Download as pptx, pdf, or txt
You might also like
- Primal Hormones Made by Aesthetic Primal 1Document59 pagesPrimal Hormones Made by Aesthetic Primal 1enzopark776No ratings yet
- KLM Anatomy Mcqs AnsweredDocument33 pagesKLM Anatomy Mcqs AnsweredJohanna Haludilu100% (3)
- Physiology of The Lateral Decubitus Position and One-Lung VentilationDocument31 pagesPhysiology of The Lateral Decubitus Position and One-Lung VentilationDebasis Sahoo100% (1)
- Tactical AthleteDocument135 pagesTactical AthleteEddy Muñoz100% (3)
- Lange Radiology of The Chest DiseasesDocument362 pagesLange Radiology of The Chest DiseasesAlexandra Nica100% (1)
- Ugrad Chest PreviewDocument39 pagesUgrad Chest PreviewKay BristolNo ratings yet
- Guide To STPM PracticalsDocument21 pagesGuide To STPM PracticalsMeng Fong100% (1)
- Physiology of Respiratry SymptomsDocument32 pagesPhysiology of Respiratry SymptomsMaryam MustafaNo ratings yet
- Physiology of Body PositioningDocument95 pagesPhysiology of Body Positioningtanya dattNo ratings yet
- Respiratory Phsysiology 2nd Edition - A - Answers To Self-Study ProbDocument6 pagesRespiratory Phsysiology 2nd Edition - A - Answers To Self-Study ProbRonny Araya AbarcaNo ratings yet
- Restrictive Lung DisordersDocument5 pagesRestrictive Lung DisordersSonali RajputNo ratings yet
- BPOC TraducereDocument2 pagesBPOC TraducereMunteanu DragosNo ratings yet
- Anaesthetic Concern For One Lung Ventilation: By-Dr - Bhushan Kinge, M.D. Ims - Bhu, VaranasiDocument57 pagesAnaesthetic Concern For One Lung Ventilation: By-Dr - Bhushan Kinge, M.D. Ims - Bhu, VaranasifaisalnaseemkhanNo ratings yet
- Mechanical Ventilation - Chapter 1Document8 pagesMechanical Ventilation - Chapter 1Raninda JuliantiNo ratings yet
- Prone Ventilation For Adult Patients With Acute Respiratory Distress Syndrome - UpToDateDocument19 pagesProne Ventilation For Adult Patients With Acute Respiratory Distress Syndrome - UpToDateHafiz Hari NugrahaNo ratings yet
- AtelectasisDocument28 pagesAtelectasisShikha Acharya100% (1)
- 1.P Fetal, NeonatalDocument2 pages1.P Fetal, NeonatalWisnu Agung WiyanggaNo ratings yet
- What S New in Respiratory PhysiologyDocument5 pagesWhat S New in Respiratory PhysiologyDaniel Gaete OsorioNo ratings yet
- Pathophysiology of CopdDocument62 pagesPathophysiology of CopddrhrshitjainNo ratings yet
- Lung Mechanics in Disease: Claude Guérin, Antonia Koutsoukou, Joseph Milic-Emili, and Edgardo D'AngeloDocument11 pagesLung Mechanics in Disease: Claude Guérin, Antonia Koutsoukou, Joseph Milic-Emili, and Edgardo D'AngeloOxigen XenonNo ratings yet
- Oxygenation and Airway Management: Quick LookDocument24 pagesOxygenation and Airway Management: Quick LookNining Komala SariNo ratings yet
- Mechanical VentilationDocument262 pagesMechanical VentilationShalini Garg0% (1)
- Adjustments of The Infant To Extrauterine LifeDocument11 pagesAdjustments of The Infant To Extrauterine LifeAntoine TimmermansNo ratings yet
- Dyamics of Respiration Composition VentilationDocument30 pagesDyamics of Respiration Composition VentilationUsama SajidNo ratings yet
- Ventilation of Obese PacientDocument4 pagesVentilation of Obese PacientAnaNo ratings yet
- SGD 9 - Respiratory 3Document7 pagesSGD 9 - Respiratory 3John RayNo ratings yet
- 2nd Year Respiratory Phys-252807Document17 pages2nd Year Respiratory Phys-252807Christopher WytherNo ratings yet
- Lecture Notes On Respiratory Physiology PDFDocument33 pagesLecture Notes On Respiratory Physiology PDFMiles HuiNo ratings yet
- Pulmonary Function TestsDocument35 pagesPulmonary Function TestsJawad MohammadNo ratings yet
- Home - Clinical - Management - News - Products - Protocols/Guidelines - Research - Buyer's Guide - Expert Insight - ArchivesDocument8 pagesHome - Clinical - Management - News - Products - Protocols/Guidelines - Research - Buyer's Guide - Expert Insight - ArchivesDuvvuri SankarNo ratings yet
- Respiratory Physiology: Dr. Okon MRCSDocument15 pagesRespiratory Physiology: Dr. Okon MRCSEdwin OkonNo ratings yet
- Pulmonary EdemaDocument5 pagesPulmonary EdemaMaris Angelica AyuyaoNo ratings yet
- TENSION PNEUMOTHORAX (Malav Shah)Document66 pagesTENSION PNEUMOTHORAX (Malav Shah)Sharath PsNo ratings yet
- Prone in ARDSDocument27 pagesProne in ARDSEmanuel VidalNo ratings yet
- Basic Principles of Mechanical Ventilation Andventilator GraphicsDocument70 pagesBasic Principles of Mechanical Ventilation Andventilator GraphicsSupriya PattnayakNo ratings yet
- Respiratory Failure Background: Other TestsDocument14 pagesRespiratory Failure Background: Other TestsRechell ValmoresNo ratings yet
- Ventilation-Perfusion - Ratio - Mismatch - TeachMePhysiologyDocument2 pagesVentilation-Perfusion - Ratio - Mismatch - TeachMePhysiologyrajnandinivermarvNo ratings yet
- Pulmonary Circulation: - The Blood Supply of The Lung Is Derived FromDocument52 pagesPulmonary Circulation: - The Blood Supply of The Lung Is Derived FromMoonAIRNo ratings yet
- Respiratory PhysiologyDocument68 pagesRespiratory PhysiologyDjNo ratings yet
- FInal Primary and Secundary (Recuperado Automaticamente)Document9 pagesFInal Primary and Secundary (Recuperado Automaticamente)João MonizNo ratings yet
- High Frequency Ventilation NeorevDocument16 pagesHigh Frequency Ventilation NeorevLuis Adolfo Gonzalez GomezNo ratings yet
- One Lung Ventilation PDFDocument79 pagesOne Lung Ventilation PDFAnnetNo ratings yet
- PK Flipped Lectures AnswersDocument12 pagesPK Flipped Lectures AnswersMusaddiqNo ratings yet
- Respiratory PhysiologyDocument42 pagesRespiratory PhysiologyvtnvmycdvgNo ratings yet
- Compliance and ResistanceDocument5 pagesCompliance and ResistanceNissie DegulacionNo ratings yet
- Ventilation Dead Space Ventilation Physiology of RespirationDocument55 pagesVentilation Dead Space Ventilation Physiology of RespirationkuhutansittinurhalizaNo ratings yet
- High-Frequency Oscillatory VentilationDocument63 pagesHigh-Frequency Oscillatory VentilationAnonymous G20oAbl6p8No ratings yet
- Thoracic Anatomy & Physiology A Simple Review: Mark Welliver CRNA, MS Assistant ProfessorDocument70 pagesThoracic Anatomy & Physiology A Simple Review: Mark Welliver CRNA, MS Assistant ProfessorRonnie JaderNo ratings yet
- Respiratoryfunctionandimportancetoanesthesia Final 140103050711 Phpapp02Document62 pagesRespiratoryfunctionandimportancetoanesthesia Final 140103050711 Phpapp02rijjorajooNo ratings yet
- Respiratory and Renal ReviewDocument39 pagesRespiratory and Renal ReviewTony PadNo ratings yet
- Ventilation Perfusion Ratio (Sachin Shah - 77)Document9 pagesVentilation Perfusion Ratio (Sachin Shah - 77)PrajwalNo ratings yet
- Shams FM02 FM2X Pulmonary Gas Exchange and Circulation 18 SummerDocument13 pagesShams FM02 FM2X Pulmonary Gas Exchange and Circulation 18 SummerFlowerNo ratings yet
- Curvas Interpretacion Clinica 4Document9 pagesCurvas Interpretacion Clinica 4Patty MArivel ReinosoNo ratings yet
- Ventilasi PerfusiDocument44 pagesVentilasi PerfusiIdahrachman515100% (1)
- Lung Hyperinflation in COPD: Applying Physiology To Clinical PracticeDocument12 pagesLung Hyperinflation in COPD: Applying Physiology To Clinical PracticeJaya Semara PutraNo ratings yet
- Pinsky1997 Article TheHemodynamicConsequencesOfMeDocument11 pagesPinsky1997 Article TheHemodynamicConsequencesOfMeAlvaro EstupiñánNo ratings yet
- Pulmonary Mumbo Jumbo - MartinezDocument12 pagesPulmonary Mumbo Jumbo - MartinezMartinez_DONo ratings yet
- One Lung VentilationDocument38 pagesOne Lung VentilationVarun Reddy V100% (1)
- Pulmonary PhysioDocument52 pagesPulmonary PhysiodjokerNo ratings yet
- Efectele Anestesiei Pe Funcționarea LungăDocument2 pagesEfectele Anestesiei Pe Funcționarea LungăAurelia AlexandraNo ratings yet
- Jet VentilationDocument2 pagesJet VentilationMarina BotrasNo ratings yet
- Ani̇mal Respiratory System PhysiologyDocument18 pagesAni̇mal Respiratory System PhysiologyNajafova SuadaNo ratings yet
- Pulmonary Function Tests in Clinical PracticeFrom EverandPulmonary Function Tests in Clinical PracticeAli AltalagRating: 5 out of 5 stars5/5 (1)
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- I STATDocument24 pagesI STATPraveen RamasamyNo ratings yet
- Neonatal Resuscitation: Presented By: Dr. Harish Uppala Chairperson: Dr. Kousalya Moderator: Dr. HemnathDocument23 pagesNeonatal Resuscitation: Presented By: Dr. Harish Uppala Chairperson: Dr. Kousalya Moderator: Dr. HemnathPraveen RamasamyNo ratings yet
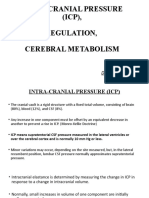
- Intra-Cranial Pressure (ICP), Regulation, Cerebral MetabolismDocument18 pagesIntra-Cranial Pressure (ICP), Regulation, Cerebral MetabolismPraveen RamasamyNo ratings yet
- Antifibrinolytic Therapy For Y2K+1: Ray Tople, M.D. Anesthesia and Operative Service BamcDocument34 pagesAntifibrinolytic Therapy For Y2K+1: Ray Tople, M.D. Anesthesia and Operative Service BamcPraveen RamasamyNo ratings yet
- Antifibrinolytic Therapy For Y2K+1: Ray Tople, M.D. Anesthesia and Operative Service BamcDocument34 pagesAntifibrinolytic Therapy For Y2K+1: Ray Tople, M.D. Anesthesia and Operative Service BamcPraveen RamasamyNo ratings yet
- Aortic StenosisDocument19 pagesAortic StenosisPraveen RamasamyNo ratings yet
- Neuraxial Analgesia & Anticoagulation: Charles E Smith MDDocument53 pagesNeuraxial Analgesia & Anticoagulation: Charles E Smith MDPraveen RamasamyNo ratings yet
- Antico Agne Ur AxialDocument27 pagesAntico Agne Ur AxialPraveen RamasamyNo ratings yet
- Anesthesia For Neurosurg2Document42 pagesAnesthesia For Neurosurg2Praveen RamasamyNo ratings yet
- Anaesthetic Challenges in Complex Maxillofacial Trauma - ADocument18 pagesAnaesthetic Challenges in Complex Maxillofacial Trauma - APraveen RamasamyNo ratings yet
- Anaesthesia in Obese PatientsDocument72 pagesAnaesthesia in Obese PatientsPraveen RamasamyNo ratings yet
- Anaesthesia For Thyroid SurgeryDocument19 pagesAnaesthesia For Thyroid SurgeryPraveen Ramasamy0% (1)
- Deep Breathing ExercisesDocument17 pagesDeep Breathing ExercisesPamela Warner100% (1)
- Kinesio Study Diaphragm TapingDocument2 pagesKinesio Study Diaphragm TapingJoao CunhaNo ratings yet
- Health AssessmentDocument51 pagesHealth AssessmentJared Dela cruzNo ratings yet
- Beatrice Unsworth On Breathing Exercises For Singers - Music - The ObserverDocument3 pagesBeatrice Unsworth On Breathing Exercises For Singers - Music - The ObserverAdrian De VilliersNo ratings yet
- BandhasDocument23 pagesBandhasLalith SolankiNo ratings yet
- Nursing Care For A Client With Chest Trauma: Reported By: Jazon, Gabriel Liberon PDocument100 pagesNursing Care For A Client With Chest Trauma: Reported By: Jazon, Gabriel Liberon PGabriel Liberon P. JazonNo ratings yet
- An Anatomical and Pathological Examination of The First Recorded Stranding of A Fraser's DolphinDocument7 pagesAn Anatomical and Pathological Examination of The First Recorded Stranding of A Fraser's DolphinStephanie Aeriel OcampoNo ratings yet
- VickeryR PDFDocument145 pagesVickeryR PDFOtrovanjeNo ratings yet
- Gut Tube and Body CavitiesDocument22 pagesGut Tube and Body CavitiesKeysha YbanezNo ratings yet
- Respiration Lecture NotesDocument7 pagesRespiration Lecture Notesamrutha mohandasNo ratings yet
- Jurnal Radiologi AtelektasisDocument14 pagesJurnal Radiologi AtelektasisferisiswonoNo ratings yet
- WHO Manual For Diagnostic Imaging Radiographic Anatomy and Interpretation of The Chest and The Pulmonary System (2002) PDFDocument147 pagesWHO Manual For Diagnostic Imaging Radiographic Anatomy and Interpretation of The Chest and The Pulmonary System (2002) PDFAloysius Anangga HNo ratings yet
- Belt Your Face Off!: A How-To Starter Guide For Broadway Belt SingingDocument23 pagesBelt Your Face Off!: A How-To Starter Guide For Broadway Belt SingingAlinutza Alina100% (2)
- GR 6 NAT REVIEWERDocument17 pagesGR 6 NAT REVIEWERmarife gupaalNo ratings yet
- Vocal AnatomyDocument8 pagesVocal AnatomyfunktotumNo ratings yet
- OSTEOPATIA EXPERIENCIA Anna Sheraton 2017Document7 pagesOSTEOPATIA EXPERIENCIA Anna Sheraton 2017ManuelGarciaMouriñoNo ratings yet
- Thoracic Sympathetic Trunk: Dr. Manuni PatelDocument20 pagesThoracic Sympathetic Trunk: Dr. Manuni PatelVinus VaghelaNo ratings yet
- Pleura: (1) Parietal Pleura (Parietal Layer)Document10 pagesPleura: (1) Parietal Pleura (Parietal Layer)Shimmering MoonNo ratings yet
- Respiratory System of Frog: External RespirationDocument3 pagesRespiratory System of Frog: External RespirationShaira CogollodoNo ratings yet
- Coping Strategies For TeachersDocument25 pagesCoping Strategies For TeachersSimplicius100% (1)
- Rat Dissection Guide: Including Pregnant FemaleDocument16 pagesRat Dissection Guide: Including Pregnant FemaleMAVIE GOMEZNo ratings yet
- Lesson 3 - Respiratory SystemDocument6 pagesLesson 3 - Respiratory SystemlarraNo ratings yet
- HIATAL HERNIA PPT Final PDFDocument49 pagesHIATAL HERNIA PPT Final PDFregysujit60% (5)
- Congenital Diaphragmatic HerniaDocument48 pagesCongenital Diaphragmatic HerniaShahd IdaisNo ratings yet