
Ulcerative Colitis
Ulcerative Colitis
You might also like
- Clinical Log Term II PDFDocument9 pagesClinical Log Term II PDFPriscilla S100% (1)
- Biliary Tract Disease - Emmet AndrewsDocument52 pagesBiliary Tract Disease - Emmet AndrewsBoneyJalgarNo ratings yet
- Nursing Care Plan Priorities: Risk For InjuryDocument6 pagesNursing Care Plan Priorities: Risk For InjuryPauling FrezNo ratings yet
- Impact of Right Waste Disposal To The Residents of Barangay 171, CaloocanDocument12 pagesImpact of Right Waste Disposal To The Residents of Barangay 171, CaloocanAljay Mirandilla100% (1)
- Hypertrophic CardiomyopathyDocument37 pagesHypertrophic CardiomyopathyMarko Vukovic100% (1)
- UBICACIONDocument18 pagesUBICACIONCarlos RedrovánNo ratings yet
- CHC VisitDocument48 pagesCHC VisitRamyasree BadeNo ratings yet
- WelcomeDocument60 pagesWelcomepandem soniyaNo ratings yet
- Biliary Tract DiseaseDocument52 pagesBiliary Tract DiseaseAna Cotoman100% (1)
- Chronic DiarrheaDocument66 pagesChronic DiarrheaJulita Yanti100% (1)
- Chronic DiarrheaDocument38 pagesChronic DiarrheaShujina ZainabNo ratings yet
- Acute AbdomenDocument53 pagesAcute AbdomenMahdi DiabNo ratings yet
- Nursing Stomach NotesDocument5 pagesNursing Stomach Noteslucas dibenedettoNo ratings yet
- Abdomen Sheet History-2Document46 pagesAbdomen Sheet History-2خديجة عمرNo ratings yet
- Biliary Tract DiseaseDocument40 pagesBiliary Tract DiseaseIsaac MwangiNo ratings yet
- Biliary&Pancreas DisordersDocument34 pagesBiliary&Pancreas DisordersLarry De LaraNo ratings yet
- GIT DisordersDocument171 pagesGIT DisordersKatrina PonceNo ratings yet
- Disorders of Small IntestineDocument41 pagesDisorders of Small IntestineSamuel kuriaNo ratings yet
- Gastro Inflammatory Bowel DiseasesDocument39 pagesGastro Inflammatory Bowel DiseasesCherish Marie HurbodaNo ratings yet
- "Get in My Belly": Abdominal EmergenciesDocument74 pages"Get in My Belly": Abdominal EmergenciesSherif Abou BakrNo ratings yet
- Acute AbdomenDocument24 pagesAcute AbdomenGrace SimmonsNo ratings yet
- 5.5 GI Disorders Dr. Jison 2022Document72 pages5.5 GI Disorders Dr. Jison 2022Monique BorresNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- PERITONITISDocument12 pagesPERITONITISHayat AL AKOUM100% (1)
- Git LDocument20 pagesGit LafolabiNo ratings yet
- Acute AbdomenDocument21 pagesAcute AbdomenMillicent AwuzieNo ratings yet
- DIVERTICULOSISDocument23 pagesDIVERTICULOSISRashmita DahalNo ratings yet
- "Gosh, Mrs. Doubtfire You Look Pale": Fire" in Television at The Emergency Departement You Worked ForDocument84 pages"Gosh, Mrs. Doubtfire You Look Pale": Fire" in Television at The Emergency Departement You Worked ForAngela Kristiana IntanNo ratings yet
- Student Copy of Gastrointestinal Problems SP 2010 IggyDocument80 pagesStudent Copy of Gastrointestinal Problems SP 2010 IggyJade CentinoNo ratings yet
- Chapter 28 Child With A Gastrointestinal ConditionDocument85 pagesChapter 28 Child With A Gastrointestinal Conditionsey_scottNo ratings yet
- Problem 1: Stefan Satria Group 4Document49 pagesProblem 1: Stefan Satria Group 4Andre OrgantoNo ratings yet
- Disorders of Biliary SystemDocument29 pagesDisorders of Biliary SystemAjibola OlamideNo ratings yet
- PancreatitisDocument59 pagesPancreatitisrimsha waseemNo ratings yet
- Disorders of The Digestive System HandoutsDocument25 pagesDisorders of The Digestive System HandoutsEdelen GaleNo ratings yet
- Dyspepsia GastritisDocument80 pagesDyspepsia GastritisSoumya Ranjan PandaNo ratings yet
- Abdominal Pain: Resources: Murtagh, John. General Practice 5 EdDocument26 pagesAbdominal Pain: Resources: Murtagh, John. General Practice 5 EdDewanti PermatasariNo ratings yet
- Inflammatory Bowel Disease: Younes R YounesDocument38 pagesInflammatory Bowel Disease: Younes R YounesDarawan MirzaNo ratings yet
- Intestinal Obstruction: by Dr. Shereen Abd El-MoniemDocument44 pagesIntestinal Obstruction: by Dr. Shereen Abd El-MoniemフセインNo ratings yet
- 01 - Signs and Symptoms of Git DisordersDocument51 pages01 - Signs and Symptoms of Git DisordersRere AnugrahNo ratings yet
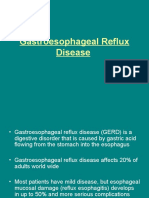
- Gastroesophageal Reflux DiseaseDocument37 pagesGastroesophageal Reflux DiseaseMahad Maxamed AxmedNo ratings yet
- K-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUDocument38 pagesK-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUChristian Lumban GaolNo ratings yet
- Abdominal Emergencies Presentation (Recovered)Document126 pagesAbdominal Emergencies Presentation (Recovered)kityamuwesiNo ratings yet
- GI SlidesDDM1Document39 pagesGI SlidesDDM1Anonymous d3qpXcm4xVNo ratings yet
- Disorders of PancreasDocument41 pagesDisorders of PancreasAbdullah BhattiNo ratings yet
- Approach To The Child With Nausea and Vomiting: by DR - Ryan Al - GhanemiDocument50 pagesApproach To The Child With Nausea and Vomiting: by DR - Ryan Al - GhanemiyusufharkianNo ratings yet
- Assessment and Management of Patients With Biliary DisorderDocument50 pagesAssessment and Management of Patients With Biliary DisorderZanida ZainonNo ratings yet
- NCMB 316 Cu11 Liver, Pancreas, & GallbladderDocument74 pagesNCMB 316 Cu11 Liver, Pancreas, & GallbladderJanine Dela CruzNo ratings yet
- Patients With Noninflammatory Intestinal Disorders: UPNS 232 Adult Health and IllnessDocument41 pagesPatients With Noninflammatory Intestinal Disorders: UPNS 232 Adult Health and Illnesslucas dibenedettoNo ratings yet
- Disease of Esophagus and Hiatal HerniaDocument76 pagesDisease of Esophagus and Hiatal HerniaSiriporn PongpattarapakNo ratings yet
- Biliary Tree LectureDocument58 pagesBiliary Tree Lecturesgod34No ratings yet
- CHOLELITHIASISDocument12 pagesCHOLELITHIASISShenbagam MahalingamNo ratings yet
- 1100 Ultrasound of The Acute Abdomen 15 3Document84 pages1100 Ultrasound of The Acute Abdomen 15 3gp1promo2016No ratings yet
- Autoimmune Pancreatitis: Dr. Arun Gnyawali Resident, General SurgeryDocument27 pagesAutoimmune Pancreatitis: Dr. Arun Gnyawali Resident, General SurgeryArun GnyawaliNo ratings yet
- Chronic Diarrhoea and MalabsorptionDocument25 pagesChronic Diarrhoea and MalabsorptionadelekeyusufNo ratings yet
- INTESTINEDocument98 pagesINTESTINEDeepika LingamNo ratings yet
- GerdDocument43 pagesGerdNidhi shriNo ratings yet
- Abdominal Pain: James S Newman, M.D. The University of Texas Medical BranchDocument27 pagesAbdominal Pain: James S Newman, M.D. The University of Texas Medical BranchYudiese YouNo ratings yet
- Week 14 - BiliaryDocument102 pagesWeek 14 - BiliaryEditha LucasNo ratings yet
- Abdominal PainDocument38 pagesAbdominal PainPro fatherNo ratings yet
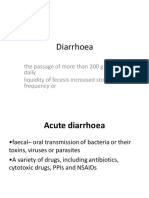
- Diarrhoea: The Passage of More Than 200 G of Stool Daily Liquidity of Fecesis Increased Stool Frequency orDocument23 pagesDiarrhoea: The Passage of More Than 200 G of Stool Daily Liquidity of Fecesis Increased Stool Frequency orUuhhNo ratings yet
- Gastroenterology Ambulatory Medicine Clerkship: Scott Grisolano, MD Division of Gastroenterolgy and Hepatology KumcDocument67 pagesGastroenterology Ambulatory Medicine Clerkship: Scott Grisolano, MD Division of Gastroenterolgy and Hepatology KumcMuath AlzghlellatNo ratings yet
- NCM 116 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns PDFDocument35 pagesNCM 116 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns PDFKathlyn Joy DulayNo ratings yet
- Acute and Chronic GastritisDocument17 pagesAcute and Chronic GastritisIndah Nur PratiwiNo ratings yet
- Gastro Week 5: Gilbert S. 2014Document43 pagesGastro Week 5: Gilbert S. 2014LioraNo ratings yet
- K11 Bedah EsofagusDocument37 pagesK11 Bedah EsofagusenriNo ratings yet
- Hyperosmolar Hyperglycemic Nonketotic Syndrome HHNSDocument12 pagesHyperosmolar Hyperglycemic Nonketotic Syndrome HHNSKyle Ü D. CunanersNo ratings yet
- Epilepsy / Seizures: Roche'e Aguarin BSN - IiiDocument31 pagesEpilepsy / Seizures: Roche'e Aguarin BSN - IiiKyle Ü D. CunanersNo ratings yet
- Path o PhysiologyDocument9 pagesPath o PhysiologyKyle Ü D. CunanersNo ratings yet
- Glaucoma Oral RevalidaDocument11 pagesGlaucoma Oral RevalidaKyle Ü D. CunanersNo ratings yet
- Cva Vs BleedDocument30 pagesCva Vs BleedKyle Ü D. CunanersNo ratings yet
- NCP - Psychiatric SettingDocument20 pagesNCP - Psychiatric SettingKyle Ü D. CunanersNo ratings yet
- Drug StudyDocument20 pagesDrug StudyKyle Ü D. CunanersNo ratings yet
- Ralph Rigor M. Canlapan, RN: Faculty, College of Nursing and Midwifery College of Our Lady of Mt. Carmel - PampangaDocument26 pagesRalph Rigor M. Canlapan, RN: Faculty, College of Nursing and Midwifery College of Our Lady of Mt. Carmel - PampangaKyle Ü D. CunanersNo ratings yet
- Chronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisDocument6 pagesChronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisKyle Ü D. CunanersNo ratings yet
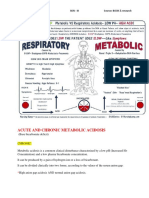
- Acute and Chronic Metabolic Acidosis: Amada, Kevin Moor N. BSN - Iii Source: BOOK & ResearchDocument10 pagesAcute and Chronic Metabolic Acidosis: Amada, Kevin Moor N. BSN - Iii Source: BOOK & ResearchKyle Ü D. CunanersNo ratings yet
- PriorDocument1 pagePriorKyle Ü D. CunanersNo ratings yet
- Table 1. 24 Hours Food Diary Breakfast Number of Serving Kcal CHO Fats ChonDocument1 pageTable 1. 24 Hours Food Diary Breakfast Number of Serving Kcal CHO Fats ChonKyle Ü D. CunanersNo ratings yet
- Adolescent Symptom InventoryDocument6 pagesAdolescent Symptom InventoryКонстантин КрахмалевNo ratings yet
- Soal EssayDocument2 pagesSoal EssayNikolas EdwinNo ratings yet
- Doe v. Abbott - LawsuitDocument68 pagesDoe v. Abbott - LawsuitWashington ExaminerNo ratings yet
- Anestesi Sirkumsisi NeonatusDocument23 pagesAnestesi Sirkumsisi NeonatuscitraNo ratings yet
- Lecture 3 - Iron Homeostasis, AnemiaDocument30 pagesLecture 3 - Iron Homeostasis, AnemiaJoanna BrumaruNo ratings yet
- Report On 470 Bedded General HospitalDocument16 pagesReport On 470 Bedded General HospitalkuldeepNo ratings yet
- Adjustment DisorderDocument4 pagesAdjustment DisorderRosalba GiovannelliNo ratings yet
- Strengths and Difficulties Questionnaire (SDQ) : Informant Parent Young PersonDocument25 pagesStrengths and Difficulties Questionnaire (SDQ) : Informant Parent Young PersonAdjengIkaWulandari100% (2)
- 5 TH Key PointDocument12 pages5 TH Key PointDr-Sanjay SinghaniaNo ratings yet
- Fundamentals of Nursing 1Document2 pagesFundamentals of Nursing 1Alura Marez Doroteo100% (2)
- Distrofia Muscular - DUCHENNEDocument4 pagesDistrofia Muscular - DUCHENNEMariano RamisNo ratings yet
- SettingsDocument2 pagesSettingsbjpalmer100% (3)
- Lesson PlanDocument7 pagesLesson PlanMr. khanNo ratings yet
- Classification of Electrical Installations in Healthcare Jul10 enDocument20 pagesClassification of Electrical Installations in Healthcare Jul10 enAndres ZuñigaNo ratings yet
- Patofisiologi DiareDocument45 pagesPatofisiologi DiareAngela Kristiana Intan100% (1)
- Refractive Amblyopia: I Wayan Ardy Paribrajaka (1871122001)Document17 pagesRefractive Amblyopia: I Wayan Ardy Paribrajaka (1871122001)ratihpdewiNo ratings yet
- Fortune - 2018 - GLM Approach For Youth OffendersDocument10 pagesFortune - 2018 - GLM Approach For Youth OffendersAndrew Myles-WrightNo ratings yet
- NRS 230 Pharmacology Week 1 Students - 11!22!11Document110 pagesNRS 230 Pharmacology Week 1 Students - 11!22!11angieswensonNo ratings yet
- Chronic Pain GuidelinesDocument56 pagesChronic Pain GuidelinesOporadhBiggan100% (1)
- UNIT IV - Bitters N SweetnersDocument30 pagesUNIT IV - Bitters N Sweetnersshweta tyagiNo ratings yet
- Pantothenic AcidDocument34 pagesPantothenic AcidNaji Mohamed AlfatihNo ratings yet
- 7 Types of AdhdDocument3 pages7 Types of AdhdAkbar ShakoorNo ratings yet
- EUA 105 Pfizer Paxlovid FS For HCPs 05242023 - 0Document41 pagesEUA 105 Pfizer Paxlovid FS For HCPs 05242023 - 0bachillerataNo ratings yet
- Soma: Muscle Relaxant For Pain Relief and Comfort.Document6 pagesSoma: Muscle Relaxant For Pain Relief and Comfort.onlinehealthmartNo ratings yet



































































































Download as pptx, pdf, or txt
You might also like
- Clinical Log Term II PDFDocument9 pagesClinical Log Term II PDFPriscilla S100% (1)
- Biliary Tract Disease - Emmet AndrewsDocument52 pagesBiliary Tract Disease - Emmet AndrewsBoneyJalgarNo ratings yet
- Nursing Care Plan Priorities: Risk For InjuryDocument6 pagesNursing Care Plan Priorities: Risk For InjuryPauling FrezNo ratings yet
- Impact of Right Waste Disposal To The Residents of Barangay 171, CaloocanDocument12 pagesImpact of Right Waste Disposal To The Residents of Barangay 171, CaloocanAljay Mirandilla100% (1)
- Hypertrophic CardiomyopathyDocument37 pagesHypertrophic CardiomyopathyMarko Vukovic100% (1)
- UBICACIONDocument18 pagesUBICACIONCarlos RedrovánNo ratings yet
- CHC VisitDocument48 pagesCHC VisitRamyasree BadeNo ratings yet
- WelcomeDocument60 pagesWelcomepandem soniyaNo ratings yet
- Biliary Tract DiseaseDocument52 pagesBiliary Tract DiseaseAna Cotoman100% (1)
- Chronic DiarrheaDocument66 pagesChronic DiarrheaJulita Yanti100% (1)
- Chronic DiarrheaDocument38 pagesChronic DiarrheaShujina ZainabNo ratings yet
- Acute AbdomenDocument53 pagesAcute AbdomenMahdi DiabNo ratings yet
- Nursing Stomach NotesDocument5 pagesNursing Stomach Noteslucas dibenedettoNo ratings yet
- Abdomen Sheet History-2Document46 pagesAbdomen Sheet History-2خديجة عمرNo ratings yet
- Biliary Tract DiseaseDocument40 pagesBiliary Tract DiseaseIsaac MwangiNo ratings yet
- Biliary&Pancreas DisordersDocument34 pagesBiliary&Pancreas DisordersLarry De LaraNo ratings yet
- GIT DisordersDocument171 pagesGIT DisordersKatrina PonceNo ratings yet
- Disorders of Small IntestineDocument41 pagesDisorders of Small IntestineSamuel kuriaNo ratings yet
- Gastro Inflammatory Bowel DiseasesDocument39 pagesGastro Inflammatory Bowel DiseasesCherish Marie HurbodaNo ratings yet
- "Get in My Belly": Abdominal EmergenciesDocument74 pages"Get in My Belly": Abdominal EmergenciesSherif Abou BakrNo ratings yet
- Acute AbdomenDocument24 pagesAcute AbdomenGrace SimmonsNo ratings yet
- 5.5 GI Disorders Dr. Jison 2022Document72 pages5.5 GI Disorders Dr. Jison 2022Monique BorresNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- PERITONITISDocument12 pagesPERITONITISHayat AL AKOUM100% (1)
- Git LDocument20 pagesGit LafolabiNo ratings yet
- Acute AbdomenDocument21 pagesAcute AbdomenMillicent AwuzieNo ratings yet
- DIVERTICULOSISDocument23 pagesDIVERTICULOSISRashmita DahalNo ratings yet
- "Gosh, Mrs. Doubtfire You Look Pale": Fire" in Television at The Emergency Departement You Worked ForDocument84 pages"Gosh, Mrs. Doubtfire You Look Pale": Fire" in Television at The Emergency Departement You Worked ForAngela Kristiana IntanNo ratings yet
- Student Copy of Gastrointestinal Problems SP 2010 IggyDocument80 pagesStudent Copy of Gastrointestinal Problems SP 2010 IggyJade CentinoNo ratings yet
- Chapter 28 Child With A Gastrointestinal ConditionDocument85 pagesChapter 28 Child With A Gastrointestinal Conditionsey_scottNo ratings yet
- Problem 1: Stefan Satria Group 4Document49 pagesProblem 1: Stefan Satria Group 4Andre OrgantoNo ratings yet
- Disorders of Biliary SystemDocument29 pagesDisorders of Biliary SystemAjibola OlamideNo ratings yet
- PancreatitisDocument59 pagesPancreatitisrimsha waseemNo ratings yet
- Disorders of The Digestive System HandoutsDocument25 pagesDisorders of The Digestive System HandoutsEdelen GaleNo ratings yet
- Dyspepsia GastritisDocument80 pagesDyspepsia GastritisSoumya Ranjan PandaNo ratings yet
- Abdominal Pain: Resources: Murtagh, John. General Practice 5 EdDocument26 pagesAbdominal Pain: Resources: Murtagh, John. General Practice 5 EdDewanti PermatasariNo ratings yet
- Inflammatory Bowel Disease: Younes R YounesDocument38 pagesInflammatory Bowel Disease: Younes R YounesDarawan MirzaNo ratings yet
- Intestinal Obstruction: by Dr. Shereen Abd El-MoniemDocument44 pagesIntestinal Obstruction: by Dr. Shereen Abd El-MoniemフセインNo ratings yet
- 01 - Signs and Symptoms of Git DisordersDocument51 pages01 - Signs and Symptoms of Git DisordersRere AnugrahNo ratings yet
- Gastroesophageal Reflux DiseaseDocument37 pagesGastroesophageal Reflux DiseaseMahad Maxamed AxmedNo ratings yet
- K-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUDocument38 pagesK-11 Esophagus: Departemen Bedah Fakultas Kedokteran USUChristian Lumban GaolNo ratings yet
- Abdominal Emergencies Presentation (Recovered)Document126 pagesAbdominal Emergencies Presentation (Recovered)kityamuwesiNo ratings yet
- GI SlidesDDM1Document39 pagesGI SlidesDDM1Anonymous d3qpXcm4xVNo ratings yet
- Disorders of PancreasDocument41 pagesDisorders of PancreasAbdullah BhattiNo ratings yet
- Approach To The Child With Nausea and Vomiting: by DR - Ryan Al - GhanemiDocument50 pagesApproach To The Child With Nausea and Vomiting: by DR - Ryan Al - GhanemiyusufharkianNo ratings yet
- Assessment and Management of Patients With Biliary DisorderDocument50 pagesAssessment and Management of Patients With Biliary DisorderZanida ZainonNo ratings yet
- NCMB 316 Cu11 Liver, Pancreas, & GallbladderDocument74 pagesNCMB 316 Cu11 Liver, Pancreas, & GallbladderJanine Dela CruzNo ratings yet
- Patients With Noninflammatory Intestinal Disorders: UPNS 232 Adult Health and IllnessDocument41 pagesPatients With Noninflammatory Intestinal Disorders: UPNS 232 Adult Health and Illnesslucas dibenedettoNo ratings yet
- Disease of Esophagus and Hiatal HerniaDocument76 pagesDisease of Esophagus and Hiatal HerniaSiriporn PongpattarapakNo ratings yet
- Biliary Tree LectureDocument58 pagesBiliary Tree Lecturesgod34No ratings yet
- CHOLELITHIASISDocument12 pagesCHOLELITHIASISShenbagam MahalingamNo ratings yet
- 1100 Ultrasound of The Acute Abdomen 15 3Document84 pages1100 Ultrasound of The Acute Abdomen 15 3gp1promo2016No ratings yet
- Autoimmune Pancreatitis: Dr. Arun Gnyawali Resident, General SurgeryDocument27 pagesAutoimmune Pancreatitis: Dr. Arun Gnyawali Resident, General SurgeryArun GnyawaliNo ratings yet
- Chronic Diarrhoea and MalabsorptionDocument25 pagesChronic Diarrhoea and MalabsorptionadelekeyusufNo ratings yet
- INTESTINEDocument98 pagesINTESTINEDeepika LingamNo ratings yet
- GerdDocument43 pagesGerdNidhi shriNo ratings yet
- Abdominal Pain: James S Newman, M.D. The University of Texas Medical BranchDocument27 pagesAbdominal Pain: James S Newman, M.D. The University of Texas Medical BranchYudiese YouNo ratings yet
- Week 14 - BiliaryDocument102 pagesWeek 14 - BiliaryEditha LucasNo ratings yet
- Abdominal PainDocument38 pagesAbdominal PainPro fatherNo ratings yet
- Diarrhoea: The Passage of More Than 200 G of Stool Daily Liquidity of Fecesis Increased Stool Frequency orDocument23 pagesDiarrhoea: The Passage of More Than 200 G of Stool Daily Liquidity of Fecesis Increased Stool Frequency orUuhhNo ratings yet
- Gastroenterology Ambulatory Medicine Clerkship: Scott Grisolano, MD Division of Gastroenterolgy and Hepatology KumcDocument67 pagesGastroenterology Ambulatory Medicine Clerkship: Scott Grisolano, MD Division of Gastroenterolgy and Hepatology KumcMuath AlzghlellatNo ratings yet
- NCM 116 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns PDFDocument35 pagesNCM 116 Care of Clients With Ibs Malabsorp Ulcerative Colitis Crohns PDFKathlyn Joy DulayNo ratings yet
- Acute and Chronic GastritisDocument17 pagesAcute and Chronic GastritisIndah Nur PratiwiNo ratings yet
- Gastro Week 5: Gilbert S. 2014Document43 pagesGastro Week 5: Gilbert S. 2014LioraNo ratings yet
- K11 Bedah EsofagusDocument37 pagesK11 Bedah EsofagusenriNo ratings yet
- Hyperosmolar Hyperglycemic Nonketotic Syndrome HHNSDocument12 pagesHyperosmolar Hyperglycemic Nonketotic Syndrome HHNSKyle Ü D. CunanersNo ratings yet
- Epilepsy / Seizures: Roche'e Aguarin BSN - IiiDocument31 pagesEpilepsy / Seizures: Roche'e Aguarin BSN - IiiKyle Ü D. CunanersNo ratings yet
- Path o PhysiologyDocument9 pagesPath o PhysiologyKyle Ü D. CunanersNo ratings yet
- Glaucoma Oral RevalidaDocument11 pagesGlaucoma Oral RevalidaKyle Ü D. CunanersNo ratings yet
- Cva Vs BleedDocument30 pagesCva Vs BleedKyle Ü D. CunanersNo ratings yet
- NCP - Psychiatric SettingDocument20 pagesNCP - Psychiatric SettingKyle Ü D. CunanersNo ratings yet
- Drug StudyDocument20 pagesDrug StudyKyle Ü D. CunanersNo ratings yet
- Ralph Rigor M. Canlapan, RN: Faculty, College of Nursing and Midwifery College of Our Lady of Mt. Carmel - PampangaDocument26 pagesRalph Rigor M. Canlapan, RN: Faculty, College of Nursing and Midwifery College of Our Lady of Mt. Carmel - PampangaKyle Ü D. CunanersNo ratings yet
- Chronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisDocument6 pagesChronic Kidney Disease (CKD) : Diabetes High Blood Pressure Responsible For Up To Two-Thirds GlomerulonephritisKyle Ü D. CunanersNo ratings yet
- Acute and Chronic Metabolic Acidosis: Amada, Kevin Moor N. BSN - Iii Source: BOOK & ResearchDocument10 pagesAcute and Chronic Metabolic Acidosis: Amada, Kevin Moor N. BSN - Iii Source: BOOK & ResearchKyle Ü D. CunanersNo ratings yet
- PriorDocument1 pagePriorKyle Ü D. CunanersNo ratings yet
- Table 1. 24 Hours Food Diary Breakfast Number of Serving Kcal CHO Fats ChonDocument1 pageTable 1. 24 Hours Food Diary Breakfast Number of Serving Kcal CHO Fats ChonKyle Ü D. CunanersNo ratings yet
- Adolescent Symptom InventoryDocument6 pagesAdolescent Symptom InventoryКонстантин КрахмалевNo ratings yet
- Soal EssayDocument2 pagesSoal EssayNikolas EdwinNo ratings yet
- Doe v. Abbott - LawsuitDocument68 pagesDoe v. Abbott - LawsuitWashington ExaminerNo ratings yet
- Anestesi Sirkumsisi NeonatusDocument23 pagesAnestesi Sirkumsisi NeonatuscitraNo ratings yet
- Lecture 3 - Iron Homeostasis, AnemiaDocument30 pagesLecture 3 - Iron Homeostasis, AnemiaJoanna BrumaruNo ratings yet
- Report On 470 Bedded General HospitalDocument16 pagesReport On 470 Bedded General HospitalkuldeepNo ratings yet
- Adjustment DisorderDocument4 pagesAdjustment DisorderRosalba GiovannelliNo ratings yet
- Strengths and Difficulties Questionnaire (SDQ) : Informant Parent Young PersonDocument25 pagesStrengths and Difficulties Questionnaire (SDQ) : Informant Parent Young PersonAdjengIkaWulandari100% (2)
- 5 TH Key PointDocument12 pages5 TH Key PointDr-Sanjay SinghaniaNo ratings yet
- Fundamentals of Nursing 1Document2 pagesFundamentals of Nursing 1Alura Marez Doroteo100% (2)
- Distrofia Muscular - DUCHENNEDocument4 pagesDistrofia Muscular - DUCHENNEMariano RamisNo ratings yet
- SettingsDocument2 pagesSettingsbjpalmer100% (3)
- Lesson PlanDocument7 pagesLesson PlanMr. khanNo ratings yet
- Classification of Electrical Installations in Healthcare Jul10 enDocument20 pagesClassification of Electrical Installations in Healthcare Jul10 enAndres ZuñigaNo ratings yet
- Patofisiologi DiareDocument45 pagesPatofisiologi DiareAngela Kristiana Intan100% (1)
- Refractive Amblyopia: I Wayan Ardy Paribrajaka (1871122001)Document17 pagesRefractive Amblyopia: I Wayan Ardy Paribrajaka (1871122001)ratihpdewiNo ratings yet
- Fortune - 2018 - GLM Approach For Youth OffendersDocument10 pagesFortune - 2018 - GLM Approach For Youth OffendersAndrew Myles-WrightNo ratings yet
- NRS 230 Pharmacology Week 1 Students - 11!22!11Document110 pagesNRS 230 Pharmacology Week 1 Students - 11!22!11angieswensonNo ratings yet
- Chronic Pain GuidelinesDocument56 pagesChronic Pain GuidelinesOporadhBiggan100% (1)
- UNIT IV - Bitters N SweetnersDocument30 pagesUNIT IV - Bitters N Sweetnersshweta tyagiNo ratings yet
- Pantothenic AcidDocument34 pagesPantothenic AcidNaji Mohamed AlfatihNo ratings yet
- 7 Types of AdhdDocument3 pages7 Types of AdhdAkbar ShakoorNo ratings yet
- EUA 105 Pfizer Paxlovid FS For HCPs 05242023 - 0Document41 pagesEUA 105 Pfizer Paxlovid FS For HCPs 05242023 - 0bachillerataNo ratings yet
- Soma: Muscle Relaxant For Pain Relief and Comfort.Document6 pagesSoma: Muscle Relaxant For Pain Relief and Comfort.onlinehealthmartNo ratings yet