisms Possible LessonsDocument5 pagesTeaching Ideas: Unit 1 Plants and Humans As Organisms Possible LessonsVeni DwintasariNo ratings yet
- D1 Brosur BusDuct Legrand MRzucchini BusbarDocument29 pagesD1 Brosur BusDuct Legrand MRzucchini BusbarAgung NugrahaNo ratings yet
- Chapter 2Document11 pagesChapter 2Agatha OfrecioNo ratings yet
- Junior WAEC Past Question - Physical & Health Education (PDF - Io)Document23 pagesJunior WAEC Past Question - Physical & Health Education (PDF - Io)Chris OryaNo ratings yet
- Hand and Wrist Swelling Management Jul18Document2 pagesHand and Wrist Swelling Management Jul18testNo ratings yet
- Hemophilia Joint Health Score HJHSDocument1 pageHemophilia Joint Health Score HJHSDebashis SamantarayNo ratings yet
- حلول جراحه ماينر 11Document14 pagesحلول جراحه ماينر 11Yousif AlaaNo ratings yet
- Tennis Elbow ExercisesDocument2 pagesTennis Elbow Exercisesmoutasim mohammadNo ratings yet
- Fractures of The Upper LimbDocument20 pagesFractures of The Upper LimbWendy Francisca Borquez PerezNo ratings yet
- The Acumoxa Treatment of Shoulder Impingement SyndromeDocument8 pagesThe Acumoxa Treatment of Shoulder Impingement SyndromeAngela PagliusoNo ratings yet
- The Physiology of Guitar Playing IznaolaDocument37 pagesThe Physiology of Guitar Playing IznaolaJacopo Rognini100% (1)
- South Narcs PSPDocument66 pagesSouth Narcs PSPTruco El MartinezNo ratings yet
- Team Sports FQ1 FQ2Document11 pagesTeam Sports FQ1 FQ2Loving AngelNo ratings yet
- Bsoa 2 Keyboarding ModuleDocument11 pagesBsoa 2 Keyboarding Modulevenus camposanoNo ratings yet
- Total Posture MobilityDocument14 pagesTotal Posture MobilityAndres CastroNo ratings yet