Download as pptx, pdf, or txt
You might also like
- Full Download Gordis Epidemiology 6th Edition Celentano Test BankDocument34 pagesFull Download Gordis Epidemiology 6th Edition Celentano Test Bankjamboolflexuous.el62498% (42)
- OsteosarcomaDocument15 pagesOsteosarcomaDesiree Guerra100% (1)
- Neoplasma Muskuloskeletal - PRMMDocument48 pagesNeoplasma Muskuloskeletal - PRMMhello from the other sideNo ratings yet
- Tumors of Musculoskeletal: Tutorial Ortopaedic SurgeryDocument108 pagesTumors of Musculoskeletal: Tutorial Ortopaedic SurgeryfarisNo ratings yet
- Tumours: Will Aston, Timothy Briggs, Louis SolomonDocument24 pagesTumours: Will Aston, Timothy Briggs, Louis SolomonShuvashishSunuwarNo ratings yet
- Benign Bone TumorsDocument31 pagesBenign Bone TumorsDr Afsar KhanNo ratings yet
- Bone and Joint TumoursDocument49 pagesBone and Joint TumoursMahmoud Abu Al Amrain100% (1)
- Bone Tumours: - Jeffrey Pradeep RajDocument42 pagesBone Tumours: - Jeffrey Pradeep RajjeffreyprajNo ratings yet
- Tumor MusculoskeletalDocument41 pagesTumor Musculoskeletalrisky setyanNo ratings yet
- Bone and Joint Neoplasm or TumorDocument49 pagesBone and Joint Neoplasm or Tumorendah rahmadaniNo ratings yet
- Bone Tumours: Natasha Eleena Nor Maghfirah Hani Farhana Nur FadhilaDocument85 pagesBone Tumours: Natasha Eleena Nor Maghfirah Hani Farhana Nur FadhilaWan Nur AdilahNo ratings yet
- Bone Tumors: Benign Tumor Malignant TumorDocument5 pagesBone Tumors: Benign Tumor Malignant TumorManish ShresthaNo ratings yet
- Vitoss - Bone StickyDocument71 pagesVitoss - Bone StickySorin BarbuNo ratings yet
- Orthopedic Tumors and OsteoarthritisDocument6 pagesOrthopedic Tumors and OsteoarthritisSai Snigdha MohantyNo ratings yet
- 3 - Imaging Hand Tumours FESSHDocument37 pages3 - Imaging Hand Tumours FESSHProfesseur Christian DumontierNo ratings yet
- BONE TUMOURS (Benign)Document42 pagesBONE TUMOURS (Benign)Ayush ChaliseNo ratings yet
- 6.musculoskeletal TumorsDocument110 pages6.musculoskeletal Tumorslina jamalNo ratings yet
- Referat Primery Bone TumorsDocument62 pagesReferat Primery Bone Tumorsrahma nilasari100% (1)
- Musculoskelet Al Tumors: Rizal Daulay MD, Spot. MarsDocument98 pagesMusculoskelet Al Tumors: Rizal Daulay MD, Spot. MarsMuhammad AdityaNo ratings yet
- MS TumorsDocument16 pagesMS TumorsASM MutahirNo ratings yet
- Septic ArthritisDocument94 pagesSeptic ArthritisCut Riska NovizaNo ratings yet
- X-Ray: Most Useful of All ImagingDocument33 pagesX-Ray: Most Useful of All ImagingDinesh VeraNo ratings yet
- Tumors Around Knee in PediatricsDocument25 pagesTumors Around Knee in PediatricsMike RossNo ratings yet
- Dr. Ronald V. Munthe Spot SMF Bedah Rs UkiDocument50 pagesDr. Ronald V. Munthe Spot SMF Bedah Rs UkiOdilia Maria RahalusNo ratings yet
- An Approach To Malignant.7496050.PowerpointDocument19 pagesAn Approach To Malignant.7496050.PowerpointAndrei OlaruNo ratings yet
- Bone Tumor & Tumor-Like Lesions: By: Dr. Manal NageebDocument56 pagesBone Tumor & Tumor-Like Lesions: By: Dr. Manal NageebSonny WijanarkoNo ratings yet
- Bone Tumor: Daniel A. (Orthopedic Surgeon)Document225 pagesBone Tumor: Daniel A. (Orthopedic Surgeon)mebrieNo ratings yet
- Bone TumorsDocument40 pagesBone TumorsVisura PrabodNo ratings yet
- Neoplasm On Bone and Soft Tissue MikoDocument151 pagesNeoplasm On Bone and Soft Tissue Mikoindra muhammadNo ratings yet
- Short Version Malignant Bone LesionsDocument57 pagesShort Version Malignant Bone LesionsAfNo ratings yet
- Bone Tumor: Kemas M Dahlan Fahriza UtamaDocument65 pagesBone Tumor: Kemas M Dahlan Fahriza UtamaAyu Ersya WindiraNo ratings yet
- General Principles of Bone TumorsDocument6 pagesGeneral Principles of Bone TumorsRonald TejoprayitnoNo ratings yet
- Bone tm3Document57 pagesBone tm3ZakiyahulfahdwNo ratings yet
- Benign Bone TumoursDocument106 pagesBenign Bone TumoursBharath NarasimhaNo ratings yet
- Tumours: Apley 9th Ed p.187-223Document66 pagesTumours: Apley 9th Ed p.187-223Helmi IsmunandarNo ratings yet
- Patologi Anatomi Kelainan MuskuloskeletalDocument38 pagesPatologi Anatomi Kelainan Muskuloskeletalmuthia saniNo ratings yet
- Dr. Andre Sihombing. SpotDocument56 pagesDr. Andre Sihombing. SpotDinda AdiaNo ratings yet
- Slide Ajar B.2 Asdos 2015Document111 pagesSlide Ajar B.2 Asdos 2015Kumala DewiNo ratings yet
- Bone TumorsDocument15 pagesBone Tumorssarguss1450% (2)
- Classification of Bone Tumors PDFDocument5 pagesClassification of Bone Tumors PDFnmahpbooksNo ratings yet
- Presenbone Tumors Irfantation1Document65 pagesPresenbone Tumors Irfantation1Ya Sayyadi BilalNo ratings yet
- Bone Tumors ImagingDocument15 pagesBone Tumors ImagingPedro Gabriel Quispe LópezNo ratings yet
- U.S. Andersen Author and SpeakerDocument57 pagesU.S. Andersen Author and SpeakerrerenNo ratings yet
- ABC Bone CystDocument43 pagesABC Bone CystIrfan Ullah KhanNo ratings yet
- Bone Tumor FinalDocument156 pagesBone Tumor Finalavni_stormNo ratings yet
- Pemeriksaan Radiology OnkologiDocument51 pagesPemeriksaan Radiology OnkologiGesta Qurrotu AyuninnataNo ratings yet
- Chest Wall and Chest Wall Neoplasms: Dr. Alfredo M. IgamaDocument11 pagesChest Wall and Chest Wall Neoplasms: Dr. Alfredo M. Igamaredz_ekg619No ratings yet
- Overview of Musculoskeletal TumorsDocument14 pagesOverview of Musculoskeletal TumorskylieverNo ratings yet
- Approach To Bone Tumor DiagnosisDocument25 pagesApproach To Bone Tumor DiagnosisFatini ChokNo ratings yet
- Booooooone Tumors REFERATDocument47 pagesBooooooone Tumors REFERATNurlaila IshaqNo ratings yet
- Neoplasms Ear CanalDocument12 pagesNeoplasms Ear CanalannaNo ratings yet
- Kuliah Blok Neoplasma - Januari 2011Document161 pagesKuliah Blok Neoplasma - Januari 2011Natallia BatuwaelNo ratings yet
- Dr. Rajasekhar A. National Pathology Laboratory HyderabadDocument26 pagesDr. Rajasekhar A. National Pathology Laboratory HyderabadAmit KumarNo ratings yet
- Kuliah Blok Neoplasma - Januari 2011 - 2Document161 pagesKuliah Blok Neoplasma - Januari 2011 - 2Natallia BatuwaelNo ratings yet
- 08 Bone TumorsDocument94 pages08 Bone TumorsSara FoudaNo ratings yet
- Bone Tumors FinalDocument80 pagesBone Tumors FinalPATHMAPRIYA GANESANNo ratings yet
- Chapter 12: Bone TumorsDocument14 pagesChapter 12: Bone TumorspoddataNo ratings yet
- Bone TumorsDocument43 pagesBone TumorsIsaac MwangiNo ratings yet
- Diagnosis of Bone Tumours: 1. Age of Patient 2. Location of Tumour 3. Radiological Appearance 4. Histological FeaturesDocument69 pagesDiagnosis of Bone Tumours: 1. Age of Patient 2. Location of Tumour 3. Radiological Appearance 4. Histological Featuresyurie_ameliaNo ratings yet
- Soft Tissue Tumors: A Practical and Comprehensive Guide to Sarcomas and Benign NeoplasmsFrom EverandSoft Tissue Tumors: A Practical and Comprehensive Guide to Sarcomas and Benign NeoplasmsNo ratings yet
- Pharmacokinetics Processes, Absorption, Distribution, Metabolism, Excretion, and Individualized TherapyDocument50 pagesPharmacokinetics Processes, Absorption, Distribution, Metabolism, Excretion, and Individualized TherapyIdris Balasa IdrisNo ratings yet
- LARGE JOINTS IN HEALTH AND DiseaseDocument75 pagesLARGE JOINTS IN HEALTH AND DiseaseIdris Balasa IdrisNo ratings yet
- Common Childhood Malignancies Radiology Rev CourseDocument35 pagesCommon Childhood Malignancies Radiology Rev CourseIdris Balasa IdrisNo ratings yet
- Anaemias: BY Osunkalu VincentDocument15 pagesAnaemias: BY Osunkalu VincentIdris Balasa IdrisNo ratings yet
- Anatomy 1st Paper September 2011Document1 pageAnatomy 1st Paper September 2011Idris Balasa IdrisNo ratings yet
- DocumentDocument2 pagesDocumentIdris Balasa IdrisNo ratings yet
- List and Discuss The Imaging Features of Cerebellopontine Angle MassesDocument39 pagesList and Discuss The Imaging Features of Cerebellopontine Angle MassesIdris Balasa IdrisNo ratings yet
- The Effect of Clown Intervention On Self-Report and Biomarker Measures of Stress and Fatigue in Pediatric Osteosarcoma Inpatients - A Pilot StudyDocument13 pagesThe Effect of Clown Intervention On Self-Report and Biomarker Measures of Stress and Fatigue in Pediatric Osteosarcoma Inpatients - A Pilot StudyMarcela HincapiéNo ratings yet
- Schreibman - Bone Tumors in 1 Simple ChartDocument31 pagesSchreibman - Bone Tumors in 1 Simple ChartborstNo ratings yet
- 2012 UpmcccanualreportDocument70 pages2012 Upmcccanualreportapi-290001443No ratings yet
- Orthopedics MnemonicsDocument8 pagesOrthopedics MnemonicsCristol MyersNo ratings yet
- Pediatric Bone TumorsDocument20 pagesPediatric Bone TumorsFelipe VenegasNo ratings yet
- Bone Cancer: by Mayo Clinic StaffDocument7 pagesBone Cancer: by Mayo Clinic Staffalura1123No ratings yet
- Neoplasma MuskuloskeletalDocument173 pagesNeoplasma Muskuloskeletaldiannisa rahmaNo ratings yet
- Sarcoma: StatisticsDocument1 pageSarcoma: StatisticsAngelica LupuNo ratings yet
- X Rays and Topics 2020Document62 pagesX Rays and Topics 2020Andreea MihaelaNo ratings yet
- Who Classificação TO 2022 PDFDocument13 pagesWho Classificação TO 2022 PDFGrasieli RamosNo ratings yet
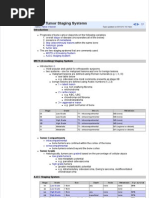
- Bone Tumour Staging - PathologyDocument2 pagesBone Tumour Staging - Pathologyo7113No ratings yet
- Narrative PathophysiologyDocument5 pagesNarrative Pathophysiologymyer pasandalanNo ratings yet
- 08 Bone TumorsDocument94 pages08 Bone TumorsSara FoudaNo ratings yet
- Miracle Hospital Study GuideDocument31 pagesMiracle Hospital Study GuideMel ClancyNo ratings yet
- Orthopaedics: Course Content TopicsDocument4 pagesOrthopaedics: Course Content TopicsRaghu VeerNo ratings yet
- Orthoheal - DNB Ortho Theory Question Papers AnalysisDocument29 pagesOrthoheal - DNB Ortho Theory Question Papers AnalysisSivaprasath JaganathanNo ratings yet
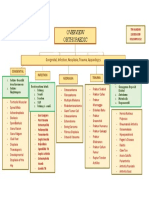
- Orthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesDocument1 pageOrthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesdinsNo ratings yet
- Case Study On Bone CancersDocument6 pagesCase Study On Bone CancersBhanodaya DokalaNo ratings yet
- Classification of Bone Tumors PDFDocument5 pagesClassification of Bone Tumors PDFnmahpbooksNo ratings yet
- 2014 Musculoskeletal Tumors and DiseasesDocument102 pages2014 Musculoskeletal Tumors and DiseasesNanda GemaNo ratings yet
- Blok 10 03.11.2017Document174 pagesBlok 10 03.11.2017VaniaNo ratings yet
- Osteosarcoma 1Document9 pagesOsteosarcoma 1Md Ahsanuzzaman PinkuNo ratings yet
- Tumors of Musculoskeletal: Tutorial Ortopaedic SurgeryDocument108 pagesTumors of Musculoskeletal: Tutorial Ortopaedic SurgeryfarisNo ratings yet
- WHO Classification of Tumors of Soft Tissue and BoneDocument6 pagesWHO Classification of Tumors of Soft Tissue and BoneDevi MirandaNo ratings yet
- SynoviomaDocument28 pagesSynoviomaAnonymous bE4VegCcNo ratings yet
- Single-Cell and Spatial Transcriptomics Reveal Metastasis Mechanism and Microenvironment Remodeling of Lymph Node in OsteosarcomaDocument19 pagesSingle-Cell and Spatial Transcriptomics Reveal Metastasis Mechanism and Microenvironment Remodeling of Lymph Node in Osteosarcomaguptaraghav343No ratings yet
- Oral Path I Combined PDFDocument68 pagesOral Path I Combined PDFpriyasargunanNo ratings yet
- Doh Communicable DiseasesDocument89 pagesDoh Communicable Diseasesapi-3853350100% (6)