Download as ppt, pdf, or txt
You might also like
- Belles Palsy Case Study Group 1Document36 pagesBelles Palsy Case Study Group 1JOEY MEAD ARUGAY100% (1)
- DR - Huang's Notes On Point PropertiesDocument4 pagesDR - Huang's Notes On Point PropertiesCarissa Nichols100% (2)
- HydralazineDocument1 pageHydralazineIvanne Hisoler75% (8)
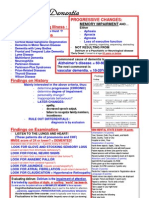
- Alzheimers Dementia Alzheimers Dementia Alzheimers Dementia Alzheimers DementiaDocument5 pagesAlzheimers Dementia Alzheimers Dementia Alzheimers Dementia Alzheimers DementiaTom Mallinson0% (1)
- Anamnesis Dan Diagnosis Topis (Dr. Hendro SP.S)Document27 pagesAnamnesis Dan Diagnosis Topis (Dr. Hendro SP.S)PatrickNicholsNo ratings yet
- CNS - Clinical Evaluation of HemiplegiaDocument36 pagesCNS - Clinical Evaluation of HemiplegiaDipin ManiNo ratings yet
- Neurological Examination Form of Michael Sir PDFDocument27 pagesNeurological Examination Form of Michael Sir PDFShikha Namdev100% (2)
- Dementia & DeliriumDocument7 pagesDementia & DeliriumSudesna Roy ChowdhuryNo ratings yet
- 2.1 Cognitive and Degenerative DisordersDocument73 pages2.1 Cognitive and Degenerative DisordersAbanoub AwadallaNo ratings yet
- A Comprehensive Neurological Examination Guide and Approach To LocalizationDocument86 pagesA Comprehensive Neurological Examination Guide and Approach To LocalizationLiberty AgcaoiliNo ratings yet
- ApproachtocomaDocument65 pagesApproachtocomantnquynhproNo ratings yet
- Case StudiesDocument11 pagesCase StudiesIndah T.INo ratings yet
- Synapse in My Pocket Neuro Exam & Localization - 1st Ed 2020Document63 pagesSynapse in My Pocket Neuro Exam & Localization - 1st Ed 2020SnowyNo ratings yet
- Quiz 3 CombinedDocument6 pagesQuiz 3 CombinedFarah BindakjiNo ratings yet
- PBL 9 Ling HaiDocument3 pagesPBL 9 Ling HaiabdulNo ratings yet
- 12 Slides Seizure DisorderDocument55 pages12 Slides Seizure DisorderDeborah AmodoiNo ratings yet
- Stroke Pharma CaseDocument63 pagesStroke Pharma CaseALI MUMTAZNo ratings yet
- Advances in Alzheimer's Disease: New Technologies, New Ethical Issues (Dr. Steven DeKosky)Document53 pagesAdvances in Alzheimer's Disease: New Technologies, New Ethical Issues (Dr. Steven DeKosky)National Press FoundationNo ratings yet
- 4 Abdominal+ExaminationDocument9 pages4 Abdominal+Examinationمرتضى حسين عبدNo ratings yet
- 2011国际学院意识障碍头痛Document67 pages2011国际学院意识障碍头痛Wai Kwong ChiuNo ratings yet
- Neuromuscular DisordersDocument43 pagesNeuromuscular DisordersReem 10No ratings yet
- Coma Means Dysfunction of Either TheDocument28 pagesComa Means Dysfunction of Either ThedrravikchNo ratings yet
- Neurological SheetDocument70 pagesNeurological SheetKlb ElbnatNo ratings yet
- Review Med SurgDocument14 pagesReview Med SurgjohnpaulvidalNo ratings yet
- Neurological SheetDocument70 pagesNeurological Sheetdrprasant100% (6)
- Neuro Year 3 MedEd Rehaan Khokar 2Document91 pagesNeuro Year 3 MedEd Rehaan Khokar 2Sugoi SagaNo ratings yet
- MS 3 Dementia - Lecture - 2014-15Document50 pagesMS 3 Dementia - Lecture - 2014-15Kreshnik IdrizajNo ratings yet
- First Aid of Psychiatry (PDFDrive)Document223 pagesFirst Aid of Psychiatry (PDFDrive)Bakir JaberNo ratings yet
- SheetDocument10 pagesSheetsushmakar pNo ratings yet
- Wakanda Neuro SpotsDocument40 pagesWakanda Neuro SpotsMiss LindiweNo ratings yet
- Neuro Localisation - LATEST BSP 2024Document106 pagesNeuro Localisation - LATEST BSP 2024bshell61No ratings yet
- QB NeuroDocument30 pagesQB Neurorichard bolinaoNo ratings yet
- Approach To Loss of Counsciousness FinalDocument38 pagesApproach To Loss of Counsciousness FinalManish ShresthaNo ratings yet
- Diagnosis and Management of Multiple SclerosisDocument4 pagesDiagnosis and Management of Multiple SclerosisTom MallinsonNo ratings yet
- How To Make Neurological Diagnosis NewDocument34 pagesHow To Make Neurological Diagnosis NewPeter AsaNo ratings yet
- Moderator: Dr. Rachel Andrews Presenter: Mr. Mahesh Kumar Sharma M.Sc. (Neurosciences NSG.) 1 YrDocument102 pagesModerator: Dr. Rachel Andrews Presenter: Mr. Mahesh Kumar Sharma M.Sc. (Neurosciences NSG.) 1 YrHardeep KaurNo ratings yet
- Neurological Coma: Zainuddin Arpandy, SP.S Neurology Department of Ulin Hospital BanjarmasinDocument24 pagesNeurological Coma: Zainuddin Arpandy, SP.S Neurology Department of Ulin Hospital BanjarmasinDwi Rezky AmaliaNo ratings yet
- Coma LectureDocument30 pagesComa Lecturereem.khafagyyNo ratings yet
- Approach To Body Weakness - StrokeDocument13 pagesApproach To Body Weakness - StrokeHynne Jhea EchavezNo ratings yet
- Neuro InfoDocument11 pagesNeuro Infojennibu1100% (4)
- Cerebrovascular Disease SymptomsDocument17 pagesCerebrovascular Disease Symptomsmannygaming011No ratings yet
- PolyneuropathyDocument17 pagesPolyneuropathyPraluki HerliawanNo ratings yet
- Cerebral Palsy Nursing ManagementDocument25 pagesCerebral Palsy Nursing ManagementpotchistroberriNo ratings yet
- Park Inso N'S Dise ASEDocument132 pagesPark Inso N'S Dise ASEGrace Dela Rosa MelecioNo ratings yet
- Kel.3 Problem 3 KGDDocument57 pagesKel.3 Problem 3 KGDWielda MutafadhilahNo ratings yet
- NCM 116 Prelim Individual RequirementsDocument2 pagesNCM 116 Prelim Individual RequirementsAmirrah LaurenteNo ratings yet
- TG 2 Spinal Cord Trauma (Neuro) PTSD (Psichiatry) - NL - SDDocument38 pagesTG 2 Spinal Cord Trauma (Neuro) PTSD (Psichiatry) - NL - SDNovi AdriNo ratings yet
- Ściąga AnfDocument1 pageŚciąga AnfKasia ManżukNo ratings yet
- Psych 2AP3 - SchizophreniaDocument7 pagesPsych 2AP3 - SchizophreniadeanNo ratings yet
- Comatous, Hypertensive Ensepalopathy, Status EpileptikusDocument71 pagesComatous, Hypertensive Ensepalopathy, Status EpileptikusRey AlwiwikhNo ratings yet
- PMHNP Ancc ReviewDocument4 pagesPMHNP Ancc ReviewEllie Mehr75% (4)
- Paediatric Posting Stage 3.1: End of Posting Questions at December 2015 Short Case Sign DiagnosisDocument3 pagesPaediatric Posting Stage 3.1: End of Posting Questions at December 2015 Short Case Sign DiagnosisayunisallehNo ratings yet
- Cerebral Palsy: A Mini Review: Amrita Kumari, S. YadavDocument10 pagesCerebral Palsy: A Mini Review: Amrita Kumari, S. YadavMahfud HidayatNo ratings yet
- Cerebral Toxoplasmosis in HIV AIDS Patient: Case ReportDocument72 pagesCerebral Toxoplasmosis in HIV AIDS Patient: Case Reportnovy rosalia chandra100% (1)
- Dementia Recentupdates 130920080812 Phpapp01Document58 pagesDementia Recentupdates 130920080812 Phpapp01SantanuNo ratings yet
- PDF DocumentDocument95 pagesPDF DocumentHannah AmerolNo ratings yet
- Clipp 19 PDFDocument9 pagesClipp 19 PDFPrashant MishraNo ratings yet
- Neurological HX TakingDocument3 pagesNeurological HX Takingbloo tomartoNo ratings yet
- Neurology MnemonicsDocument11 pagesNeurology MnemonicsOstaz100% (1)
- Dokumen - Tips - Pediatric Head Trauma Joshua Rocker MD Pediatric Emergency Medicine SchneiderDocument43 pagesDokumen - Tips - Pediatric Head Trauma Joshua Rocker MD Pediatric Emergency Medicine SchneiderKen100% (1)
- Multiple Sclerosis: BY: Ridhima Daga MPT-2 YearDocument130 pagesMultiple Sclerosis: BY: Ridhima Daga MPT-2 YearDurga BhavaniNo ratings yet
- Typhoid Fever: Year III Lecture May 2010Document15 pagesTyphoid Fever: Year III Lecture May 2010Hassen Kavi IsseNo ratings yet
- Lecture On MovementDocument29 pagesLecture On MovementHassen Kavi Isse100% (1)
- Stroke LectureDocument39 pagesStroke LectureHassen Kavi IsseNo ratings yet
- The Neurological History Taking: Osheik Seidi Sunderland Royal Hospital UKDocument38 pagesThe Neurological History Taking: Osheik Seidi Sunderland Royal Hospital UKHassen Kavi Isse100% (3)
- Abdominal Swelling: Ela-BelaDocument48 pagesAbdominal Swelling: Ela-BelaHassen Kavi IsseNo ratings yet
- Acute Rheumatic Fever: Ela-BelaDocument90 pagesAcute Rheumatic Fever: Ela-BelaHassen Kavi IsseNo ratings yet
- Principles of Management of DKADocument4 pagesPrinciples of Management of DKAHassen Kavi IsseNo ratings yet
- Pathophysiology: Adobe Stock, Licensed To Teachmeseries LTDDocument6 pagesPathophysiology: Adobe Stock, Licensed To Teachmeseries LTDNestaNo ratings yet
- Pathophysiology of Hyponatremia in Children: Frontiers in Pediatrics October 2017Document9 pagesPathophysiology of Hyponatremia in Children: Frontiers in Pediatrics October 2017nuhigiartoNo ratings yet
- Disorders of Acid Base BalanceDocument1 pageDisorders of Acid Base BalanceLyn Domingo EllaquezNo ratings yet
- 13 Vassileva Pediatric DRLDocument57 pages13 Vassileva Pediatric DRLLavinia BaracNo ratings yet
- AIF Questionnaire: Acute Intestinal Failure Special Interest GroupDocument5 pagesAIF Questionnaire: Acute Intestinal Failure Special Interest GroupYacine Tarik AizelNo ratings yet
- MB Rules and Main Other ConditionDocument54 pagesMB Rules and Main Other ConditionDevi TresmiatiNo ratings yet
- Barthels Index of ADLs PDFDocument4 pagesBarthels Index of ADLs PDFWindaNo ratings yet
- Module 18: Casualty Monitoring: TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document14 pagesModule 18: Casualty Monitoring: TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Luis-alfredo Perez Bolde HernandezNo ratings yet
- Dengue DRUG StudyDocument4 pagesDengue DRUG Studyjaninenicole100% (1)
- Mary MallonDocument4 pagesMary MallonChristelle MalaitNo ratings yet
- Data KC Perdesa 25 Juni SD 6 Juli 2021Document58 pagesData KC Perdesa 25 Juni SD 6 Juli 2021Nita ZahriNo ratings yet
- Alcohol Related Liver Disease Brochure 2017Document16 pagesAlcohol Related Liver Disease Brochure 2017DarkangelcaliNo ratings yet
- ChesttubesDocument30 pagesChesttubesapi-2692977900% (1)
- Liang Zhao, PHD, Ping Ji, PHD, Zhihong Li, PHD, Partha Roy, PHD, and Chandrahas G. Sahajwalla, PHDDocument12 pagesLiang Zhao, PHD, Ping Ji, PHD, Zhihong Li, PHD, Partha Roy, PHD, and Chandrahas G. Sahajwalla, PHDTharanga Devinda JayathungaNo ratings yet
- Blood PhysiologyDocument11 pagesBlood PhysiologyDrSherwan Rahman Shal100% (6)
- Amyotrophic Lateral Sclerosis: PathophysiologyDocument4 pagesAmyotrophic Lateral Sclerosis: PathophysiologyJulia SalvioNo ratings yet
- 0092015020Document9 pages0092015020ChloéNo ratings yet
- Aquanet LG100 MSDS 21.5.2012Document5 pagesAquanet LG100 MSDS 21.5.2012Alejandra Paz San MartínNo ratings yet
- 2023 10 18 Sanction ADRV ENG 2.0Document3 pages2023 10 18 Sanction ADRV ENG 2.0salvadorNo ratings yet
- Daftar Obat Puskesmas KanjiloDocument2 pagesDaftar Obat Puskesmas KanjiloAhmad SalimNo ratings yet
- Glaucoma Case StudyDocument5 pagesGlaucoma Case StudyEdgel QuidolesNo ratings yet
- Duncan Et Al-2018-Cochrane Database of Systematic ReviewsDocument150 pagesDuncan Et Al-2018-Cochrane Database of Systematic Reviewsluis.fe.gd84No ratings yet
- Inattentive Signs and Symptoms of ADD/ADHDDocument8 pagesInattentive Signs and Symptoms of ADD/ADHDmaryNo ratings yet
- PGP (P-Glycoprotein)Document8 pagesPGP (P-Glycoprotein)Anonymous kjh9P2qNo ratings yet
- Kristen Bentley Technical Writing 345 Dr. JamesDocument4 pagesKristen Bentley Technical Writing 345 Dr. Jamesapi-26011176No ratings yet
- 3 Retrorectal Myxoid Fibrosarcoma A New Entity 1584 9341 11 1 9Document2 pages3 Retrorectal Myxoid Fibrosarcoma A New Entity 1584 9341 11 1 9EstuNo ratings yet
- Pre Employment Medical Declaration Form - 2022Document2 pagesPre Employment Medical Declaration Form - 2022Neel GhoshNo ratings yet
- Ilizarov Ankle ArthrodesisDocument17 pagesIlizarov Ankle ArthrodesisasioquaNo ratings yet