Download as pptx, pdf, or txt
You might also like
- Nursing Care Plan Diabetes Mellitus Type 2Document2 pagesNursing Care Plan Diabetes Mellitus Type 2deric88% (76)
- The Preppers Medical Handbook by William ForgeyDocument321 pagesThe Preppers Medical Handbook by William ForgeyAtiwat Tre100% (9)
- Heart BlockDocument26 pagesHeart BlockMihir Patel88% (8)
- ECG Rhythm Strip Interpretation Lesson 4Document5 pagesECG Rhythm Strip Interpretation Lesson 4phoebjaetanNo ratings yet
- Atrial ExtrasystoleDocument11 pagesAtrial ExtrasystoleRaiganNo ratings yet
- Heartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaDocument31 pagesHeartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaNinaNo ratings yet
- Atrial Fibrilation GauDocument39 pagesAtrial Fibrilation GauRANA MOHAMMED HAMOOD AL-HADEQNo ratings yet
- Department of Propaedeutics of Internal Diseases: Kursk State Medical UniversityDocument88 pagesDepartment of Propaedeutics of Internal Diseases: Kursk State Medical UniversityHendraDarmawanNo ratings yet
- Epidemiology: Arrhythmia/DysrhythmiaDocument6 pagesEpidemiology: Arrhythmia/DysrhythmiashaitabliganNo ratings yet
- Arrhythmia OF THE HEARTDocument4 pagesArrhythmia OF THE HEARTSellappan MuthusamyNo ratings yet
- Cardiac Emergencies Cne DelhiDocument109 pagesCardiac Emergencies Cne DelhiManisha Thakur100% (1)
- Cardiac Dysrhythmias: Mrs. D. Melba Sahaya Sweety M.SC Nursing GimsarDocument60 pagesCardiac Dysrhythmias: Mrs. D. Melba Sahaya Sweety M.SC Nursing GimsarD. Melba S.S Chinna100% (1)
- What Causes Arrhythmias? What'S Its Cure: John Jero 11-DDocument23 pagesWhat Causes Arrhythmias? What'S Its Cure: John Jero 11-DJeroNo ratings yet
- Arrhythmias Dr. VishvasDocument20 pagesArrhythmias Dr. VishvasvishvasNo ratings yet
- Dysrhythmias: Normal Electrical ActivityDocument32 pagesDysrhythmias: Normal Electrical ActivityLarisse de LeonNo ratings yet
- What Is An Abnormal Heart RhythmDocument23 pagesWhat Is An Abnormal Heart Rhythmanon_287871141No ratings yet
- Cardiac ArrhythmiasDocument11 pagesCardiac ArrhythmiasChino Paolo SamsonNo ratings yet
- 12 - Cardiac Arrhythmias - 0Document12 pages12 - Cardiac Arrhythmias - 0Ehtiram HuseynovNo ratings yet
- Arrhythmia: PalpitationDocument36 pagesArrhythmia: PalpitationHala BahaaNo ratings yet
- Investigatory ProjectDocument26 pagesInvestigatory ProjectJeroNo ratings yet
- Arrhythmia FinalDocument36 pagesArrhythmia FinalBEA RADANo ratings yet
- Peri Operative Arryhthmias: Dr. Juzny Alkatiri, SPPD, SPJPDocument102 pagesPeri Operative Arryhthmias: Dr. Juzny Alkatiri, SPPD, SPJPAstari Pratiwi NuhrintamaNo ratings yet
- Esraa Abd Elnasser HassanDocument10 pagesEsraa Abd Elnasser HassanEsraa Abd ElnasserNo ratings yet
- ArrhythmiaDocument55 pagesArrhythmiaDonjeta AbaziNo ratings yet
- Sugiyono, S.Kep., Ners., M.KepDocument48 pagesSugiyono, S.Kep., Ners., M.KepHervin Ramadhani100% (1)
- Broadly DefinedDocument10 pagesBroadly DefinedJayvee AguilarNo ratings yet
- Cardiac DysrhythmiasDocument54 pagesCardiac DysrhythmiasClark LlameraNo ratings yet
- Approach To PalpitationsDocument74 pagesApproach To PalpitationsDarawan MirzaNo ratings yet
- Management Lethal ArrhythmiaDocument42 pagesManagement Lethal ArrhythmiaNovi CahyaNo ratings yet
- Cardiopulmonary ArrestDocument22 pagesCardiopulmonary ArrestEdi Saputra SNo ratings yet
- Medicine Lecture 17,18Document51 pagesMedicine Lecture 17,18Nayela AkramNo ratings yet
- Campugan - Jay - Patho - AssignmentDocument11 pagesCampugan - Jay - Patho - AssignmentFlower Flower FlowerNo ratings yet
- Cardiac ArrythmiaDocument16 pagesCardiac ArrythmiaHossen AliNo ratings yet
- Ngaji Arrythmia Cordis 3Document122 pagesNgaji Arrythmia Cordis 3Dhita Dwi NandaNo ratings yet
- Atrial FibrillationDocument19 pagesAtrial FibrillationAnwari MuhammadNo ratings yet
- Arrhythmia (Irregular Heartbeats) Symptoms, Types, and TreatmentDocument5 pagesArrhythmia (Irregular Heartbeats) Symptoms, Types, and TreatmentCyberMeow100% (1)
- 12 - Cardiac ArrhythmiasDocument12 pages12 - Cardiac ArrhythmiasYassine LaiymaniNo ratings yet
- Cardiac DysrhythmiaDocument5 pagesCardiac Dysrhythmiahoney_eytNo ratings yet
- Arrhythmias: Anurag Patidar Lecturer, Con, DMCHDocument40 pagesArrhythmias: Anurag Patidar Lecturer, Con, DMCHpreet kaurNo ratings yet
- Int9 ArrhythemiaDocument21 pagesInt9 ArrhythemiaOsama AlhumisiNo ratings yet
- Electrical System of The HeartDocument4 pagesElectrical System of The HeartEldhaNo ratings yet
- Cardiac Arrhythmias Guide - Causes, Symptoms and Treatment OptionsDocument5 pagesCardiac Arrhythmias Guide - Causes, Symptoms and Treatment OptionsaksinuNo ratings yet
- DR Mohamed A. Fathi Cardiology Specialist and Tutor GMCHRCDocument76 pagesDR Mohamed A. Fathi Cardiology Specialist and Tutor GMCHRCMohamed Ahmed FathiNo ratings yet
- CARDIOVASCULAR SYSTEM Assignment 1bDocument9 pagesCARDIOVASCULAR SYSTEM Assignment 1bDayasoruban SanmugamNo ratings yet
- Cardiac DysrythmiasDocument190 pagesCardiac DysrythmiasKoRnflakes100% (4)
- 20 Blok 15 Tahun 2015 SVT DysrrhytmiasDocument69 pages20 Blok 15 Tahun 2015 SVT Dysrrhytmiaswarriordc1995No ratings yet
- 5-Approach To PalpitationsDocument103 pages5-Approach To PalpitationsEverythingNo ratings yet
- DysrhythmiaDocument84 pagesDysrhythmiasuganthi rajesh kannaNo ratings yet
- 16cardiac Arrhythmias Part 1Document12 pages16cardiac Arrhythmias Part 1Jaydave PatelNo ratings yet
- ArrthymiasDocument11 pagesArrthymiasSyafiq AbeNo ratings yet
- Cvs PathoDocument36 pagesCvs PathoISRAELNo ratings yet
- 4a. Types of ArrhythmiasDocument11 pages4a. Types of Arrhythmiasessa sunnaNo ratings yet
- Conductive Disturbances: Rhythm vs. Conduction - Your Heart's Rhythm Is Its Pace or BeatDocument3 pagesConductive Disturbances: Rhythm vs. Conduction - Your Heart's Rhythm Is Its Pace or BeatSoleNo ratings yet
- ArrhythmiaDocument31 pagesArrhythmiaAbdallah Essam Al-ZireeniNo ratings yet
- Supplementary Material 4.3 Cardiac Rhythm Disorders-2Document14 pagesSupplementary Material 4.3 Cardiac Rhythm Disorders-2Andrea Love PalomoNo ratings yet
- Guia ArritmiasDocument13 pagesGuia ArritmiasPaolaNo ratings yet
- Atrial Fibrillation 1Document15 pagesAtrial Fibrillation 1api-595122187No ratings yet
- Dental Management of The Patient With Cardiac Arrhythmias: An UpdateDocument5 pagesDental Management of The Patient With Cardiac Arrhythmias: An UpdateDiego Zúñiga de LeónNo ratings yet
- Atrial FibrillationDocument2 pagesAtrial FibrillationsrimatsimhasaneshwarNo ratings yet
- 8C - Antiarrythmic DrugsDocument76 pages8C - Antiarrythmic DrugsShahpoor Ahmad ShirzadaNo ratings yet
- Abnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAbnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Unless Otherwise Noted, The Content of This Course Material Is Licensed Under A Creative Commons 3.0 LicenseDocument48 pagesUnless Otherwise Noted, The Content of This Course Material Is Licensed Under A Creative Commons 3.0 LicenseAmra ahmedNo ratings yet
- Section 9 Anti Parkinsonism MedicinesDocument14 pagesSection 9 Anti Parkinsonism MedicinesAmra ahmedNo ratings yet
- How To Make Simple Solutions and DilutionsDocument12 pagesHow To Make Simple Solutions and DilutionsAmra ahmedNo ratings yet
- Basic and Clinical Biostatisticts, by Beth D. Sanders, Robart G. TrappDocument2 pagesBasic and Clinical Biostatisticts, by Beth D. Sanders, Robart G. TrappAmra ahmedNo ratings yet
- Introduction Applied PharmacognosyDocument11 pagesIntroduction Applied PharmacognosyAmra ahmed100% (1)
- Anti Ulcer 2Document55 pagesAnti Ulcer 2Amra ahmedNo ratings yet
- SpondilodiscitisDocument4 pagesSpondilodiscitisMihnea VulpeNo ratings yet
- Amenore: Pembimbing: Dr. Putri Sekar W, Spog (K)Document56 pagesAmenore: Pembimbing: Dr. Putri Sekar W, Spog (K)Mc Robert JrNo ratings yet
- Case Study: Medical Colleges of Northern PhilippinesDocument16 pagesCase Study: Medical Colleges of Northern Philippinesmark OrpillaNo ratings yet
- Ecgs Made Easy 5th Edition Aehlert Test BankDocument14 pagesEcgs Made Easy 5th Edition Aehlert Test BankQuinn50% (2)
- WHO 2009 Dengue ClassificationDocument31 pagesWHO 2009 Dengue ClassificationGarata DwiNo ratings yet
- West Visayas State University COLLEGE of NURSING La Paz, IloiloDocument2 pagesWest Visayas State University COLLEGE of NURSING La Paz, IloilopircanoNo ratings yet
- NCP Nephrotic SyndromeDocument2 pagesNCP Nephrotic SyndromeReyzzhor50% (4)
- RCCM 202109-2166ocDocument10 pagesRCCM 202109-2166ocjoelsonNo ratings yet
- (Week 10) Epidemiology and Disease TransmissionDocument1 page(Week 10) Epidemiology and Disease TransmissionDiana Leen Dela CruzNo ratings yet
- Radiology ReportDocument4 pagesRadiology ReportMayNo ratings yet
- Drug Study - Calcium GluconateDocument1 pageDrug Study - Calcium GluconatemikErlhNo ratings yet
- LevodopaDocument3 pagesLevodopaderic50% (2)
- Nexus ConnectionsDocument2 pagesNexus ConnectionsBarry RoginskiNo ratings yet
- LUMBERPUNCTURDocument14 pagesLUMBERPUNCTURRahul VasavaNo ratings yet
- Chromosome Abnormalities Flash CardsDocument3 pagesChromosome Abnormalities Flash CardsAmirreza ReyNo ratings yet
- Interview Guide For Nursing Health HistoryDocument3 pagesInterview Guide For Nursing Health HistoryDersly LaneNo ratings yet
- ChildDocument17 pagesChildReyna Glorian HilarioNo ratings yet
- Thyroid SwellingDocument8 pagesThyroid SwellingDn Ezrinah Dn Esham50% (2)
- The Spanish Flu Pandemic of 1918Document5 pagesThe Spanish Flu Pandemic of 1918jellNo ratings yet
- CH 13 Burtons Diagnosing Infectious DiseasesDocument17 pagesCH 13 Burtons Diagnosing Infectious DiseasesedemcantosumjiNo ratings yet
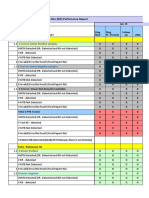
- GeneXpert - Monthly - Report - JAN, FEB, MARCH 2019 (GIMS) GAMBAT)Document12 pagesGeneXpert - Monthly - Report - JAN, FEB, MARCH 2019 (GIMS) GAMBAT)shakeelNo ratings yet
- COVID-19 Response Plan: Guidance Manual For A Public Health Community ResponseDocument12 pagesCOVID-19 Response Plan: Guidance Manual For A Public Health Community ResponseErin Richey KSDK0% (1)
- Nursing Care Plan Impaired Skin IntegrityDocument2 pagesNursing Care Plan Impaired Skin Integritycuicuita100% (3)
- Hypoxia: Lori HolmesDocument5 pagesHypoxia: Lori HolmesDanson Githinji ENo ratings yet
- Anemia in PregnancyDocument18 pagesAnemia in Pregnancysaagiba100% (1)
- PyelonephritisDocument24 pagesPyelonephritisfatihahannisahumairaNo ratings yet
- Laparoscopic Cholecystectomy 8-12 - tcm75-618838Document4 pagesLaparoscopic Cholecystectomy 8-12 - tcm75-618838zaid maythamNo ratings yet
- Satellite Images Baidu COVID19 Manuscript PreprintDocument10 pagesSatellite Images Baidu COVID19 Manuscript PreprintEconomy 365No ratings yet