Download as pptx, pdf, or txt
You might also like
- Jacobs RiggingDocument27 pagesJacobs Riggingreborn_willy50% (2)
- Captive - A Guard's Tale From Malachi's Perspective - Sarah FineDocument65 pagesCaptive - A Guard's Tale From Malachi's Perspective - Sarah FineJakus SzilveeNo ratings yet
- Six Pack Shortcuts Exercise SubstitutionDocument6 pagesSix Pack Shortcuts Exercise SubstitutionMicky LiNo ratings yet
- Cross, Melinda - Lion of DarknessDocument209 pagesCross, Melinda - Lion of Darknesskata_zjalic90% (10)
- Kamis, 05/11/2020: Bedah Thorax Kardio VaskulerDocument2 pagesKamis, 05/11/2020: Bedah Thorax Kardio VaskulerRadenSiwi Bagus HadhiningratNo ratings yet
- NP 2. Mrs. Imas Komariah / / 31 Yo / 1709274 / Spine / RD: CC: Weakness of Both Lower Extremities HistoryDocument6 pagesNP 2. Mrs. Imas Komariah / / 31 Yo / 1709274 / Spine / RD: CC: Weakness of Both Lower Extremities HistoryGina Lestari IINo ratings yet
- March 10, 2020Document2 pagesMarch 10, 2020Diana Colleen DimayugaNo ratings yet
- Assessment and Concept Map Care Plan For Critical Care PatientDocument11 pagesAssessment and Concept Map Care Plan For Critical Care Patientapi-508432180No ratings yet
- MR CITO Minggu, 22 November 2021 Debri Belum SelesaiDocument26 pagesMR CITO Minggu, 22 November 2021 Debri Belum Selesaiwim adhitamaNo ratings yet
- Duty Rabu 13 10 21 Post Pra MRDocument91 pagesDuty Rabu 13 10 21 Post Pra MRAmrina RosyadaNo ratings yet
- Resume CPC 8-8-2018Document2 pagesResume CPC 8-8-2018okkiemsNo ratings yet
- Weekly 11 August BTKV 2Document10 pagesWeekly 11 August BTKV 2Anggita ChandraNo ratings yet
- Pasbar 23022023Document8 pagesPasbar 23022023hafizalfarizieNo ratings yet
- 852-Article Text-1602-1-10-20190613Document12 pages852-Article Text-1602-1-10-20190613anidar1245No ratings yet
- Neuropathic Pain in Daily Practice: Teddy Wijatmiko, DR - SP.SDocument52 pagesNeuropathic Pain in Daily Practice: Teddy Wijatmiko, DR - SP.SeciNo ratings yet
- Daftar Pasien Baru Bedah Saraf 8 Maret 2019: Divisi TGL in Nama U MR Diagnosa R Rencana KS R Problem J KDocument1 pageDaftar Pasien Baru Bedah Saraf 8 Maret 2019: Divisi TGL in Nama U MR Diagnosa R Rencana KS R Problem J KFaisal AkbarNo ratings yet
- (Trauma) 14 Des 22 - An - Nashwan - CF Antebrachii DDocument14 pages(Trauma) 14 Des 22 - An - Nashwan - CF Antebrachii Dnadiya salmaNo ratings yet
- October 31,2019: TH TH TH THDocument4 pagesOctober 31,2019: TH TH TH THYoussry JaranillaNo ratings yet
- Case Presentation: Old Fracture 1/3 Middle Right Radius Et UlnaDocument35 pagesCase Presentation: Old Fracture 1/3 Middle Right Radius Et UlnaMuhammad Yasdar BahriNo ratings yet
- List 20 November 2018 - AWKDocument1 pageList 20 November 2018 - AWKPriza RazunipNo ratings yet
- NG Teng Fong Discharge DocumentsDocument14 pagesNG Teng Fong Discharge DocumentsAnonymous yGwMIPJRawNo ratings yet
- SICU Nov 2Document5 pagesSICU Nov 2Youssry JaranillaNo ratings yet
- Morning Report OrthopaediDocument28 pagesMorning Report OrthopaeditaniamaulaniNo ratings yet
- Surgeon Should Learn Not Just How To Operate But How To Create System of CareDocument15 pagesSurgeon Should Learn Not Just How To Operate But How To Create System of Careamal.fathullahNo ratings yet
- Grace Kinan MRDocument11 pagesGrace Kinan MRNathalia MariaNo ratings yet
- Duty 30 1 2024 Gabung Ortho Post KoreksiDocument100 pagesDuty 30 1 2024 Gabung Ortho Post Koreksijonathanhartanto89No ratings yet
- Medical Consultation From Neurology Department: The Aim of ConsultationDocument19 pagesMedical Consultation From Neurology Department: The Aim of ConsultationIka AyuNo ratings yet
- 3 MAIN B February 23Document13 pages3 MAIN B February 23Student Access SLMC-IMNo ratings yet
- 1st Clinical NCPDocument4 pages1st Clinical NCPjoidaNo ratings yet
- List Pasien NS Ruangan 2.6.21Document4 pagesList Pasien NS Ruangan 2.6.21DICKY PANDUWINATANo ratings yet
- Surgeon Should Learn Not Just How To Operate But How To Create System of CareDocument19 pagesSurgeon Should Learn Not Just How To Operate But How To Create System of Careamal.fathullahNo ratings yet
- Teleconference 23 Juli 2019Document11 pagesTeleconference 23 Juli 2019Vita DesriantiNo ratings yet
- Bagan Alur MeningiomaDocument2 pagesBagan Alur MeningiomaRiri DaynuriNo ratings yet
- (Trauma) 2 - 07 - 2023 - SDR Sulthan - Dislocation Elbow DDocument13 pages(Trauma) 2 - 07 - 2023 - SDR Sulthan - Dislocation Elbow DRasyidu MashuriNo ratings yet
- Duty Anemia Def Fe + UtiDocument5 pagesDuty Anemia Def Fe + UtigemaNo ratings yet
- Update Pasien NC 11 Januari Untuk Konsulen-1Document2 pagesUpdate Pasien NC 11 Januari Untuk Konsulen-1bobirfansyahputraNo ratings yet
- Psoriatic ArthritisDocument24 pagesPsoriatic ArthritisgemaNo ratings yet
- Chaudhari Imaging Associates PVT - Ltd.Document11 pagesChaudhari Imaging Associates PVT - Ltd.Amit SinghNo ratings yet
- Parade Wspos DarkDocument3 pagesParade Wspos Darkirwan_201291No ratings yet
- Potongan Lapjag WildanDocument9 pagesPotongan Lapjag WildanHafiz AlfarizieNo ratings yet
- No. Room/ Admission Identity Diagnosis Problem Treatment/ Planning Pre/ Post OpDocument5 pagesNo. Room/ Admission Identity Diagnosis Problem Treatment/ Planning Pre/ Post OpYuda RadityaNo ratings yet
- MR 2 Juni OA, AzotemiaDocument32 pagesMR 2 Juni OA, AzotemiaAlvin PratamaNo ratings yet
- MR 2 Juni OA, AzotemiaDocument32 pagesMR 2 Juni OA, AzotemiaWenNy RupiNaNo ratings yet
- Penfield's Motor Homunculus Revisited:: MR Prajwal GhimireDocument19 pagesPenfield's Motor Homunculus Revisited:: MR Prajwal GhimireEdwin Yahir GalvisNo ratings yet
- Daftar Pasien Baru Bedah Saraf 9 April 2019: Divisi TGL in Nama U MR Diagnosa R Rencana KS R Problem J KDocument1 pageDaftar Pasien Baru Bedah Saraf 9 April 2019: Divisi TGL in Nama U MR Diagnosa R Rencana KS R Problem J KFaisal AkbarNo ratings yet
- Img 0001Document1 pageImg 0001mohan bNo ratings yet
- Responsi Kasus: Disusunoleh: Elisa Isdasari 16710Document11 pagesResponsi Kasus: Disusunoleh: Elisa Isdasari 16710abdiNo ratings yet
- Chief Complaint: History TakingDocument9 pagesChief Complaint: History TakingMohamad ZulfikarNo ratings yet
- Update Pasien NC 22092023 Untuk KonsulenDocument1 pageUpdate Pasien NC 22092023 Untuk KonsulenHafiz AlfarizieNo ratings yet
- December 12Document12 pagesDecember 12Reda SoNo ratings yet
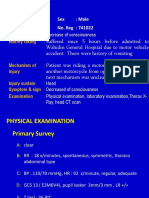
- No. Name: Mr. L Sex: Male Age: 20 Years Old No. Reg: 741022Document5 pagesNo. Name: Mr. L Sex: Male Age: 20 Years Old No. Reg: 741022Francesc OktofabregasNo ratings yet
- DDHDHSDHDocument38 pagesDDHDHSDHHarlan SiMarmutNo ratings yet
- Neurosurgery Report Sunday, 30 September 2012Document43 pagesNeurosurgery Report Sunday, 30 September 2012Ananta WinartoNo ratings yet
- Case ReportDocument24 pagesCase ReportRiski Wahyudi LasarikaNo ratings yet
- NCP Ischemic StrokeDocument4 pagesNCP Ischemic StrokeDenise Loren O. PamaongNo ratings yet
- امينDocument2 pagesامينm.ghafouri2017No ratings yet
- Choanal Atresia For ISUOG-Jerusalem 2018Document10 pagesChoanal Atresia For ISUOG-Jerusalem 2018Ahmed H. Ali ElbestaweyNo ratings yet
- Cold Spot Bone Imaging PDFDocument472 pagesCold Spot Bone Imaging PDFvijay singhNo ratings yet
- JTCS 2016Document11 pagesJTCS 2016Francielly GenuinoNo ratings yet
- Emergency Surgical Services Wednesday, October 7 2015: Doctors On DutyDocument56 pagesEmergency Surgical Services Wednesday, October 7 2015: Doctors On DutyWulan MulyaniNo ratings yet
- Update Pasien NC 03 Desember 2022 Untuk KonsulenDocument2 pagesUpdate Pasien NC 03 Desember 2022 Untuk Konsulenbosnia agusNo ratings yet
- (Trauma) - TN Latif - 17-09-2023Document18 pages(Trauma) - TN Latif - 17-09-2023Rasyidu MashuriNo ratings yet
- Sample Emg/Ncv Report - Normal StudyDocument5 pagesSample Emg/Ncv Report - Normal StudyPhysiotherapist AliNo ratings yet
- Da Kou An e Giudicelli 2014Document1 pageDa Kou An e Giudicelli 2014Anonymous KsxN7vIQxbNo ratings yet
- 19857-285991-3-PB - Viii Il 10Document11 pages19857-285991-3-PB - Viii Il 10Anonymous KsxN7vIQxbNo ratings yet
- Urology Patients Friday 01 June 2018: Dr. Dr. Basuki Bambang Purnomo, Sp.U (K)Document187 pagesUrology Patients Friday 01 June 2018: Dr. Dr. Basuki Bambang Purnomo, Sp.U (K)Anonymous KsxN7vIQxbNo ratings yet
- Kidney and Urinary System Anatomy&PhysiologyDocument52 pagesKidney and Urinary System Anatomy&PhysiologyAnonymous KsxN7vIQxbNo ratings yet
- Daman Wound Care MangmentDocument5 pagesDaman Wound Care Mangmentriyas mhdNo ratings yet
- Balance Exercise For ElderlyDocument46 pagesBalance Exercise For ElderlyReni ZubirNo ratings yet
- ABLS PROVIDER MANUAL 2015 Revisions PDFDocument133 pagesABLS PROVIDER MANUAL 2015 Revisions PDFBrinaNo ratings yet
- SciaticaDocument35 pagesSciaticaRahmadanii RahmadaniiNo ratings yet
- Burn GuidelineDocument7 pagesBurn GuidelinegreenNo ratings yet
- Bridge Plating PDFDocument4 pagesBridge Plating PDFKae 王珊婷 Wang100% (1)
- PD Dressings PDFDocument8 pagesPD Dressings PDFaksmahajanNo ratings yet
- Brachial Plexus Anesthesia: A Review of The Relevant Anatomy, Complications, and Anatomical VariationsDocument12 pagesBrachial Plexus Anesthesia: A Review of The Relevant Anatomy, Complications, and Anatomical VariationsLucille IlaganNo ratings yet
- Anatomy Lec 9 (Muscles)Document21 pagesAnatomy Lec 9 (Muscles)HumrazNo ratings yet
- Plagiarism Report SampleDocument2 pagesPlagiarism Report SampleParatech EngineeringNo ratings yet
- Operating Instructions: Radial Drill Press R32Document23 pagesOperating Instructions: Radial Drill Press R32Osama EidNo ratings yet
- Tower Crane InstallationDocument6 pagesTower Crane Installationloveson709100% (1)
- Dynamic StretchingDocument46 pagesDynamic Stretchingdeepblue9700100% (4)
- Tonight'S Game Information: CHICAGO CUBS (6-7) vs. SEATTLE MARINERS (11-4-1)Document2 pagesTonight'S Game Information: CHICAGO CUBS (6-7) vs. SEATTLE MARINERS (11-4-1)WWU_SIDNo ratings yet
- Active and Passive Insufficiency - PhysiopediaDocument5 pagesActive and Passive Insufficiency - Physiopediateam7MFkkOP YT50% (2)
- Benefits of Massage PowerpointDocument31 pagesBenefits of Massage PowerpointJeremiah TannNo ratings yet
- Urinary System - Gross 2016Document73 pagesUrinary System - Gross 2016dawnparkNo ratings yet
- En Ox A Par inDocument3 pagesEn Ox A Par inapi-3797941No ratings yet
- Position Paper About Cebu PacificDocument1 pagePosition Paper About Cebu PacificPeter Paul ParasNo ratings yet
- SJMC - xi-nCP&HTP - Impaired Skin IntegrityDocument10 pagesSJMC - xi-nCP&HTP - Impaired Skin IntegrityJoy CompetenteNo ratings yet
- Justin Ubay BSN212 Group 48A FracturesDocument5 pagesJustin Ubay BSN212 Group 48A FracturesubaycentralNo ratings yet
- Inguinal Hernia SlidesDocument42 pagesInguinal Hernia SlidesEzekiel Arteta100% (1)
- Dr. Ibrahim Bashayreh RN, PHDDocument16 pagesDr. Ibrahim Bashayreh RN, PHDEndy DestriawanNo ratings yet
- MC33883Document21 pagesMC33883Nguyen TuanNo ratings yet
- The Journal of ArthroplastyDocument5 pagesThe Journal of Arthroplastyosman gorkemNo ratings yet
- AnanomyDocument7 pagesAnanomyapi-552730621No ratings yet