
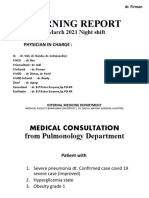
Morning Report: Physician in Charge
Morning Report: Physician in Charge
You might also like
- Critical Care Nursing A Holistic Approach 11th Edition Morton Fontaine Test Bank PDFDocument335 pagesCritical Care Nursing A Holistic Approach 11th Edition Morton Fontaine Test Bank PDFSami Atawi100% (1)
- SITXFSA001 - Written AssessmentDocument16 pagesSITXFSA001 - Written Assessmenthazem khudairNo ratings yet
- Gangrene Hand of Mrs. Mustiah, 86 YoDocument27 pagesGangrene Hand of Mrs. Mustiah, 86 YoWilujeng AnggrainiNo ratings yet
- Yen CKD AloDocument31 pagesYen CKD AloSafira RNo ratings yet
- POMR Satiti Acute CholangitisDocument30 pagesPOMR Satiti Acute CholangitisIka AyuNo ratings yet
- Morning Report: Date: 6 April 2021Document17 pagesMorning Report: Date: 6 April 2021Adinda DianNo ratings yet
- Morning Report: Date: Monday, 2 November 2020Document24 pagesMorning Report: Date: Monday, 2 November 2020Ika AyuNo ratings yet
- Sos Pomr SatitiDocument30 pagesSos Pomr SatitiIka AyuNo ratings yet
- Morning Report: Physician in ChargeDocument33 pagesMorning Report: Physician in ChargeIka AyuNo ratings yet
- Morning Report: Physician in ChargeDocument21 pagesMorning Report: Physician in ChargePHOENIX LUNANo ratings yet
- Morning ReportDocument17 pagesMorning Reportjoe joeNo ratings yet
- Morning Report: Monday, 8 May 2017Document25 pagesMorning Report: Monday, 8 May 2017HarisNo ratings yet
- Morning Report: Physician in ChargeDocument11 pagesMorning Report: Physician in ChargeImam Mi'raj SuprayogaNo ratings yet
- Morning Report: June 2022 Physician in ChargeDocument24 pagesMorning Report: June 2022 Physician in ChargeIka AyuNo ratings yet
- Ahmad Basori VidiDocument30 pagesAhmad Basori VidiIka AyuNo ratings yet
- Friday 2-2-2018 Multiple MyelomaDocument20 pagesFriday 2-2-2018 Multiple MyelomaJefri SusantoNo ratings yet
- Duty Report: Sunday, 27 May 2018Document17 pagesDuty Report: Sunday, 27 May 2018HarisNo ratings yet
- Hypocalcemia, Hypoparathyroid WahyuDocument27 pagesHypocalcemia, Hypoparathyroid WahyuFerdinando BaehaNo ratings yet
- Summary of Data Base: MR Z/41 YO/W.26Document35 pagesSummary of Data Base: MR Z/41 YO/W.26Faricha KurniaNo ratings yet
- Friday 2-2-2018 CKD HT DMDocument31 pagesFriday 2-2-2018 CKD HT DMJefri SusantoNo ratings yet
- MedCon Template - Melena+DOC+Septic ConditionDocument26 pagesMedCon Template - Melena+DOC+Septic ConditionPramudia DeniNo ratings yet
- Pomr Alul CKD SobDocument20 pagesPomr Alul CKD SobSeptabian IskandarNo ratings yet
- Firman - CKD ST V + CKDMBDDocument28 pagesFirman - CKD ST V + CKDMBDAdinda DianNo ratings yet
- Adenocarcinoma Rectal + UgibDocument26 pagesAdenocarcinoma Rectal + UgibgemaNo ratings yet
- Morning Report CKDDocument20 pagesMorning Report CKDjoe joeNo ratings yet
- Date: December 25th, 2021 Emanuela Indah Hanani Fadiah Desnawisk Evira Natasya Yusuf Jeanne Gabrielle Wibowo Karina Rahmawati E.PDocument14 pagesDate: December 25th, 2021 Emanuela Indah Hanani Fadiah Desnawisk Evira Natasya Yusuf Jeanne Gabrielle Wibowo Karina Rahmawati E.PTania Krisna PutriNo ratings yet
- Morning Report: Date: 1 June 2019Document15 pagesMorning Report: Date: 1 June 2019Erwin HidayatNo ratings yet
- SOS AYU - Ax - PeunjangDocument11 pagesSOS AYU - Ax - PeunjangIka AyuNo ratings yet
- MR DOC KAD DR HeriDocument16 pagesMR DOC KAD DR HeriIffaNo ratings yet
- Morning ReportDocument27 pagesMorning ReportDody PrasetyaNo ratings yet
- MR - INCOVIT - 30521 - Probable Covid-Complicated UTI - SAHDocument24 pagesMR - INCOVIT - 30521 - Probable Covid-Complicated UTI - SAHIka AyuNo ratings yet
- POMR FAH BAshori CMLDocument22 pagesPOMR FAH BAshori CMLIka AyuNo ratings yet
- Malaria Cerebral: Agnes Wanda SuwantoDocument21 pagesMalaria Cerebral: Agnes Wanda SuwantoAgnes Wanda SuwantoNo ratings yet
- POMR SATITI - Nephrotic SyndromeDocument27 pagesPOMR SATITI - Nephrotic SyndromeIka AyuNo ratings yet
- Ponda Leiomyosarcoma 7-9-2018Document12 pagesPonda Leiomyosarcoma 7-9-2018DoctoRides 46No ratings yet
- Laporan Kasus Cardio CHF Ec CADDocument14 pagesLaporan Kasus Cardio CHF Ec CADHilyah Fadhilah Al HamdaniNo ratings yet
- Responsi Stemi Dr. Tuko SP - JP FixDocument56 pagesResponsi Stemi Dr. Tuko SP - JP FixcintaNo ratings yet
- Mr. Y A S / 49 Y.o/ Ward Chief Complaint: Lump in Chest History of Present IllnessDocument31 pagesMr. Y A S / 49 Y.o/ Ward Chief Complaint: Lump in Chest History of Present IllnessIka AyuNo ratings yet
- Morning Report Case: MarchDocument20 pagesMorning Report Case: Marchputri meiliawatiNo ratings yet
- Program Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaDocument27 pagesProgram Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaIka AyuNo ratings yet
- POMR Satiti Medical Consultation FixDocument18 pagesPOMR Satiti Medical Consultation FixIka AyuNo ratings yet
- Its Just HoaxDocument10 pagesIts Just HoaxArkhan HanafiNo ratings yet
- CKD CapdDocument20 pagesCKD CapdgemaNo ratings yet
- Wa0024Document25 pagesWa0024sujarot dwiNo ratings yet
- Afina Fitra Firdaus Ppds Ipd 50Document30 pagesAfina Fitra Firdaus Ppds Ipd 5050Afina Fitra FirdausNo ratings yet
- Jaga Tengah - MedCon - 010321 - CAMDocument22 pagesJaga Tengah - MedCon - 010321 - CAMAdinda DianNo ratings yet
- Mrs Siti Wahyuni/ 48 Yo/ Ward 25 Bed 1.6Document7 pagesMrs Siti Wahyuni/ 48 Yo/ Ward 25 Bed 1.6DoctoRides 46No ratings yet
- Shock SepticDocument35 pagesShock SepticAkbar SyarialNo ratings yet
- Case ReportDocument34 pagesCase ReportMiftahul JannahNo ratings yet
- Morning Report: Physician in ChargeDocument15 pagesMorning Report: Physician in ChargeJefri SusantoNo ratings yet
- Duty Report Saturday, May 2 2015 Dr. Ramadhan Physician in ChargeDocument6 pagesDuty Report Saturday, May 2 2015 Dr. Ramadhan Physician in ChargeCristian RajagukgukNo ratings yet
- Stemi Anterior ExtensiveDocument29 pagesStemi Anterior ExtensiveNur Abidatul FitriaNo ratings yet
- Duty Report 4 CKDDocument5 pagesDuty Report 4 CKDCristian RajagukgukNo ratings yet
- Case of DeathDocument37 pagesCase of Deathnina purnamasariNo ratings yet
- Laporan Kasus CHFDocument27 pagesLaporan Kasus CHFBerka Phillia NingrumNo ratings yet
- MR R 26 6-3 2017 MR W Fix AMS Septic AKIDocument15 pagesMR R 26 6-3 2017 MR W Fix AMS Septic AKISafira RNo ratings yet
- Case #3 - Heart Failure History of Present IllnessDocument5 pagesCase #3 - Heart Failure History of Present IllnessPerlyn Mac Basiloy - AloNo ratings yet
- CAP AfinaDocument30 pagesCAP Afinaphyna27No ratings yet
- Hipokalsemia - KSMDocument22 pagesHipokalsemia - KSMAdinda DianNo ratings yet
- Morning Report 24-9Document18 pagesMorning Report 24-9hendra nuraminNo ratings yet
- MR Belakang 24022021 RAM Ca Buli EDITDocument25 pagesMR Belakang 24022021 RAM Ca Buli EDITWilujeng AnggrainiNo ratings yet
- Azotemia - Tumor BuliDocument2 pagesAzotemia - Tumor BuliWilujeng AnggrainiNo ratings yet
- Gangrene Hand of Mrs. Mustiah, 86 YoDocument27 pagesGangrene Hand of Mrs. Mustiah, 86 YoWilujeng AnggrainiNo ratings yet
- MR BHD / 53 Y.o/ W.24ADocument22 pagesMR BHD / 53 Y.o/ W.24AWilujeng AnggrainiNo ratings yet
- IGD BAR Confirmed CovidDocument4 pagesIGD BAR Confirmed CovidWilujeng AnggrainiNo ratings yet
- MR Belakang 24022021 RAM Ca Buli EDITDocument25 pagesMR Belakang 24022021 RAM Ca Buli EDITWilujeng AnggrainiNo ratings yet
- Morning Report: 2 March 2021 Night ShiftDocument16 pagesMorning Report: 2 March 2021 Night ShiftWilujeng AnggrainiNo ratings yet
- POMR - Belakang - Nanda NHL 0103Document36 pagesPOMR - Belakang - Nanda NHL 0103Wilujeng AnggrainiNo ratings yet
- 02-03-21 - Impending Thyroid Storm PerioperativeDocument4 pages02-03-21 - Impending Thyroid Storm PerioperativeWilujeng AnggrainiNo ratings yet
- Indri Astutik CAPD Peritonitis RezdyDocument2 pagesIndri Astutik CAPD Peritonitis RezdyWilujeng AnggrainiNo ratings yet
- Cue and Clue Problem List and Initial Diagnosis PlanningDocument2 pagesCue and Clue Problem List and Initial Diagnosis PlanningWilujeng AnggrainiNo ratings yet
- Teaching-Learning Models in Clinical Setting: Susanto NugrohoDocument47 pagesTeaching-Learning Models in Clinical Setting: Susanto NugrohoWilujeng AnggrainiNo ratings yet
- Family Planning Semester VDocument82 pagesFamily Planning Semester Vduaabdullah33No ratings yet
- Meptin® Swinghaler®: Dry Powder InhalerDocument9 pagesMeptin® Swinghaler®: Dry Powder InhalerYusuf HadiNo ratings yet
- Biodeterioration of Cosmetic ProductsDocument21 pagesBiodeterioration of Cosmetic ProductsSundaralingam RajNo ratings yet
- Cannabis Marijuana) and AnesthesiaDocument6 pagesCannabis Marijuana) and AnesthesiasuckeydluffyNo ratings yet
- Parameters of Fluid Responsiveness Curr Op Crit Care Shi2020Document8 pagesParameters of Fluid Responsiveness Curr Op Crit Care Shi2020Tadeo PradoNo ratings yet
- The Influence of Probiotic Bacteria and Human Gut Microorganisms Causing Opportunistic Infections On Blastocystis ST3Document11 pagesThe Influence of Probiotic Bacteria and Human Gut Microorganisms Causing Opportunistic Infections On Blastocystis ST3Esteli189No ratings yet
- Sociological JurisprudenceDocument8 pagesSociological JurisprudenceLAW MANTRA100% (1)
- Sex Link and Punnett Square ExamDocument2 pagesSex Link and Punnett Square ExamRouse Leanne NicolasNo ratings yet
- Gainz Village Un-Natty Guide An Intro Into PedsDocument30 pagesGainz Village Un-Natty Guide An Intro Into PedsGrant ggNo ratings yet
- Nutrients: Muscle Growth and Poultry Meat Quality IssuesDocument12 pagesNutrients: Muscle Growth and Poultry Meat Quality Issuesadin dazaNo ratings yet
- Prognosis - EBM - Bahan Kuliah Yg Dipakai - 1Document48 pagesPrognosis - EBM - Bahan Kuliah Yg Dipakai - 1WantiAsmaraNo ratings yet
- Human Herpesviruses: Christopher Downing, Natalia Mendoza, Karan Sra and Stephen K. TyringDocument45 pagesHuman Herpesviruses: Christopher Downing, Natalia Mendoza, Karan Sra and Stephen K. TyringPietro PensoNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanRhobic ManansalaNo ratings yet
- Caring For The Crew Programtm Captains' ManualDocument18 pagesCaring For The Crew Programtm Captains' ManualAdhimas ErlambangNo ratings yet
- Immune Responses in The Oral CavityDocument1 pageImmune Responses in The Oral CavityCiro GuerraNo ratings yet
- Perio 3Document6 pagesPerio 3Bea YmsnNo ratings yet
- PneumothoraxDocument26 pagesPneumothoraxToni-Ann AllenNo ratings yet
- Hydroseeding WorkDocument26 pagesHydroseeding WorkSamsiah TolaNo ratings yet
- Toward A Healthy and Harmonious Life in China: Stemming The Rising Tide of Non-Communicable DiseasesDocument48 pagesToward A Healthy and Harmonious Life in China: Stemming The Rising Tide of Non-Communicable DiseasesADB Health Sector GroupNo ratings yet
- TDR Call - 2023Document5 pagesTDR Call - 2023Misaw KasyeNo ratings yet
- Bells PalsyDocument2 pagesBells PalsyMary AbellaNo ratings yet
- Identify Hazards and Risks: By: Rosemel C. Rempillo TLE Teacher, Balogo HSDocument28 pagesIdentify Hazards and Risks: By: Rosemel C. Rempillo TLE Teacher, Balogo HSMhel Abbyzj100% (1)
- Textbook Clinical Psychosomatic Obstetrics and Gynaecology A Patient Centred Biopsychosocial Practice 1St Edition Lal Ebook All Chapter PDFDocument54 pagesTextbook Clinical Psychosomatic Obstetrics and Gynaecology A Patient Centred Biopsychosocial Practice 1St Edition Lal Ebook All Chapter PDFwilliam.hunt993100% (14)
- Central Nervous System Drug StudyDocument11 pagesCentral Nervous System Drug StudySanny L Asim Jr.No ratings yet
- Fluid and Electrolytes Checklist ProceduresDocument4 pagesFluid and Electrolytes Checklist ProceduresJamaica Leslie Noveno0% (1)
- Ma Thesis WritingDocument7 pagesMa Thesis Writingtmexyhikd100% (3)
- To Slip Inferior The Result Is A Spondylolisthesis: The Four Grades of Spondylolisthesisare As Follows: °°Document2 pagesTo Slip Inferior The Result Is A Spondylolisthesis: The Four Grades of Spondylolisthesisare As Follows: °°Katrina Vea CalaroNo ratings yet
- 500 Most Important English Questions For CDS Exam Part 2Document259 pages500 Most Important English Questions For CDS Exam Part 2Jatin BhagatNo ratings yet
































































































Download as pptx, pdf, or txt
You might also like
- Critical Care Nursing A Holistic Approach 11th Edition Morton Fontaine Test Bank PDFDocument335 pagesCritical Care Nursing A Holistic Approach 11th Edition Morton Fontaine Test Bank PDFSami Atawi100% (1)
- SITXFSA001 - Written AssessmentDocument16 pagesSITXFSA001 - Written Assessmenthazem khudairNo ratings yet
- Gangrene Hand of Mrs. Mustiah, 86 YoDocument27 pagesGangrene Hand of Mrs. Mustiah, 86 YoWilujeng AnggrainiNo ratings yet
- Yen CKD AloDocument31 pagesYen CKD AloSafira RNo ratings yet
- POMR Satiti Acute CholangitisDocument30 pagesPOMR Satiti Acute CholangitisIka AyuNo ratings yet
- Morning Report: Date: 6 April 2021Document17 pagesMorning Report: Date: 6 April 2021Adinda DianNo ratings yet
- Morning Report: Date: Monday, 2 November 2020Document24 pagesMorning Report: Date: Monday, 2 November 2020Ika AyuNo ratings yet
- Sos Pomr SatitiDocument30 pagesSos Pomr SatitiIka AyuNo ratings yet
- Morning Report: Physician in ChargeDocument33 pagesMorning Report: Physician in ChargeIka AyuNo ratings yet
- Morning Report: Physician in ChargeDocument21 pagesMorning Report: Physician in ChargePHOENIX LUNANo ratings yet
- Morning ReportDocument17 pagesMorning Reportjoe joeNo ratings yet
- Morning Report: Monday, 8 May 2017Document25 pagesMorning Report: Monday, 8 May 2017HarisNo ratings yet
- Morning Report: Physician in ChargeDocument11 pagesMorning Report: Physician in ChargeImam Mi'raj SuprayogaNo ratings yet
- Morning Report: June 2022 Physician in ChargeDocument24 pagesMorning Report: June 2022 Physician in ChargeIka AyuNo ratings yet
- Ahmad Basori VidiDocument30 pagesAhmad Basori VidiIka AyuNo ratings yet
- Friday 2-2-2018 Multiple MyelomaDocument20 pagesFriday 2-2-2018 Multiple MyelomaJefri SusantoNo ratings yet
- Duty Report: Sunday, 27 May 2018Document17 pagesDuty Report: Sunday, 27 May 2018HarisNo ratings yet
- Hypocalcemia, Hypoparathyroid WahyuDocument27 pagesHypocalcemia, Hypoparathyroid WahyuFerdinando BaehaNo ratings yet
- Summary of Data Base: MR Z/41 YO/W.26Document35 pagesSummary of Data Base: MR Z/41 YO/W.26Faricha KurniaNo ratings yet
- Friday 2-2-2018 CKD HT DMDocument31 pagesFriday 2-2-2018 CKD HT DMJefri SusantoNo ratings yet
- MedCon Template - Melena+DOC+Septic ConditionDocument26 pagesMedCon Template - Melena+DOC+Septic ConditionPramudia DeniNo ratings yet
- Pomr Alul CKD SobDocument20 pagesPomr Alul CKD SobSeptabian IskandarNo ratings yet
- Firman - CKD ST V + CKDMBDDocument28 pagesFirman - CKD ST V + CKDMBDAdinda DianNo ratings yet
- Adenocarcinoma Rectal + UgibDocument26 pagesAdenocarcinoma Rectal + UgibgemaNo ratings yet
- Morning Report CKDDocument20 pagesMorning Report CKDjoe joeNo ratings yet
- Date: December 25th, 2021 Emanuela Indah Hanani Fadiah Desnawisk Evira Natasya Yusuf Jeanne Gabrielle Wibowo Karina Rahmawati E.PDocument14 pagesDate: December 25th, 2021 Emanuela Indah Hanani Fadiah Desnawisk Evira Natasya Yusuf Jeanne Gabrielle Wibowo Karina Rahmawati E.PTania Krisna PutriNo ratings yet
- Morning Report: Date: 1 June 2019Document15 pagesMorning Report: Date: 1 June 2019Erwin HidayatNo ratings yet
- SOS AYU - Ax - PeunjangDocument11 pagesSOS AYU - Ax - PeunjangIka AyuNo ratings yet
- MR DOC KAD DR HeriDocument16 pagesMR DOC KAD DR HeriIffaNo ratings yet
- Morning ReportDocument27 pagesMorning ReportDody PrasetyaNo ratings yet
- MR - INCOVIT - 30521 - Probable Covid-Complicated UTI - SAHDocument24 pagesMR - INCOVIT - 30521 - Probable Covid-Complicated UTI - SAHIka AyuNo ratings yet
- POMR FAH BAshori CMLDocument22 pagesPOMR FAH BAshori CMLIka AyuNo ratings yet
- Malaria Cerebral: Agnes Wanda SuwantoDocument21 pagesMalaria Cerebral: Agnes Wanda SuwantoAgnes Wanda SuwantoNo ratings yet
- POMR SATITI - Nephrotic SyndromeDocument27 pagesPOMR SATITI - Nephrotic SyndromeIka AyuNo ratings yet
- Ponda Leiomyosarcoma 7-9-2018Document12 pagesPonda Leiomyosarcoma 7-9-2018DoctoRides 46No ratings yet
- Laporan Kasus Cardio CHF Ec CADDocument14 pagesLaporan Kasus Cardio CHF Ec CADHilyah Fadhilah Al HamdaniNo ratings yet
- Responsi Stemi Dr. Tuko SP - JP FixDocument56 pagesResponsi Stemi Dr. Tuko SP - JP FixcintaNo ratings yet
- Mr. Y A S / 49 Y.o/ Ward Chief Complaint: Lump in Chest History of Present IllnessDocument31 pagesMr. Y A S / 49 Y.o/ Ward Chief Complaint: Lump in Chest History of Present IllnessIka AyuNo ratings yet
- Morning Report Case: MarchDocument20 pagesMorning Report Case: Marchputri meiliawatiNo ratings yet
- Program Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaDocument27 pagesProgram Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaIka AyuNo ratings yet
- POMR Satiti Medical Consultation FixDocument18 pagesPOMR Satiti Medical Consultation FixIka AyuNo ratings yet
- Its Just HoaxDocument10 pagesIts Just HoaxArkhan HanafiNo ratings yet
- CKD CapdDocument20 pagesCKD CapdgemaNo ratings yet
- Wa0024Document25 pagesWa0024sujarot dwiNo ratings yet
- Afina Fitra Firdaus Ppds Ipd 50Document30 pagesAfina Fitra Firdaus Ppds Ipd 5050Afina Fitra FirdausNo ratings yet
- Jaga Tengah - MedCon - 010321 - CAMDocument22 pagesJaga Tengah - MedCon - 010321 - CAMAdinda DianNo ratings yet
- Mrs Siti Wahyuni/ 48 Yo/ Ward 25 Bed 1.6Document7 pagesMrs Siti Wahyuni/ 48 Yo/ Ward 25 Bed 1.6DoctoRides 46No ratings yet
- Shock SepticDocument35 pagesShock SepticAkbar SyarialNo ratings yet
- Case ReportDocument34 pagesCase ReportMiftahul JannahNo ratings yet
- Morning Report: Physician in ChargeDocument15 pagesMorning Report: Physician in ChargeJefri SusantoNo ratings yet
- Duty Report Saturday, May 2 2015 Dr. Ramadhan Physician in ChargeDocument6 pagesDuty Report Saturday, May 2 2015 Dr. Ramadhan Physician in ChargeCristian RajagukgukNo ratings yet
- Stemi Anterior ExtensiveDocument29 pagesStemi Anterior ExtensiveNur Abidatul FitriaNo ratings yet
- Duty Report 4 CKDDocument5 pagesDuty Report 4 CKDCristian RajagukgukNo ratings yet
- Case of DeathDocument37 pagesCase of Deathnina purnamasariNo ratings yet
- Laporan Kasus CHFDocument27 pagesLaporan Kasus CHFBerka Phillia NingrumNo ratings yet
- MR R 26 6-3 2017 MR W Fix AMS Septic AKIDocument15 pagesMR R 26 6-3 2017 MR W Fix AMS Septic AKISafira RNo ratings yet
- Case #3 - Heart Failure History of Present IllnessDocument5 pagesCase #3 - Heart Failure History of Present IllnessPerlyn Mac Basiloy - AloNo ratings yet
- CAP AfinaDocument30 pagesCAP Afinaphyna27No ratings yet
- Hipokalsemia - KSMDocument22 pagesHipokalsemia - KSMAdinda DianNo ratings yet
- Morning Report 24-9Document18 pagesMorning Report 24-9hendra nuraminNo ratings yet
- MR Belakang 24022021 RAM Ca Buli EDITDocument25 pagesMR Belakang 24022021 RAM Ca Buli EDITWilujeng AnggrainiNo ratings yet
- Azotemia - Tumor BuliDocument2 pagesAzotemia - Tumor BuliWilujeng AnggrainiNo ratings yet
- Gangrene Hand of Mrs. Mustiah, 86 YoDocument27 pagesGangrene Hand of Mrs. Mustiah, 86 YoWilujeng AnggrainiNo ratings yet
- MR BHD / 53 Y.o/ W.24ADocument22 pagesMR BHD / 53 Y.o/ W.24AWilujeng AnggrainiNo ratings yet
- IGD BAR Confirmed CovidDocument4 pagesIGD BAR Confirmed CovidWilujeng AnggrainiNo ratings yet
- MR Belakang 24022021 RAM Ca Buli EDITDocument25 pagesMR Belakang 24022021 RAM Ca Buli EDITWilujeng AnggrainiNo ratings yet
- Morning Report: 2 March 2021 Night ShiftDocument16 pagesMorning Report: 2 March 2021 Night ShiftWilujeng AnggrainiNo ratings yet
- POMR - Belakang - Nanda NHL 0103Document36 pagesPOMR - Belakang - Nanda NHL 0103Wilujeng AnggrainiNo ratings yet
- 02-03-21 - Impending Thyroid Storm PerioperativeDocument4 pages02-03-21 - Impending Thyroid Storm PerioperativeWilujeng AnggrainiNo ratings yet
- Indri Astutik CAPD Peritonitis RezdyDocument2 pagesIndri Astutik CAPD Peritonitis RezdyWilujeng AnggrainiNo ratings yet
- Cue and Clue Problem List and Initial Diagnosis PlanningDocument2 pagesCue and Clue Problem List and Initial Diagnosis PlanningWilujeng AnggrainiNo ratings yet
- Teaching-Learning Models in Clinical Setting: Susanto NugrohoDocument47 pagesTeaching-Learning Models in Clinical Setting: Susanto NugrohoWilujeng AnggrainiNo ratings yet
- Family Planning Semester VDocument82 pagesFamily Planning Semester Vduaabdullah33No ratings yet
- Meptin® Swinghaler®: Dry Powder InhalerDocument9 pagesMeptin® Swinghaler®: Dry Powder InhalerYusuf HadiNo ratings yet
- Biodeterioration of Cosmetic ProductsDocument21 pagesBiodeterioration of Cosmetic ProductsSundaralingam RajNo ratings yet
- Cannabis Marijuana) and AnesthesiaDocument6 pagesCannabis Marijuana) and AnesthesiasuckeydluffyNo ratings yet
- Parameters of Fluid Responsiveness Curr Op Crit Care Shi2020Document8 pagesParameters of Fluid Responsiveness Curr Op Crit Care Shi2020Tadeo PradoNo ratings yet
- The Influence of Probiotic Bacteria and Human Gut Microorganisms Causing Opportunistic Infections On Blastocystis ST3Document11 pagesThe Influence of Probiotic Bacteria and Human Gut Microorganisms Causing Opportunistic Infections On Blastocystis ST3Esteli189No ratings yet
- Sociological JurisprudenceDocument8 pagesSociological JurisprudenceLAW MANTRA100% (1)
- Sex Link and Punnett Square ExamDocument2 pagesSex Link and Punnett Square ExamRouse Leanne NicolasNo ratings yet
- Gainz Village Un-Natty Guide An Intro Into PedsDocument30 pagesGainz Village Un-Natty Guide An Intro Into PedsGrant ggNo ratings yet
- Nutrients: Muscle Growth and Poultry Meat Quality IssuesDocument12 pagesNutrients: Muscle Growth and Poultry Meat Quality Issuesadin dazaNo ratings yet
- Prognosis - EBM - Bahan Kuliah Yg Dipakai - 1Document48 pagesPrognosis - EBM - Bahan Kuliah Yg Dipakai - 1WantiAsmaraNo ratings yet
- Human Herpesviruses: Christopher Downing, Natalia Mendoza, Karan Sra and Stephen K. TyringDocument45 pagesHuman Herpesviruses: Christopher Downing, Natalia Mendoza, Karan Sra and Stephen K. TyringPietro PensoNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanRhobic ManansalaNo ratings yet
- Caring For The Crew Programtm Captains' ManualDocument18 pagesCaring For The Crew Programtm Captains' ManualAdhimas ErlambangNo ratings yet
- Immune Responses in The Oral CavityDocument1 pageImmune Responses in The Oral CavityCiro GuerraNo ratings yet
- Perio 3Document6 pagesPerio 3Bea YmsnNo ratings yet
- PneumothoraxDocument26 pagesPneumothoraxToni-Ann AllenNo ratings yet
- Hydroseeding WorkDocument26 pagesHydroseeding WorkSamsiah TolaNo ratings yet
- Toward A Healthy and Harmonious Life in China: Stemming The Rising Tide of Non-Communicable DiseasesDocument48 pagesToward A Healthy and Harmonious Life in China: Stemming The Rising Tide of Non-Communicable DiseasesADB Health Sector GroupNo ratings yet
- TDR Call - 2023Document5 pagesTDR Call - 2023Misaw KasyeNo ratings yet
- Bells PalsyDocument2 pagesBells PalsyMary AbellaNo ratings yet
- Identify Hazards and Risks: By: Rosemel C. Rempillo TLE Teacher, Balogo HSDocument28 pagesIdentify Hazards and Risks: By: Rosemel C. Rempillo TLE Teacher, Balogo HSMhel Abbyzj100% (1)
- Textbook Clinical Psychosomatic Obstetrics and Gynaecology A Patient Centred Biopsychosocial Practice 1St Edition Lal Ebook All Chapter PDFDocument54 pagesTextbook Clinical Psychosomatic Obstetrics and Gynaecology A Patient Centred Biopsychosocial Practice 1St Edition Lal Ebook All Chapter PDFwilliam.hunt993100% (14)
- Central Nervous System Drug StudyDocument11 pagesCentral Nervous System Drug StudySanny L Asim Jr.No ratings yet
- Fluid and Electrolytes Checklist ProceduresDocument4 pagesFluid and Electrolytes Checklist ProceduresJamaica Leslie Noveno0% (1)
- Ma Thesis WritingDocument7 pagesMa Thesis Writingtmexyhikd100% (3)
- To Slip Inferior The Result Is A Spondylolisthesis: The Four Grades of Spondylolisthesisare As Follows: °°Document2 pagesTo Slip Inferior The Result Is A Spondylolisthesis: The Four Grades of Spondylolisthesisare As Follows: °°Katrina Vea CalaroNo ratings yet
- 500 Most Important English Questions For CDS Exam Part 2Document259 pages500 Most Important English Questions For CDS Exam Part 2Jatin BhagatNo ratings yet