Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ipu Admit Card PDFDocument4 pagesIpu Admit Card PDFAbhinav DixitNo ratings yet
- Pivotal TrialDocument36 pagesPivotal TrialDr MonikaNo ratings yet
- IDA in CKDDocument7 pagesIDA in CKDDr MonikaNo ratings yet
- Pathogenesis, Evaluation and Diagnosis of LupusDocument113 pagesPathogenesis, Evaluation and Diagnosis of LupusDr MonikaNo ratings yet
- Potential Phytopharmaceutical Constituents of Solanum Trilobatum L As Significant Inhibitors Against COVID-19 Robust-B v2Document51 pagesPotential Phytopharmaceutical Constituents of Solanum Trilobatum L As Significant Inhibitors Against COVID-19 Robust-B v2Dr MonikaNo ratings yet
- Pign Vs Irgn: by DR Monika Resident Nephrology, Saveetha CollegeDocument50 pagesPign Vs Irgn: by DR Monika Resident Nephrology, Saveetha CollegeDr MonikaNo ratings yet
- A Guide To The Management of Tuberculosis in Patients With Chronic Liver DiseaseDocument12 pagesA Guide To The Management of Tuberculosis in Patients With Chronic Liver DiseaseMeldaNo ratings yet
- Textile Internship - Usha YarnsDocument49 pagesTextile Internship - Usha YarnsROHAN GIREESHNo ratings yet
- AphishmDocument1 pageAphishmAmit RajputNo ratings yet
- Physics PDFDocument276 pagesPhysics PDFBenjamín Medina CarrilloNo ratings yet
- Optimization of Flexible Manufacturing Systems Using IoTDocument5 pagesOptimization of Flexible Manufacturing Systems Using IoTbijejournalNo ratings yet
- Kubernetes Controllers - The Kubernetes WorkshopDocument70 pagesKubernetes Controllers - The Kubernetes WorkshopOLALEKAN ALEDARENo ratings yet
- Nift MFM Placement PDFDocument40 pagesNift MFM Placement PDFAastha BattuNo ratings yet
- Learning & Development Activity Enrollment Form: Employee-Applicant DataDocument17 pagesLearning & Development Activity Enrollment Form: Employee-Applicant DataEvelyn dela CruzNo ratings yet
- Lab ManualDocument14 pagesLab Manualhak creationNo ratings yet
- Telephone EnglishDocument5 pagesTelephone EnglishZaw WinOoNo ratings yet
- Cobol 1.0Document43 pagesCobol 1.0sarathNo ratings yet
- Catalog Copeland KCLDocument40 pagesCatalog Copeland KCLIsidro MendozaNo ratings yet
- Sepharial - The Science of Foreknowledge Cd13 Id 1928069166 Size603Document114 pagesSepharial - The Science of Foreknowledge Cd13 Id 1928069166 Size603makarandmone100% (9)
- Office THE: OF SecretaryDocument9 pagesOffice THE: OF SecretaryAling KinaiNo ratings yet
- Policy - Task 2 ContentDocument6 pagesPolicy - Task 2 ContentJadhav AmitNo ratings yet
- NKK Handbook For ISM AuditsDocument29 pagesNKK Handbook For ISM Auditsbill baileyNo ratings yet
- 11 HUMSS JQR - Family Earthquake PreparednessDocument4 pages11 HUMSS JQR - Family Earthquake PreparednessCLARIZZE JAINE MANALONo ratings yet
- Anti-Virus Malware DNS Trap FeatureDocument2 pagesAnti-Virus Malware DNS Trap Featuredas zobNo ratings yet
- SuperDoctor5 UserGuideDocument139 pagesSuperDoctor5 UserGuidemlody45No ratings yet
- Ricky C. Alfon: - Individual Differences - (Prof Ed 6) Facilitating Learner-Centered TeachingDocument8 pagesRicky C. Alfon: - Individual Differences - (Prof Ed 6) Facilitating Learner-Centered TeachingMark Joseph DacubaNo ratings yet
- Havkin-Frenkel, Daphna Belanger, Faith C. (2018) - Handbook of Vanilla Science and Technology. Vanilla Diseases.Document14 pagesHavkin-Frenkel, Daphna Belanger, Faith C. (2018) - Handbook of Vanilla Science and Technology. Vanilla Diseases.Victoria PérezNo ratings yet
- Syllabusbtechec1 PDFDocument107 pagesSyllabusbtechec1 PDFAmol AmollNo ratings yet
- Tense Direct Speech Reported SpeechDocument2 pagesTense Direct Speech Reported SpeechChristeena HoàngNo ratings yet
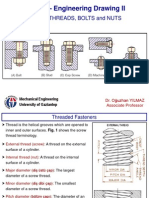
- SCREW THREADS, BOLTS and NUTS PDFDocument10 pagesSCREW THREADS, BOLTS and NUTS PDFhrhgk50% (2)
- RDDocument6 pagesRDViệt HùngNo ratings yet
- Detect Me: DirectionDocument6 pagesDetect Me: DirectionMaymay Auau100% (2)
- ManufuckingscriptDocument13 pagesManufuckingscript가푸타No ratings yet
- Pond Based Tilapia Hatchery ManagementDocument50 pagesPond Based Tilapia Hatchery ManagementAlvin Javier PeranteNo ratings yet
- List of Candidates For Entrance Test of PH D (Tech) in Pharma Through M Pharm & M Tech For Entrance Test 2015 - 2016Document7 pagesList of Candidates For Entrance Test of PH D (Tech) in Pharma Through M Pharm & M Tech For Entrance Test 2015 - 2016mppatilmayur1679No ratings yet