Download as ppt, pdf, or txt
You might also like
- Psy 2300 Clinical Case 2 BDocument2 pagesPsy 2300 Clinical Case 2 BFaruse Ali0% (1)
- Malaysian Triage Category DraftDocument11 pagesMalaysian Triage Category DraftMUHAMMAD FAIZ BIN NASIR / HPUPM100% (1)
- ADVANCED LIFE SUPPORT Training Manual Final 2017Document85 pagesADVANCED LIFE SUPPORT Training Manual Final 2017Jeevan Velan94% (18)
- Essay Claim of Policy HIV AIDSDocument2 pagesEssay Claim of Policy HIV AIDSdiary_anteNo ratings yet
- RESEARCH GCS AdecDocument62 pagesRESEARCH GCS Adec07 FARAH ATHIRAH BINTI MOH FUZINo ratings yet
- Polytrauma, ABC of Trauma & Its ManagementDocument33 pagesPolytrauma, ABC of Trauma & Its ManagementMongolian MutuNo ratings yet
- Pre-Hospital Trauma CareDocument8 pagesPre-Hospital Trauma Carecorsaru100% (1)
- Malaysian Triage CategoryDocument3 pagesMalaysian Triage CategoryHafiz Hamidi71% (7)
- Needle Prick Injury Dalam Kalangan Jururawat Di Malaysia....................................................................................Document8 pagesNeedle Prick Injury Dalam Kalangan Jururawat Di Malaysia....................................................................................Rizal FarieNo ratings yet
- Managment of Trauma Patient in ERDocument46 pagesManagment of Trauma Patient in ERtofanNo ratings yet
- Cardiac Emergency - Cardiac Arrest Management (Ali Haedar)Document39 pagesCardiac Emergency - Cardiac Arrest Management (Ali Haedar)Aatroney MadureseNo ratings yet
- Vasopressor & InotropesDocument44 pagesVasopressor & InotropesArun KumarNo ratings yet
- Early Assessment of Trauma Patients and ATLSDocument45 pagesEarly Assessment of Trauma Patients and ATLSTILAHUNNo ratings yet
- Pre Hospital Care in Malaysia - Issues and ChallengesDocument50 pagesPre Hospital Care in Malaysia - Issues and Challengeschat5619100% (1)
- INOTROPIC SUPPORT (Autosaved)Document23 pagesINOTROPIC SUPPORT (Autosaved)Bindhu RaniNo ratings yet
- Mother: HealthDocument39 pagesMother: HealthPadma BhatiaNo ratings yet
- 1 Early Management of Trauma Patient in The HospitalDocument23 pages1 Early Management of Trauma Patient in The HospitalkgnmatinNo ratings yet
- Emergency AssessmentDocument27 pagesEmergency AssessmentJoanna RachelNo ratings yet
- JPP Prehospital Care MalaysiaDocument5 pagesJPP Prehospital Care MalaysiaNasibah Tuan YaacobNo ratings yet
- Immobilization ExtricationDocument75 pagesImmobilization ExtricationJohn Britto100% (3)
- Heart AttackDocument2 pagesHeart Attackmeylisa putri ayunandaNo ratings yet
- SOSD Phases of Fluid ResuscitationDocument8 pagesSOSD Phases of Fluid ResuscitationAvinash KumbharNo ratings yet
- HypoglycemiaDocument8 pagesHypoglycemianurizzah_885541No ratings yet
- Hypertension FinalDocument64 pagesHypertension FinalrameshbmcNo ratings yet
- Covid 19 Psychological Support: Department of Psychiatry, LLRM Medical College MeerutDocument23 pagesCovid 19 Psychological Support: Department of Psychiatry, LLRM Medical College MeerutNaina SharmaNo ratings yet
- Malaysian Triage CategoryDocument2 pagesMalaysian Triage CategoryArnold Daniel70% (10)
- Approach To HypertensionDocument16 pagesApproach To HypertensionShradha KhuranaNo ratings yet
- Cholinergic DrugsDocument11 pagesCholinergic Drugsshivanshpande100% (1)
- Triage ZoneDocument4 pagesTriage ZoneHafiz Hamidi100% (1)
- Polytrauma ManagementDocument70 pagesPolytrauma ManagementStar Cruise88% (8)
- Cardiac Emergencies Cne DelhiDocument109 pagesCardiac Emergencies Cne DelhiManisha Thakur100% (1)
- Endocrine Disorders Cont... (For ADRENAL GLAND)Document4 pagesEndocrine Disorders Cont... (For ADRENAL GLAND)Ernie G. Bautista II, RN, MD100% (3)
- FIRST AID by Dr. Qasim AhmedDocument80 pagesFIRST AID by Dr. Qasim AhmedFaheem KhanNo ratings yet
- Sharp InjuryDocument31 pagesSharp InjuryRamli Mohd NajibNo ratings yet
- ICU Bundles Dr-DohaDocument44 pagesICU Bundles Dr-DohaAhmed Mohammed Salama0% (1)
- AnemiaMukt Bharat I-NIPIDocument23 pagesAnemiaMukt Bharat I-NIPIMukunda MurariNo ratings yet
- Thoracic Injury Management Jan 08Document39 pagesThoracic Injury Management Jan 08Uday PrabhuNo ratings yet
- InsulinomaDocument18 pagesInsulinomaBetta BeTta0% (1)
- Myasthenia GravisDocument24 pagesMyasthenia GravisAliMalikNo ratings yet
- Scene Size UpDocument7 pagesScene Size UpChester QuilalaNo ratings yet
- Essentials of Anesthesia For Medical Students FinalDocument82 pagesEssentials of Anesthesia For Medical Students FinalEs LamNo ratings yet
- Chapter 1 - Central Venous CathetersDocument6 pagesChapter 1 - Central Venous CathetersParth PatelNo ratings yet
- World Heart Day: September - 2011 Risk Factor Control and Life Style Modification For Prevention of Ischemic Heart DiseaseDocument35 pagesWorld Heart Day: September - 2011 Risk Factor Control and Life Style Modification For Prevention of Ischemic Heart DiseaseSoikotNo ratings yet
- Stroke 1Document35 pagesStroke 1Aisyah IcahNo ratings yet
- Drugs and Doping in SportDocument39 pagesDrugs and Doping in SportAbhijit Sharma100% (1)
- BurnsDocument58 pagesBurnsMarie MayNo ratings yet
- Life Threatening Rhythm: Presenter: Muhammad Najmuddin Bin Hussain 2. Wan Muhammad Nasirudin Bin Wan YusoffDocument17 pagesLife Threatening Rhythm: Presenter: Muhammad Najmuddin Bin Hussain 2. Wan Muhammad Nasirudin Bin Wan YusoffWan NasirudinNo ratings yet
- What Is A Heart Attack?Document5 pagesWhat Is A Heart Attack?hesitajohnrey100% (1)
- Acls LectureDocument15 pagesAcls LectureVincent BautistaNo ratings yet
- KON HandbookDocument78 pagesKON HandbookRasyad KamalNo ratings yet
- Instant Alert For Myocardial Infarction Keshav Singhal Shri Vaishnav Institute of Tech. & Science Indore EMAIL ADD: Keshav - Svits@yahoo - Co.inDocument7 pagesInstant Alert For Myocardial Infarction Keshav Singhal Shri Vaishnav Institute of Tech. & Science Indore EMAIL ADD: Keshav - Svits@yahoo - Co.inKeshav SinghalNo ratings yet
- Pre Anaesthetic Check-UpDocument4 pagesPre Anaesthetic Check-UpUdoy PaulNo ratings yet
- Nota BLS Siri 1Document37 pagesNota BLS Siri 1PUSAT LATIHAN AADK100% (1)
- Examination Lumps and BumpsDocument4 pagesExamination Lumps and BumpsSodiqa Strida SaSi TwinzNo ratings yet
- Nursing Care of The Client With Burn Injury: BurnsDocument40 pagesNursing Care of The Client With Burn Injury: BurnsAhmad Rayan100% (2)
- CPG Management DiabetesDocument49 pagesCPG Management DiabetesEmi Tri SiswantiNo ratings yet
- Polytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaDocument57 pagesPolytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaAbuhafezbaka100% (1)
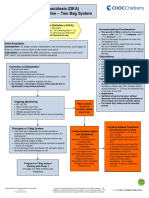
- Diabetic Ketoacidosis Care GuidelineDocument5 pagesDiabetic Ketoacidosis Care GuidelineRahma DhNo ratings yet
- Advanced Trauma and Life Support (ATLS) : EpidemiologyDocument7 pagesAdvanced Trauma and Life Support (ATLS) : EpidemiologyMohamed FarahatNo ratings yet
- 3rd (X) Lecture (NCM106 ABC IV) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingDocument17 pages3rd (X) Lecture (NCM106 ABC IV) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingKamx Mohammed100% (1)
- Triage in Polytauma: Prof. Dr. A. Chandrasekaran M.S., PH.D.Document73 pagesTriage in Polytauma: Prof. Dr. A. Chandrasekaran M.S., PH.D.ShrutiNo ratings yet
- Emergency Medicine 2001 PDFDocument44 pagesEmergency Medicine 2001 PDFJoel Antonio García AlvarezNo ratings yet
- Principles of Palliative Care (Edited) PPC-1Document33 pagesPrinciples of Palliative Care (Edited) PPC-1Mohamed Saeed BachooNo ratings yet
- Spina BifidaDocument23 pagesSpina BifidaMohamed Saeed BachooNo ratings yet
- Wa0008Document49 pagesWa0008Mohamed Saeed BachooNo ratings yet
- Surg Sem 3 Cat 2Document8 pagesSurg Sem 3 Cat 2Mohamed Saeed BachooNo ratings yet
- Bleeding and HemostasisDocument24 pagesBleeding and HemostasisMohamed Saeed BachooNo ratings yet
- Surgical Drains: Dr. George MugenyaDocument21 pagesSurgical Drains: Dr. George MugenyaMohamed Saeed BachooNo ratings yet
- Surgical Ethics: Dr. MugenyaDocument18 pagesSurgical Ethics: Dr. MugenyaMohamed Saeed BachooNo ratings yet
- AutopsyDocument37 pagesAutopsyMohamed Saeed BachooNo ratings yet
- Prognostic Value of Preoperative Neutrophil-To-Lymphocyte Ratio For Prediction of Severe CholecystitisDocument7 pagesPrognostic Value of Preoperative Neutrophil-To-Lymphocyte Ratio For Prediction of Severe CholecystitisDrelsayed HagagNo ratings yet
- Cardiac Rehabilitation Following Open-Heart Surgery in ChildrenDocument7 pagesCardiac Rehabilitation Following Open-Heart Surgery in ChildrenegajayaNo ratings yet
- Mourning in Children A Theoretical Synthesis and Clinical ApplicationDocument8 pagesMourning in Children A Theoretical Synthesis and Clinical ApplicationGary FreedmanNo ratings yet
- Coulson Institute 2014 ManualDocument305 pagesCoulson Institute 2014 ManualMaria Frola100% (1)
- Lab 10 Semen AnalysisDocument45 pagesLab 10 Semen AnalysisFeroz KhanNo ratings yet
- Modified Infectious - 1Document171 pagesModified Infectious - 1Shreya SinghNo ratings yet
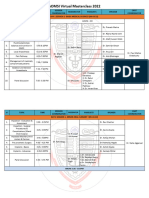
- AOMSI MC2022 ScheduleDocument10 pagesAOMSI MC2022 ScheduleDarain ShahidNo ratings yet
- Diagnostic Test Third YearDocument1 pageDiagnostic Test Third YearNesrine EnglishNo ratings yet
- m7 KimDocument4 pagesm7 KimKimberly CarmenNo ratings yet
- Gastric Analysis: Printable Version Download PDF Cite This PageDocument4 pagesGastric Analysis: Printable Version Download PDF Cite This PageFranz Mercader100% (1)
- Breast ExaminationDocument3 pagesBreast ExaminationShum Wing Hei JoanneNo ratings yet
- American Journal of Emergency Medicine: Dietrich Jehle Mary Claire Lark, Clay O'BrienDocument3 pagesAmerican Journal of Emergency Medicine: Dietrich Jehle Mary Claire Lark, Clay O'BrienGufront MustofaNo ratings yet
- Review The Causes of Decreased Breath SoundsDocument1 pageReview The Causes of Decreased Breath SoundsArvinth Guna SegaranNo ratings yet
- Early Tooth Loss in ChildrenDocument4 pagesEarly Tooth Loss in ChildrenFatima AliNo ratings yet
- Ebook Foundations For Population Health in Community Public Health Nursing PDF Full Chapter PDFDocument67 pagesEbook Foundations For Population Health in Community Public Health Nursing PDF Full Chapter PDFmargaret.forbes670100% (29)
- HBP 2.0-For Website V2 PDFDocument26 pagesHBP 2.0-For Website V2 PDFapurva shahNo ratings yet
- Assessing and Treating Patients With Impulsivity, Compulsivity and AddictionDocument7 pagesAssessing and Treating Patients With Impulsivity, Compulsivity and AddictionGeorsen GeorgeNo ratings yet
- HLH-2020-ASH TalkDocument43 pagesHLH-2020-ASH TalkИван НегарэNo ratings yet
- Aratiles Chap 1 3Document34 pagesAratiles Chap 1 3Gilbert75% (12)
- Malawi PP LegislationDocument36 pagesMalawi PP LegislationErmiyas YeshitlaNo ratings yet
- Cutting-Edge Natural Secrets For Healing Your Heart, Bob LivingstonDocument98 pagesCutting-Edge Natural Secrets For Healing Your Heart, Bob LivingstonAniko Gergely-Varga100% (1)
- Traditional Medicinal Plants of Nigeria: An Overview: Monier M. Abd El-GhaniDocument28 pagesTraditional Medicinal Plants of Nigeria: An Overview: Monier M. Abd El-GhaniOyediran OlabamijiNo ratings yet
- Indigenous System of MedicineDocument33 pagesIndigenous System of MedicinePrajwal ChhetriNo ratings yet
- LogrollingDocument1 pageLogrollingLoren MisticaNo ratings yet
- Bcs ReportDocument20 pagesBcs ReportShwetaNo ratings yet
- Akanksha Gupta FinalDraft - WHO - WordDocument114 pagesAkanksha Gupta FinalDraft - WHO - WordAkanksha GuptaNo ratings yet
- Pharmacology 208 Power PointDocument402 pagesPharmacology 208 Power PointYasmin Jeffries SingletonNo ratings yet
- Iv. Guidance Chapter: Bi-Rads - MammographyDocument7 pagesIv. Guidance Chapter: Bi-Rads - MammographyAmritNo ratings yet