Download as pptx, pdf, or txt
You might also like
- Preclinical Anatomy Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Anatomy Review 2023: For USMLE Step 1 and COMLEX-USA Level 1Rating: 5 out of 5 stars5/5 (2)
- Module 6.9 TLEDocument115 pagesModule 6.9 TLEroseavy90% (10)
- Multiple Fetal Pregnancy: Riza SufriadiDocument20 pagesMultiple Fetal Pregnancy: Riza SufriadiRizur SufisonNo ratings yet
- Multiple Pregnancy 2008Document61 pagesMultiple Pregnancy 2008Dagnachew kasayeNo ratings yet
- A Case of - Twin Gestation With OneDocument31 pagesA Case of - Twin Gestation With OneMD Nazar ImamNo ratings yet
- Understanding Multiple Pregnancy: Maternal & Fetal ComplicationsDocument69 pagesUnderstanding Multiple Pregnancy: Maternal & Fetal Complications966342No ratings yet
- Twin TDocument30 pagesTwin TmaezuNo ratings yet
- Multiple PregnancyDocument55 pagesMultiple PregnancyNathaniel YeriNo ratings yet
- Wachemo University: M/H/S/C NemmhDocument52 pagesWachemo University: M/H/S/C NemmhDira DitaNo ratings yet
- Book ReportDocument69 pagesBook ReportBarangay MotibotNo ratings yet
- Multiple Pregnancy: Nirav Hitesh Kumar ValandDocument28 pagesMultiple Pregnancy: Nirav Hitesh Kumar ValandNirav SharmaNo ratings yet
- 10.multiple GestationDocument49 pages10.multiple GestationdenekeNo ratings yet
- Multiple PregnancyDocument52 pagesMultiple Pregnancyazida90100% (4)
- Cytogenetics FinalsDocument18 pagesCytogenetics FinalsPatrick AbellaNo ratings yet
- 4th Year Multiple PregnancyDocument57 pages4th Year Multiple PregnancyKingsley Calex100% (2)
- Multiple PregnanciesDocument36 pagesMultiple PregnanciesBasudev ch100% (1)
- Kehamilan Ganda1Document54 pagesKehamilan Ganda1rizmaNo ratings yet
- K-Medics Placental Previa - AbruptionDocument28 pagesK-Medics Placental Previa - AbruptionMichael AdjeiNo ratings yet
- Twin PregnancyDocument73 pagesTwin Pregnancykrishna mandalNo ratings yet
- First Trimester BleedingDocument93 pagesFirst Trimester BleedingScribdTranslationsNo ratings yet
- IUFD Repro21Document31 pagesIUFD Repro21DhianNo ratings yet
- Twin Pregnancy: Dr. Girishankar Samarasam Supervised By: DR Rathimalar DR Mohd Faizal Bin Nor AzmiDocument56 pagesTwin Pregnancy: Dr. Girishankar Samarasam Supervised By: DR Rathimalar DR Mohd Faizal Bin Nor AzmiShre RanjithamNo ratings yet
- Multifetal PregnancyDocument11 pagesMultifetal PregnancyDr. ZeekNo ratings yet
- Multifetal Pregnancy: Amr Nadim, MDDocument36 pagesMultifetal Pregnancy: Amr Nadim, MDsharenNo ratings yet
- PretermDocument28 pagesPretermhacker ammerNo ratings yet
- Abortion Chapter 18 Willobs 25th EdDocument40 pagesAbortion Chapter 18 Willobs 25th EdNabil MaulanaNo ratings yet
- Abruption PlacentaDocument40 pagesAbruption Placentamruts aregawiNo ratings yet
- Extreme Preterm Premature Rupture of Membranes: KSM Obstetri Dan Ginekologi Rumah Sakit Umum Pusat PersahabatanDocument27 pagesExtreme Preterm Premature Rupture of Membranes: KSM Obstetri Dan Ginekologi Rumah Sakit Umum Pusat Persahabatanrilla saeliputriNo ratings yet
- Multiple Pregnancy: Kevin AndrewDocument36 pagesMultiple Pregnancy: Kevin AndrewintanpurnNo ratings yet
- Genetic Disorder and Pediatric DiseasesDocument48 pagesGenetic Disorder and Pediatric DiseasesJohn LloydNo ratings yet
- Myoma of The UterusDocument22 pagesMyoma of The UterusSemon YohannesNo ratings yet
- Congenital AnomaliesDocument121 pagesCongenital AnomaliesIptisam SwalehNo ratings yet
- Multifetal PregnancyDocument68 pagesMultifetal PregnancyHoque Mohammed Newaz ShorifulNo ratings yet
- NCM 109 Abnormal Ob High Risk PregnancyDocument13 pagesNCM 109 Abnormal Ob High Risk PregnancyMatth N. ErejerNo ratings yet
- علاااءDocument21 pagesعلاااءalaazeez2000No ratings yet
- Abortion (Miscarrage)Document46 pagesAbortion (Miscarrage)escalatorNo ratings yet
- Abortion and Ectopic PregnancyDocument40 pagesAbortion and Ectopic PregnancyGebremichael RetaNo ratings yet
- Multifetal GestationDocument15 pagesMultifetal GestationAlloy Trixia BaguioNo ratings yet
- Uterine FibroidsDocument25 pagesUterine FibroidssyifasfNo ratings yet
- Placental Abruption: Liu Wei Department of Ob & Gy Ren Ji HospitalDocument15 pagesPlacental Abruption: Liu Wei Department of Ob & Gy Ren Ji HospitalTotaAl-mutairiNo ratings yet
- Methods of Human GeneticsDocument81 pagesMethods of Human Geneticsfae-ar_raziNo ratings yet
- Multifetal PregnancyDocument42 pagesMultifetal PregnancyRisman TangdiNo ratings yet
- OBSTETRIC 2017-2018 4 Assistant Professor: DR - Esraa AL-MainiDocument43 pagesOBSTETRIC 2017-2018 4 Assistant Professor: DR - Esraa AL-MainiBlacky ChyaNo ratings yet
- Multi Fetal Pregnancy & ComplicationsDocument20 pagesMulti Fetal Pregnancy & Complicationsapi-3705046No ratings yet
- Human Embryology: Professor of Anatomy and Embryology Faculty of Medicine Hamadan University of Medical SciencesDocument51 pagesHuman Embryology: Professor of Anatomy and Embryology Faculty of Medicine Hamadan University of Medical SciencesGaziza MaaroofNo ratings yet
- Abortion: Zhang Ming 张 铭Document51 pagesAbortion: Zhang Ming 张 铭api-19641337No ratings yet
- HemorrhagesDocument3 pagesHemorrhagesARAugustoNo ratings yet
- Week 11 Framework For Maternal and Child Health Nursing Focusing On at Risk High Risk and Sick ClientsDocument15 pagesWeek 11 Framework For Maternal and Child Health Nursing Focusing On at Risk High Risk and Sick Clientss.tabaquin.edwardjrNo ratings yet
- Abruptio Placenta and AbortionDocument10 pagesAbruptio Placenta and Abortiondanica grace gubaNo ratings yet
- 4.. ReproDocument61 pages4.. Reprosabin luitelNo ratings yet
- 54 Fetal Death of A Twin PDFDocument3 pages54 Fetal Death of A Twin PDFrajma2006No ratings yet
- OB (Midterms Reviewer)Document19 pagesOB (Midterms Reviewer)JULIANO, GRACHELLE A.No ratings yet
- D. High Risk PregnanciesDocument78 pagesD. High Risk PregnanciesKeziah TampusNo ratings yet
- FertilizationDocument108 pagesFertilizationDauda RukaiyaNo ratings yet
- AbortionDocument30 pagesAbortionKIYANo ratings yet
- Bleeding in Early PregnancyDocument34 pagesBleeding in Early Pregnancyنواف الجهنيNo ratings yet
- Abnormal Placentation Teaching Script JHUFinalDocument2 pagesAbnormal Placentation Teaching Script JHUFinalJILL ANGELESNo ratings yet
- 11-Ectopic PregnancyDocument35 pages11-Ectopic PregnancyDawit g/kidanNo ratings yet
- Characteristics of Pathologic Processes in Fetus, Newbons, Children of Various AgesDocument42 pagesCharacteristics of Pathologic Processes in Fetus, Newbons, Children of Various AgesChris QueiklinNo ratings yet
- Female Genital Tract Tumours Pathology Assignment #5Document5 pagesFemale Genital Tract Tumours Pathology Assignment #5aimy.palawataraNo ratings yet
- HypertensionDocument5 pagesHypertensionJonathan BreedveldNo ratings yet
- Instructor: Nguyen Hoang Khue Tu, PH.D, PharmDocument24 pagesInstructor: Nguyen Hoang Khue Tu, PH.D, PharmChaoswind_Ka_2673No ratings yet
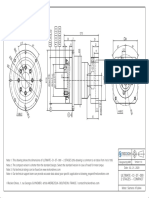
- ULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Document1 pageULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Francesco SchioppaNo ratings yet
- VedicReport6 10 20179 56 16PMDocument47 pagesVedicReport6 10 20179 56 16PManandpaithankar13No ratings yet
- XML and PHPDocument33 pagesXML and PHPsplokbovNo ratings yet
- Agrirobot PDFDocument103 pagesAgrirobot PDFMuhamad Azlan ShahNo ratings yet
- Chapter 10 - Eco LiteracyDocument15 pagesChapter 10 - Eco LiteracyMichelle Bandoquillo100% (1)
- 322 Dynamic Demographic Characteristic Slum Population in Nashik City With Special Reference From 2011Document6 pages322 Dynamic Demographic Characteristic Slum Population in Nashik City With Special Reference From 2011B-15 Keyur BhanushaliNo ratings yet
- Security ManagementDocument35 pagesSecurity ManagementVanessa CarreteNo ratings yet
- Methods-Time Measurement: MODAPTS Technique. This Technique Was Introduced in 1966 byDocument2 pagesMethods-Time Measurement: MODAPTS Technique. This Technique Was Introduced in 1966 byChisom IkengwuNo ratings yet
- Boiler WaterDocument70 pagesBoiler WaterDarius DsouzaNo ratings yet
- 1700 N Manhattan Ave - Royal Towers - Notice of CondemnationDocument14 pages1700 N Manhattan Ave - Royal Towers - Notice of CondemnationMatthew SelfNo ratings yet
- SKRAMDocument14 pagesSKRAMSebastián BoteroNo ratings yet
- West Elm Digital CatalogueDocument131 pagesWest Elm Digital CatalogueogkanishkNo ratings yet
- PunctuationsDocument5 pagesPunctuationsPrincess De VegaNo ratings yet
- Is 228 9 1989Document8 pagesIs 228 9 1989Andrewz PachuauNo ratings yet
- Money Laundering, Terrorism Financing in NigeriaDocument7 pagesMoney Laundering, Terrorism Financing in NigeriaThe Law Brigade (Journals) PublishersNo ratings yet
- Nigeria's Agenda 21 Draft Objectives and Strategies ForDocument77 pagesNigeria's Agenda 21 Draft Objectives and Strategies ForbenNo ratings yet
- Advanced Baking 1Document61 pagesAdvanced Baking 1Judelmae SisonNo ratings yet
- 6º Ano Ingles Unit4 Test3Document3 pages6º Ano Ingles Unit4 Test3Paula Lopes100% (1)
- Dyna SandDocument8 pagesDyna SandRuchi GuptaNo ratings yet
- Sunil Panda Commerce Classes: Before Exam Practice Questions For Term 2 Boards Accounts-Not For Profit OrganisationDocument3 pagesSunil Panda Commerce Classes: Before Exam Practice Questions For Term 2 Boards Accounts-Not For Profit OrganisationHigi SNo ratings yet
- JLTR, 02Document8 pagesJLTR, 02Junalyn Villegas FerbesNo ratings yet
- Actuator-Sensor-Interface: I/O Modules For Operation in The Control Cabinet (IP 20)Document22 pagesActuator-Sensor-Interface: I/O Modules For Operation in The Control Cabinet (IP 20)chochoroyNo ratings yet
- 19 8 English+Manual+Rt 3Document249 pages19 8 English+Manual+Rt 3aleba1975No ratings yet
- Spa Music 10 SLM3 q1Document21 pagesSpa Music 10 SLM3 q1Noldan King FranciscoNo ratings yet
- (20635303 - Journal of Behavioral Addictions) Fear of Missing Out (FoMO) and Internet Use - A Comprehensive Systematic Review and Meta-AnalysisDocument22 pages(20635303 - Journal of Behavioral Addictions) Fear of Missing Out (FoMO) and Internet Use - A Comprehensive Systematic Review and Meta-AnalysisNeeraj raiNo ratings yet
- National Simultaneous Earthquake and Fire DrillsDocument2 pagesNational Simultaneous Earthquake and Fire DrillsCatherine TamayoNo ratings yet
- Drug Chart 7 - Hee InternetDocument19 pagesDrug Chart 7 - Hee InternetAhmzzdNo ratings yet