Download as pptx, pdf, or txt
You might also like
- Cusack Protocol .. Supplement Dosages Information Chart. Word PDFDocument2 pagesCusack Protocol .. Supplement Dosages Information Chart. Word PDFNaomy DC100% (6)
- The Human Circulatory System: Grade 9 - Sussex - Wennappuwa - ScienceDocument23 pagesThe Human Circulatory System: Grade 9 - Sussex - Wennappuwa - ScienceSwarnapaliliyanageNo ratings yet
- Diabetic Ketoacidosis Hypoglycemia: DR MD Mamunul Abedin ShimulDocument18 pagesDiabetic Ketoacidosis Hypoglycemia: DR MD Mamunul Abedin ShimulDr. Mamunul AbedinNo ratings yet
- SepsisDocument19 pagesSepsisapi-308355800No ratings yet
- LeptospirosisDocument9 pagesLeptospirosisDeepu VijayaBhanuNo ratings yet
- Case Study - Congestive Heart FailureDocument71 pagesCase Study - Congestive Heart FailureFrancis Adrian100% (3)
- Jack Westin MCAT Content BiologyDocument183 pagesJack Westin MCAT Content BiologyLoraNo ratings yet
- Assessment of bleeding Shock in a Politraumatized PatientFrom EverandAssessment of bleeding Shock in a Politraumatized PatientNo ratings yet
- Hyperosmolar Hyperglycemic StateDocument8 pagesHyperosmolar Hyperglycemic StateEsra AljafferNo ratings yet
- Hypertensive Emergencies (ESC 2019)Document10 pagesHypertensive Emergencies (ESC 2019)Glen LazarusNo ratings yet
- Sedation in ICUDocument14 pagesSedation in ICUIhtesham Ul Haq100% (1)
- Cost EffectivenessDocument22 pagesCost EffectivenessEdalyn CapiliNo ratings yet
- B U F N & H S N: Advanced Medical Surgical NURS 337 " Emergency Department Report "Document16 pagesB U F N & H S N: Advanced Medical Surgical NURS 337 " Emergency Department Report "Yousef JafarNo ratings yet
- SGLT2i Beyond Glycemic ControlDocument55 pagesSGLT2i Beyond Glycemic ControlSwapnaNo ratings yet
- DKA Canadian ProtocolDocument2 pagesDKA Canadian Protocolplay_wright2084No ratings yet
- Nursing Management: Nursing Management: Acute Kidney Injury and Chronic Kidney DiseaseDocument22 pagesNursing Management: Nursing Management: Acute Kidney Injury and Chronic Kidney Diseasedian rachmat saputroNo ratings yet
- DKA and HHSDocument16 pagesDKA and HHSGepengCungkringNo ratings yet
- Hyperosmolar Hyperglycemic Nonketotic Syndrome HHNSDocument12 pagesHyperosmolar Hyperglycemic Nonketotic Syndrome HHNSKyle Ü D. CunanersNo ratings yet
- Hyperosmolar Hyperglycemic State (HHS)Document21 pagesHyperosmolar Hyperglycemic State (HHS)Malueth AnguiNo ratings yet
- Dka GuidelineDocument16 pagesDka GuidelineGhada HusseinNo ratings yet
- Dka and HHSDocument25 pagesDka and HHSMouhammad Dawoud100% (2)
- CH 46 Complications of AnaesthesiaDocument29 pagesCH 46 Complications of AnaesthesiaChristian LeepoNo ratings yet
- Myxedema ComaDocument14 pagesMyxedema Comabc3bhat6206No ratings yet
- DKA Draft 1 AM - Drawio 2Document1 pageDKA Draft 1 AM - Drawio 2Dud AccNo ratings yet
- EMTDocument73 pagesEMTLovely Acabado TampocoNo ratings yet
- Dr. Surya Abadi KristyoadiDocument42 pagesDr. Surya Abadi KristyoadiDr. Surya Abadi KristyoadiNo ratings yet
- Adrenaline (Epinephrine) : InotropesDocument4 pagesAdrenaline (Epinephrine) : Inotropespachino007No ratings yet
- Blunt Trauma AbdomenDocument41 pagesBlunt Trauma AbdomenSanthanu SukumaranNo ratings yet
- Orientation Booklet For Emergency DepartmentDocument10 pagesOrientation Booklet For Emergency Departmentshahidchaudhary100% (1)
- Cardiac TestsDocument17 pagesCardiac TestsGiorgiana pNo ratings yet
- Midazolam FinalDocument2 pagesMidazolam FinalAhmad AbqariNo ratings yet
- NURSING Review Session (Nur 220) Part 1Document8 pagesNURSING Review Session (Nur 220) Part 1Mariel EstoniloNo ratings yet
- Thyroid StormDocument23 pagesThyroid Stormtogi_siahaanNo ratings yet
- Posterior Cranial Fossa Anesthetic ManagementDocument48 pagesPosterior Cranial Fossa Anesthetic ManagementDivya Rekha KolliNo ratings yet
- Type 1 Diabetes: Diabetic Ketoacidos ISDocument16 pagesType 1 Diabetes: Diabetic Ketoacidos ISapi-551073862No ratings yet
- Approach To Septic ShockDocument16 pagesApproach To Septic ShockRaja EllysyaNo ratings yet
- Critical Care Environment - Design Stucture and FacilitiesDocument22 pagesCritical Care Environment - Design Stucture and FacilitiesProf. Ramsharan MehtaNo ratings yet
- Supraventricular TachycardiaDocument9 pagesSupraventricular TachycardiaclubsanatateNo ratings yet
- Endocrine Emergencies CompiledDocument102 pagesEndocrine Emergencies CompiledSubhkanish RavindraNo ratings yet
- Acute Stroke ManagementDocument8 pagesAcute Stroke ManagementГурам ЧахвадзеNo ratings yet
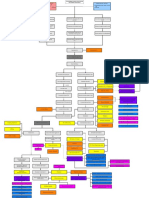
- Conceptual Map - Diabetic KetoacidosisDocument2 pagesConceptual Map - Diabetic KetoacidosisLovie Japhet LopezNo ratings yet
- Shock Power PointDocument24 pagesShock Power PointmarwaNo ratings yet
- Cad ....Document94 pagesCad ....AnanthibalaNo ratings yet
- Anterior Pituitary Gland: Fawwaz Ammari Laith & HaniDocument22 pagesAnterior Pituitary Gland: Fawwaz Ammari Laith & HaniRashed ShatnawiNo ratings yet
- Management of Diabetes Patients in SurgeryDocument28 pagesManagement of Diabetes Patients in Surgerylow_sernNo ratings yet
- Pulmonary EmbolismDocument16 pagesPulmonary EmbolismniyigokNo ratings yet
- Acute Liver FailureDocument3 pagesAcute Liver FailureElisabeth F. OjhaNo ratings yet
- TB MeningeDocument75 pagesTB MeningeAyen FornollesNo ratings yet
- ShockDocument24 pagesShockYaacub IbrahimNo ratings yet
- Pneumonia Management ProtocolDocument2 pagesPneumonia Management Protocolsky nuts100% (1)
- Sick Sinus Syndrome 1Document23 pagesSick Sinus Syndrome 1Salman HabeebNo ratings yet
- IsoprenalineDocument2 pagesIsoprenalineImmanuel Victor GeorgeNo ratings yet
- Acute Respiratory InfectionsDocument18 pagesAcute Respiratory InfectionsEmilyRose17No ratings yet
- Medical Evaluation of Surgical Patient 2015049Document39 pagesMedical Evaluation of Surgical Patient 2015049Kanneaufii KaramelNo ratings yet
- Traumatic Lesions: Head Injuries: Delano, Alexandra Julianne Duran, Fatima MedrizaDocument31 pagesTraumatic Lesions: Head Injuries: Delano, Alexandra Julianne Duran, Fatima MedrizaFatima Medriza Duran100% (1)
- Sedation in The ICU PulmCritDocument32 pagesSedation in The ICU PulmCritchadchimaNo ratings yet
- Nonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Document32 pagesNonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Saad MotawéaNo ratings yet
- Hypertensive CrisisDocument28 pagesHypertensive CrisisJacob Alexander MarpaungNo ratings yet
- Hypokalem Ia: Clarisse Cloie Lamberte - BSN3DDocument26 pagesHypokalem Ia: Clarisse Cloie Lamberte - BSN3DClarisse Cloie LamberteNo ratings yet
- SepsisDocument33 pagesSepsisv_vijayakanth7656No ratings yet
- Insulin, Oral Hypoglycaemic Agents, GlucagonDocument63 pagesInsulin, Oral Hypoglycaemic Agents, GlucagonBhavesh kunvarNo ratings yet
- Acute Kidney InjuryDocument34 pagesAcute Kidney Injury* mokhtar !!No ratings yet
- Cirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDocument21 pagesCirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDan ChicinasNo ratings yet
- A Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Abdominal Aortic Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Fracture Tibia & Fibula-1Document111 pagesFracture Tibia & Fibula-1Usaid SulaimanNo ratings yet
- Radiographic Anatomy of Gastrointestinal Tract: Dr. Kikomeko Sharif Department of Radiology Iuiu-Habib Medical SchoolDocument55 pagesRadiographic Anatomy of Gastrointestinal Tract: Dr. Kikomeko Sharif Department of Radiology Iuiu-Habib Medical SchoolUsaid SulaimanNo ratings yet
- TB SpineDocument18 pagesTB SpineUsaid SulaimanNo ratings yet
- Nutrition in The Surgical PatientDocument35 pagesNutrition in The Surgical PatientUsaid SulaimanNo ratings yet
- 4 Chest Imaging - Part 234Document63 pages4 Chest Imaging - Part 234Usaid SulaimanNo ratings yet
- Abdominal Imaging - Part 23Document74 pagesAbdominal Imaging - Part 23Usaid SulaimanNo ratings yet
- TB and Leprosy Case Management Desk Guide - 3rd Edition - 22!1!2019 - FINAL - SHAREDDocument78 pagesTB and Leprosy Case Management Desk Guide - 3rd Edition - 22!1!2019 - FINAL - SHAREDUsaid SulaimanNo ratings yet
- COVID-19: Current Understanding of Its Pathophysiology, Clinical Presentation and TreatmentDocument9 pagesCOVID-19: Current Understanding of Its Pathophysiology, Clinical Presentation and TreatmentUsaid SulaimanNo ratings yet
- Islamic University in Uganda: Name: Abdiqani Omar NoorDocument11 pagesIslamic University in Uganda: Name: Abdiqani Omar NoorUsaid SulaimanNo ratings yet
- BURNSDocument17 pagesBURNSUsaid SulaimanNo ratings yet
- Islamic University in Uganda: Habib Medical SchoolDocument8 pagesIslamic University in Uganda: Habib Medical SchoolUsaid SulaimanNo ratings yet
- Circulatory and Respiratory Systems - Module 3Document47 pagesCirculatory and Respiratory Systems - Module 3CaityNo ratings yet
- TerminDocument5 pagesTerminAnonymous DA8iQzNo ratings yet
- Mock ExamsDocument3 pagesMock ExamsRon DanyNo ratings yet
- WGA6-Ocular Blood Flow in GlaucomaDocument177 pagesWGA6-Ocular Blood Flow in Glaucomamdmmm100% (1)
- Neonatal Resuscitation ProgramDocument6 pagesNeonatal Resuscitation ProgramRick Frea100% (5)
- Pulmonary CirculationDocument36 pagesPulmonary CirculationSllavko K. KallfaNo ratings yet
- Confessions of A Celebrity PsychicDocument303 pagesConfessions of A Celebrity Psychicapi-19792901100% (2)
- Lesson 2Document26 pagesLesson 2Janielle FajardoNo ratings yet
- Acute and Chronic InflammationDocument52 pagesAcute and Chronic Inflammationjames20123100% (1)
- Circulatory System HandoutsDocument4 pagesCirculatory System HandoutsCzarae VillanuevaNo ratings yet
- Highlights2020 Essay eDocument7 pagesHighlights2020 Essay eS3MT-10 Fong Lok ChingNo ratings yet
- Morphopathology CS 2014-2015 469Document59 pagesMorphopathology CS 2014-2015 469Elena PavlicNo ratings yet
- Sample The Human Body Worksheets 1Document18 pagesSample The Human Body Worksheets 1Jan Erika AlmeronNo ratings yet
- Assessing The Thorax and LungsDocument4 pagesAssessing The Thorax and LungsLorenz Jude Cańete100% (2)
- Peran Perawat Dalam Manajemen Tim Akses Vaskular HD - Theresia M Toji Pio, RNDocument40 pagesPeran Perawat Dalam Manajemen Tim Akses Vaskular HD - Theresia M Toji Pio, RNjaybeat09No ratings yet
- Transport in AnimalsDocument43 pagesTransport in AnimalsEdwins MaranduNo ratings yet
- Healthy LivingDocument83 pagesHealthy LivingAnonymous KovGERSNo ratings yet
- Effect of Watermelon (Citrullus Lanatus) On Pulse Rate and Blood Pressure in Healthy IndividualsDocument4 pagesEffect of Watermelon (Citrullus Lanatus) On Pulse Rate and Blood Pressure in Healthy IndividualsAyu WidiartiNo ratings yet
- Interactive PDF The Circulatory System - Ver - 1Document2 pagesInteractive PDF The Circulatory System - Ver - 1Alyasin FrougaNo ratings yet
- Coke and Great Depression - The Big LieDocument13 pagesCoke and Great Depression - The Big LieN yatesNo ratings yet
- 3.4 Blood PressureDocument50 pages3.4 Blood Pressure091Nurul Nur AkmalNo ratings yet
- Regulation of Coronary Blood Flow PDFDocument330 pagesRegulation of Coronary Blood Flow PDFAlin-Octavian BorinaNo ratings yet
- Naturopathic Approaches For HypertensionDocument45 pagesNaturopathic Approaches For HypertensionMarissa CartyNo ratings yet
- Muscular System FunctionDocument2 pagesMuscular System FunctionLachlan PalmerNo ratings yet
- Physical and Psychological Changes in Older PersonDocument8 pagesPhysical and Psychological Changes in Older Personjanna mae patriarcaNo ratings yet
- Ganoderma Lucidum Ancient HerbDocument52 pagesGanoderma Lucidum Ancient HerbSARGURU SAI MEDIANo ratings yet