Download as pptx, pdf, or txt
You might also like
- Fascial SpacesDocument17 pagesFascial SpacesAlaa MoradNo ratings yet
- Document MergedDocument105 pagesDocument MergedAhmad AlQahtaniNo ratings yet
- Spread of InflamationDocument14 pagesSpread of InflamationShadeeBreijiehNo ratings yet
- 3,2 - Spread of InflamationDocument14 pages3,2 - Spread of Inflamationحمزة تلاحمةNo ratings yet
- Acute Periapical AbscessDocument12 pagesAcute Periapical AbscessDarshilNo ratings yet
- Differential Diagnosis of Palatal SwellingsDocument90 pagesDifferential Diagnosis of Palatal SwellingsAME DENTAL COLLEGE RAICHUR, KARNATAKA100% (2)
- 9 Odontogenic Infections and Pyogenic Infections of The Soft TissuesDocument9 pages9 Odontogenic Infections and Pyogenic Infections of The Soft Tissuesاحمد سلامNo ratings yet
- PERICORONITIS5Document15 pagesPERICORONITIS5dentist40No ratings yet
- Chapter-18 - Orofacial Infection and Its SpreadDocument6 pagesChapter-18 - Orofacial Infection and Its Spreadbjahboi2No ratings yet
- Ludwig's AnginaDocument14 pagesLudwig's Anginafreelancer.am1302No ratings yet
- Histology: Diagnosis and Treatment of Acute Apical AbscessDocument4 pagesHistology: Diagnosis and Treatment of Acute Apical AbscessPrince AmiryNo ratings yet
- Cellulitis: A.prof. Keam Born. Dental Department of Khmer Soviet Friendship HospitalDocument183 pagesCellulitis: A.prof. Keam Born. Dental Department of Khmer Soviet Friendship HospitalRaksmey PhanNo ratings yet
- Periapical Lesions: Diseases of The Periapical Tissue LectureDocument7 pagesPeriapical Lesions: Diseases of The Periapical Tissue Lecturekhaled alahmadNo ratings yet
- Ludwig AnginaDocument14 pagesLudwig AnginaAnggri SeptyanNo ratings yet
- Ludwig AnginaDocument6 pagesLudwig AnginarichardananNo ratings yet
- Dental Infections FaizanDocument10 pagesDental Infections FaizanYousef SalemNo ratings yet
- Ludwig's Angina PresentationDocument11 pagesLudwig's Angina PresentationKNo ratings yet
- Chapter 1Document11 pagesChapter 1talaaghaNo ratings yet
- Acute Apical AbscessDocument2 pagesAcute Apical AbscessLily HaslinaNo ratings yet
- 3.part 3 Case History - Intraoral Examination and InvestigationDocument80 pages3.part 3 Case History - Intraoral Examination and InvestigationDR.NITHA WILLYNo ratings yet
- Oral Mucosal Lesions Indenture WearersDocument27 pagesOral Mucosal Lesions Indenture Wearersade ismailNo ratings yet
- Oro-Facial Infection and ManagementDocument80 pagesOro-Facial Infection and ManagementEticha EmbaboNo ratings yet
- Periapical LesionsDocument36 pagesPeriapical LesionsGaddafi HamzaNo ratings yet
- TBR Odontogenic InfectionsDocument34 pagesTBR Odontogenic InfectionsGiePramaNo ratings yet
- Acute Apical PeriodontitisDocument37 pagesAcute Apical PeriodontitisTri Deasy Permata Hati100% (2)
- S Tomato LogyDocument3 pagesS Tomato LogyAjay The RockerNo ratings yet
- Infecciones OdontogenicaDocument18 pagesInfecciones OdontogenicacarlosNo ratings yet
- Odontogenic InfectionsDocument18 pagesOdontogenic InfectionsAlexander LeonNo ratings yet
- Syphilis: DR Muniba SaleemDocument45 pagesSyphilis: DR Muniba SaleemAbdur RehmanNo ratings yet
- Developmental DisturbancesDocument60 pagesDevelopmental DisturbancesDinesh YadavNo ratings yet
- Abscesses Maxillo: Vittorio Carlino MGE VIDocument31 pagesAbscesses Maxillo: Vittorio Carlino MGE VIVittorio CarlinoNo ratings yet
- Sinusitis 2 - New1Document48 pagesSinusitis 2 - New1neferpitouhoeNo ratings yet
- M S I & C: Andibular Pace Nfections OmplicationsDocument89 pagesM S I & C: Andibular Pace Nfections OmplicationsArun panwarNo ratings yet
- Lesions of Oral Soft Tissues in Children PedoDocument74 pagesLesions of Oral Soft Tissues in Children PedoFourthMolar.comNo ratings yet
- Orofacial Fungal InfectionsDocument26 pagesOrofacial Fungal InfectionsDenis KimNo ratings yet
- 3,1 - Periapical Periodontitis 1Document20 pages3,1 - Periapical Periodontitis 1حمزة تلاحمةNo ratings yet
- Aberrant Frenum and Its TreatmentDocument90 pagesAberrant Frenum and Its TreatmentheycoolalexNo ratings yet
- Contents:: Infectious DiseasesDocument87 pagesContents:: Infectious DiseasesdrnainagargNo ratings yet
- Abscess, Lud Wig AnginaDocument64 pagesAbscess, Lud Wig Anginafahim ahamedNo ratings yet
- Odontogenic InfectionsDocument18 pagesOdontogenic Infectionsjhesica.galeanoNo ratings yet
- Sread of InfectionDocument7 pagesSread of InfectionmustafaNo ratings yet
- Purpose StatementDocument46 pagesPurpose Statementade ismailNo ratings yet
- 5 Tongue Root, Floor, Neck PhlegmonDocument30 pages5 Tongue Root, Floor, Neck PhlegmonАлександр ВолошанNo ratings yet
- Oral Inflammation and Ulceration LesionsDocument27 pagesOral Inflammation and Ulceration LesionsVonny MariaNo ratings yet
- Patient With Single Ulcer: Traumatic Injuries Causing Solitary UlcerationsDocument3 pagesPatient With Single Ulcer: Traumatic Injuries Causing Solitary UlcerationshusseinNo ratings yet
- Fascial Space InfectionsDocument15 pagesFascial Space Infectionsali tiwanaNo ratings yet
- Oral Pathology Review NotesDocument4 pagesOral Pathology Review NotesShoyo HinataNo ratings yet
- Ent and Teeth. Lect. MiniDocument61 pagesEnt and Teeth. Lect. MiniAmrAsser KhattabNo ratings yet
- Space InfectionDocument44 pagesSpace InfectionArun panwarNo ratings yet
- Sinus and UlcerDocument19 pagesSinus and UlcerrejwandazvanNo ratings yet
- Notes 231115 225554Document59 pagesNotes 231115 225554محمد عبدالله قائد المحزفيNo ratings yet
- Physicalandchemicalinjuriesoforalcavity 180120174153Document71 pagesPhysicalandchemicalinjuriesoforalcavity 180120174153draryajyoti1No ratings yet
- Kul PA-Oral Cavity & Salivary GlandDocument73 pagesKul PA-Oral Cavity & Salivary GlandDewi Tri ANo ratings yet
- Odontogenic Infections Of Upper Jaw: حلا ــف دمحم ةـشـئاع Group: C2Document24 pagesOdontogenic Infections Of Upper Jaw: حلا ــف دمحم ةـشـئاع Group: C2Hayder HussienNo ratings yet
- Ludwig'S Angina: Ayma Azhar Roll No 174Document17 pagesLudwig'S Angina: Ayma Azhar Roll No 174Ayma AzharNo ratings yet
- Rhadomyoma Mouth Floor OOOE 2010Document5 pagesRhadomyoma Mouth Floor OOOE 2010DrPrabhat Kumar TiwariNo ratings yet
- Natural History of Odontogenic Infection: Maxillary SpacesDocument5 pagesNatural History of Odontogenic Infection: Maxillary SpacesPaolo BonifacioNo ratings yet
- Chronic Infection Endodontic Therapy Root Canal Pathogens CEJ Crown PalatalDocument8 pagesChronic Infection Endodontic Therapy Root Canal Pathogens CEJ Crown PalatalFitria FafifufuNo ratings yet
- 1.1a The Normal Oral Mucosa PDF-2Document18 pages1.1a The Normal Oral Mucosa PDF-2marianaffernandes10No ratings yet
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- Treatment of An Intrabony Defect CombinedDocument29 pagesTreatment of An Intrabony Defect CombinedDR.AMITHBABU.C.BNo ratings yet
- Treatment of FurcationDocument38 pagesTreatment of FurcationDR.AMITHBABU.C.BNo ratings yet
- Signs and Symptoms of Pulpal DiseasesDocument37 pagesSigns and Symptoms of Pulpal DiseasesDR.AMITHBABU.C.BNo ratings yet
- Mandibular Bone Necrosis Caused by Use of ArsenicDocument23 pagesMandibular Bone Necrosis Caused by Use of ArsenicDR.AMITHBABU.C.BNo ratings yet
- One Step PulpDocument36 pagesOne Step PulpDR.AMITHBABU.C.BNo ratings yet
- Extra Cellular Microbes: DR - Amithbabu.C.B Mscd-EndoDocument35 pagesExtra Cellular Microbes: DR - Amithbabu.C.B Mscd-EndoDR.AMITHBABU.C.BNo ratings yet
- Diabetic Neuropathy: Amithbabu.C.B Mscd-EndoDocument19 pagesDiabetic Neuropathy: Amithbabu.C.B Mscd-EndoDR.AMITHBABU.C.BNo ratings yet
- Cell Junctions and AdhesionsDocument24 pagesCell Junctions and AdhesionsDR.AMITHBABU.C.BNo ratings yet
- Trigeminal Neuralgia: Amithbabu.C.B Mscd-EndoDocument18 pagesTrigeminal Neuralgia: Amithbabu.C.B Mscd-EndoDR.AMITHBABU.C.B100% (1)
- Interdisciplinary Diagnosis and Treatment PlanningDocument24 pagesInterdisciplinary Diagnosis and Treatment PlanningDR.AMITHBABU.C.BNo ratings yet
- Treatment Plan in EndodonticsDocument28 pagesTreatment Plan in EndodonticsDR.AMITHBABU.C.BNo ratings yet
- Submitted by DR - Amithbabu.C.BDocument54 pagesSubmitted by DR - Amithbabu.C.BDR.AMITHBABU.C.BNo ratings yet
- 11 - Central IncisorDocument53 pages11 - Central IncisorDR.AMITHBABU.C.BNo ratings yet
- Capsular Pain: Submitted by DR - Amithbabu Mscd-EndoDocument17 pagesCapsular Pain: Submitted by DR - Amithbabu Mscd-EndoDR.AMITHBABU.C.BNo ratings yet
- The Dental PulpDocument12 pagesThe Dental PulpDR.AMITHBABU.C.BNo ratings yet
- Instruments Obs & Gynea PDFDocument19 pagesInstruments Obs & Gynea PDFVibes Usmlee100% (1)
- Hardy ObituaryDocument2 pagesHardy ObituaryNewzjunkyNo ratings yet
- Sistemas de Refrigeracion Industrial en AmoniacoDocument102 pagesSistemas de Refrigeracion Industrial en AmoniacoDiego Trinidad100% (8)
- Fleming's Left Hand Rule (ForDocument8 pagesFleming's Left Hand Rule (Forb_geyl4286No ratings yet
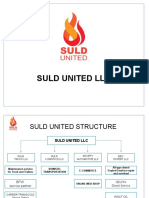
- Suld United PPT2020.09Document31 pagesSuld United PPT2020.09Ulstuguldur Kh.No ratings yet
- Led Music Controller InsructionsDocument2 pagesLed Music Controller InsructionsArnaldoloNo ratings yet
- Creative Beading Vol3 N6Document86 pagesCreative Beading Vol3 N6Rosalba Jg56% (9)
- Extra NumericalsDocument2 pagesExtra NumericalsDeep KambleNo ratings yet
- 4G Wireless PresentationDocument26 pages4G Wireless PresentationArjun ShankaNo ratings yet
- Table of Fundamental Constants in Theoretical PhysicsDocument1 pageTable of Fundamental Constants in Theoretical PhysicsTunarisNo ratings yet
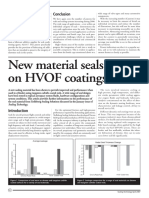
- New Material Seals Better On HVOF CoatingsDocument2 pagesNew Material Seals Better On HVOF Coatingssandbad2100% (2)
- PROGRAMA DE INGLES 11°jeDocument14 pagesPROGRAMA DE INGLES 11°jeJoséNo ratings yet
- EE 413-Engg ElectromagneticsDocument2 pagesEE 413-Engg ElectromagneticsVan GonzalesNo ratings yet
- KM Heavy Duty Clutch - DDocument2 pagesKM Heavy Duty Clutch - DCataNo ratings yet
- Definition of The CaribbeanDocument2 pagesDefinition of The CaribbeanBrianna AllenNo ratings yet
- Datasheet LTH-1550-01Document4 pagesDatasheet LTH-1550-01AntonellaBogadoNo ratings yet
- Sabbaba MenuDocument8 pagesSabbaba Menuaresha6881No ratings yet
- FALLSEM2022-23 BCSE202L TH VL2022230103384 Reference Material I 22-07-2022 DSA Module1 1Document15 pagesFALLSEM2022-23 BCSE202L TH VL2022230103384 Reference Material I 22-07-2022 DSA Module1 1anisha sharmaNo ratings yet
- Essential University Physics 3rd Edition by Wolfson ISBN Test BankDocument23 pagesEssential University Physics 3rd Edition by Wolfson ISBN Test Bankandrea100% (32)
- JKSSB Class IV (28 Feb 2021) EnglishDocument12 pagesJKSSB Class IV (28 Feb 2021) Englishmirziya711No ratings yet
- Extract of All Sales Vouchers 1-Apr-2015 To 31-Dec-2015Document8 pagesExtract of All Sales Vouchers 1-Apr-2015 To 31-Dec-2015taseerNo ratings yet
- Questionnaire Socio-Economic Structure of Small-Scale Coastal Fishermen at Barangay Bonawon, Siaton, Negros OrientalDocument6 pagesQuestionnaire Socio-Economic Structure of Small-Scale Coastal Fishermen at Barangay Bonawon, Siaton, Negros OrientalGuilbert AtilloNo ratings yet
- Power of The BloodDocument14 pagesPower of The BloodEturnal BrandsNo ratings yet
- Quiz - Lab Safety and ApparatusDocument1 pageQuiz - Lab Safety and ApparatusJohn Kristoffer RoblezaNo ratings yet
- 36 - 4 - New York - 08-91 - 1478Document8 pages36 - 4 - New York - 08-91 - 1478Ovo OjasNo ratings yet
- Hermite Cubic Spline CurveDocument4 pagesHermite Cubic Spline CurveKshitij SharmaNo ratings yet
- MMSE Journal Vol.7 2016Document114 pagesMMSE Journal Vol.7 2016Leonardo MonteiroNo ratings yet
- 10.4 Diagnostic Based in Vibrations AnalysisDocument35 pages10.4 Diagnostic Based in Vibrations AnalysisgabrielNo ratings yet
- Yr1 Mid-Year Assessment - Model Test - AnswersDocument2 pagesYr1 Mid-Year Assessment - Model Test - AnswersNieda NorNo ratings yet
- Programmable 3 Channel Power Supply 526Document2 pagesProgrammable 3 Channel Power Supply 526digiarkanandNo ratings yet