Download as ppt, pdf, or txt
You might also like
- Feasibility StudyDocument5 pagesFeasibility StudyKath Garcia50% (4)
- Encyclopedia of Chemical Processing - S Lee (Taylor and Francis, 2006) WW PDFDocument3,338 pagesEncyclopedia of Chemical Processing - S Lee (Taylor and Francis, 2006) WW PDFMahfuzur Rahman SiddikyNo ratings yet
- Causes and Treatment of Malignant Melanoma: DiscussionDocument4 pagesCauses and Treatment of Malignant Melanoma: DiscussionAriSeliengNo ratings yet
- Australian Professional Standards For TeachersDocument1 pageAustralian Professional Standards For Teachersapi-365080091No ratings yet
- Creighton University School of Medicine Department of Pathology MDDocument36 pagesCreighton University School of Medicine Department of Pathology MDDeba P SarmaNo ratings yet
- Melanocytes, Mole, MelanomaDocument35 pagesMelanocytes, Mole, MelanomaDeba P SarmaNo ratings yet
- Epidemiologyandrisk Factorsofmelanoma: Stephanie Carr,, Christy Smith,, Jessica WernbergDocument12 pagesEpidemiologyandrisk Factorsofmelanoma: Stephanie Carr,, Christy Smith,, Jessica WernbergGabriela AgrigNo ratings yet
- ABout Melanoma Skin CancerDocument11 pagesABout Melanoma Skin CancerOdair Braz JuniorNo ratings yet
- Melanoma - PregradoDocument8 pagesMelanoma - PregradoDaniela DuránNo ratings yet
- Maligna MelanomaDocument80 pagesMaligna MelanomaNoveldy PitnaNo ratings yet
- MelanomaDocument19 pagesMelanomaAdhiguna PrabawaNo ratings yet
- MelanomaDocument10 pagesMelanomaShalu RjNo ratings yet
- AnaPhy Skin Cancer Case Study-BASCODocument6 pagesAnaPhy Skin Cancer Case Study-BASCOChristine Jane BascoNo ratings yet
- Skin CancerDocument3 pagesSkin CancerourskrishNo ratings yet
- Midgut Volvulus ABSTRACTDocument27 pagesMidgut Volvulus ABSTRACTely saktiNo ratings yet
- Ultraviolet Radiation Induces Skin Cancer in Developing WorldDocument4 pagesUltraviolet Radiation Induces Skin Cancer in Developing WorldmmuruganandamNo ratings yet
- MelanomaDocument11 pagesMelanomaAriSeliengNo ratings yet
- Skin Lesion DiagnosisDocument9 pagesSkin Lesion DiagnosisaequNo ratings yet
- Group 4 Case Study On Malignant MelanomaDocument7 pagesGroup 4 Case Study On Malignant MelanomaLance JardiolinNo ratings yet
- CA de Piel y MelanomaDocument30 pagesCA de Piel y MelanomaDiego Bedón AscurraNo ratings yet
- Skin Cancer Term PaperDocument6 pagesSkin Cancer Term Paperafmzfvlopbchbe100% (1)
- Research Paper On Skin CancerDocument7 pagesResearch Paper On Skin Cancernywxluvkg100% (1)
- SKIN CANCER by Shahid and Nawaira PthologyDocument31 pagesSKIN CANCER by Shahid and Nawaira PthologyShahid BashirNo ratings yet
- Seminar: Vishal Madan, John T Lear, Rolf-Markus SzeimiesDocument13 pagesSeminar: Vishal Madan, John T Lear, Rolf-Markus SzeimiesAbdul HaseebNo ratings yet
- Malignant Melanoma and Skin Cancer: Igor Y. Galaychuk, MD, DSCDocument53 pagesMalignant Melanoma and Skin Cancer: Igor Y. Galaychuk, MD, DSCMohammadSAL-RawashdehNo ratings yet
- Melanoma Treatment (PDQ®) - National Cancer InstituteDocument33 pagesMelanoma Treatment (PDQ®) - National Cancer InstituteAnil RajaniNo ratings yet
- Cancer in Adults and ChildrenDocument21 pagesCancer in Adults and Childrenapi-313341021No ratings yet
- Oncology: Ivano-Frankivsk National Medical University Department of OncologyDocument41 pagesOncology: Ivano-Frankivsk National Medical University Department of OncologyAli Baker AlgelaneNo ratings yet
- Mrs. Maria Susan Z. MaglaquiDocument5 pagesMrs. Maria Susan Z. MaglaquiRon Agustin JrNo ratings yet
- Diagnosis and Treatment of Basal Cell and Squamous Cell CarcinomasDocument8 pagesDiagnosis and Treatment of Basal Cell and Squamous Cell CarcinomasAffan AdibNo ratings yet
- Nodular Malignant Melanoma: Case ReportDocument13 pagesNodular Malignant Melanoma: Case ReportasclepiuspdfsNo ratings yet
- Genetic Diseases: Mendelian Inheritance Multifactorial Inheritance Chromosome Inheritance Mitochondria InheritanceDocument74 pagesGenetic Diseases: Mendelian Inheritance Multifactorial Inheritance Chromosome Inheritance Mitochondria InheritanceinakiNo ratings yet
- Diagnosis and Management of Malignant MelanomaDocument10 pagesDiagnosis and Management of Malignant MelanomaDewinsNo ratings yet
- LTL CancerDocument7 pagesLTL Cancerapi-262360890No ratings yet
- Viatori 2012Document10 pagesViatori 2012jedan185No ratings yet
- Managing Malignant Melanoma: Learning Objectives: After Reading This Article, The Participant Should Be AbleDocument15 pagesManaging Malignant Melanoma: Learning Objectives: After Reading This Article, The Participant Should Be AbleDian Ariska SNo ratings yet
- Cec 2023 NejmDocument12 pagesCec 2023 Nejmgabrieeltavares_No ratings yet
- Subcutaneous MetsDocument27 pagesSubcutaneous MetsDavidJohnsonNo ratings yet
- Skin Cancer FinalDocument9 pagesSkin Cancer Finalapi-609308130No ratings yet
- Garbe2007 PDFDocument7 pagesGarbe2007 PDFArsen NitNo ratings yet
- Melanoma FinallllDocument14 pagesMelanoma FinallllHIND MOHAMEDNo ratings yet
- Cancers 13 04914Document27 pagesCancers 13 04914Caca FaizahNo ratings yet
- Bio1010 Melanoma PaperDocument5 pagesBio1010 Melanoma Paperapi-300889005No ratings yet
- Melanoma: Meku Damtie (M.D.) July 18, 2006Document38 pagesMelanoma: Meku Damtie (M.D.) July 18, 2006Worku KifleNo ratings yet
- 27.2 Nikfarjam 11-18Document8 pages27.2 Nikfarjam 11-18afm26No ratings yet
- Screening and Early Detection of Melanoma in Adults and AdolescentsDocument43 pagesScreening and Early Detection of Melanoma in Adults and AdolescentsTeytey SimpsonNo ratings yet
- Skin Cancers. Malignant MelanomaDocument53 pagesSkin Cancers. Malignant MelanomaАбдул Насер МохаммадізмаелNo ratings yet
- Tanning Salons Research PaperDocument6 pagesTanning Salons Research PaperjessicadietlinNo ratings yet
- © 2010 Mcgraw-Hill Companies. All Rights ReservedDocument36 pages© 2010 Mcgraw-Hill Companies. All Rights ReservedThalia SandersNo ratings yet
- Thyroid Cancer PDFDocument67 pagesThyroid Cancer PDFJaredNo ratings yet
- Diagnosis and Management of Skin CancerDocument6 pagesDiagnosis and Management of Skin Cancerdavin otooleNo ratings yet
- MelafindDocument5 pagesMelafindEvan KristantoNo ratings yet
- Elizabeth Swenson Student - Heritagehs - Cancer ProjectDocument10 pagesElizabeth Swenson Student - Heritagehs - Cancer Projectapi-551048845No ratings yet
- Diagnosis and Treatment of MelanomaDocument14 pagesDiagnosis and Treatment of MelanomaAnonymous Af24L7No ratings yet
- Presentation 3Document14 pagesPresentation 3Linda Lam100% (1)
- Gordon 2013Document10 pagesGordon 2013Gabriela AgrigNo ratings yet
- Collector Oncology 3Document936 pagesCollector Oncology 3Sarhan AliNo ratings yet
- Skin Cancer Research Paper 1Document4 pagesSkin Cancer Research Paper 1api-646942864No ratings yet
- Nurul Wahida BT Hamdan 030.08.301Document15 pagesNurul Wahida BT Hamdan 030.08.301Nor Ubudiah SetiNo ratings yet
- DOI03semSkC Skin CancerDocument36 pagesDOI03semSkC Skin CancermkmanNo ratings yet
- Final Project Work of English: Topic: Breast CancerDocument8 pagesFinal Project Work of English: Topic: Breast CancerLeidy AguileraNo ratings yet
- Skin CancerDocument5 pagesSkin Cancerapi-646942864No ratings yet
- A Practical Guide to Skin CancerFrom EverandA Practical Guide to Skin CancerAllison HanlonNo ratings yet
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaNo ratings yet
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaNo ratings yet
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNo ratings yet
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaNo ratings yet
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaNo ratings yet
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaNo ratings yet
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNo ratings yet
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNo ratings yet
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNo ratings yet
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNo ratings yet
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaNo ratings yet
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNo ratings yet
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaNo ratings yet
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaNo ratings yet
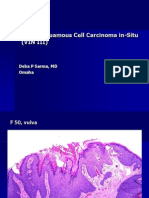
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNo ratings yet
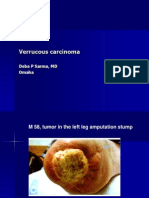
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNo ratings yet
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNo ratings yet
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Polymers in Our Daily Life PDFDocument2 pagesPolymers in Our Daily Life PDFAnjali Reddy ANo ratings yet
- 279 On CK. AMA! (Tips On Using UW) - Step2Document3 pages279 On CK. AMA! (Tips On Using UW) - Step2lashaNo ratings yet
- Essay On Flood in PakistanDocument6 pagesEssay On Flood in Pakistanjvscmacaf100% (2)
- Sisymposiumharrisburgpaworkshoptraceyvincent PDFDocument76 pagesSisymposiumharrisburgpaworkshoptraceyvincent PDFNancyNo ratings yet
- Product Environmental Profile: Canalis KNA 40A To 160ADocument7 pagesProduct Environmental Profile: Canalis KNA 40A To 160AJavier LazoNo ratings yet
- Construction of A 170m Long Cripple Sided Tunnel Using Variable Geometry Hydraulic Formwork in DTL 3, C927Document16 pagesConstruction of A 170m Long Cripple Sided Tunnel Using Variable Geometry Hydraulic Formwork in DTL 3, C927Batu GajahNo ratings yet
- Kiosk Design & Construction CriteriaDocument33 pagesKiosk Design & Construction CriteriaAdson AlcantaraNo ratings yet
- UK Terms Shell Collection Granny Square Pattern by Shelley Husband 2014Document5 pagesUK Terms Shell Collection Granny Square Pattern by Shelley Husband 2014Liz MatzNo ratings yet
- Arm RollDocument2 pagesArm Rollahmad elnggarNo ratings yet
- Acute. KetoacidosisdocxDocument12 pagesAcute. KetoacidosisdocxShara SampangNo ratings yet
- Case CX TrainingDocument20 pagesCase CX Traininghoward100% (27)
- Reactivity Series Homework Worksheet LADocument4 pagesReactivity Series Homework Worksheet LAkevinzhao704No ratings yet
- Updating Your Application From The RCM3365 To The RCM3900: 022-0131 Rev. DDocument5 pagesUpdating Your Application From The RCM3365 To The RCM3900: 022-0131 Rev. Droberto carlos anguloNo ratings yet
- Cloud Data Security: University College of Engineering, RTU, Kota (Rajasthan)Document26 pagesCloud Data Security: University College of Engineering, RTU, Kota (Rajasthan)arpita patidarNo ratings yet
- MPT Staff Rules of Service - Latest XXXYDocument126 pagesMPT Staff Rules of Service - Latest XXXYwaheedNo ratings yet
- Tel. ++39 011 9648211 - Fax ++39 011 9648222 E-Mail: Irem@irem - It - WWW - Irem.itDocument8 pagesTel. ++39 011 9648211 - Fax ++39 011 9648222 E-Mail: Irem@irem - It - WWW - Irem.itkenneth molina100% (1)
- Geotechnical Properties of Dublin Boulder ClayDocument18 pagesGeotechnical Properties of Dublin Boulder ClayBLPgalwayNo ratings yet
- Anne Lise Becker Sanofi Pasteur MSD 2Document10 pagesAnne Lise Becker Sanofi Pasteur MSD 2SRARNo ratings yet
- Instructional Methods For Teaching Social Studies: A Survey of What Middle School Students Like and Dislike About Social Studies InstructionDocument4 pagesInstructional Methods For Teaching Social Studies: A Survey of What Middle School Students Like and Dislike About Social Studies InstructionShally GuptaNo ratings yet
- Duplichecker-Plagiarism-Bab (2,3)Document2 pagesDuplichecker-Plagiarism-Bab (2,3)Sarah MaharaniNo ratings yet
- Normalized Impedance and Admittance Coordinates: Name Title Dwg. NoDocument1 pageNormalized Impedance and Admittance Coordinates: Name Title Dwg. NoJayeng WidiatmokoNo ratings yet
- Game Sense ApproachDocument7 pagesGame Sense Approachapi-408626896No ratings yet
- Lab Reproductive SDocument8 pagesLab Reproductive SJoyce TorcuatorNo ratings yet
- A Court Case On Letters of Credit & UCP600Document2 pagesA Court Case On Letters of Credit & UCP600gmat1287No ratings yet
- Eng/Npd Girish Comprehen Sive Charan Marketing: Internal Quality Audit Schedule No:Qms Ia-1Document1 pageEng/Npd Girish Comprehen Sive Charan Marketing: Internal Quality Audit Schedule No:Qms Ia-1DhinakaranNo ratings yet
- Experiment 7: Investigating The Change of Volume in The Change of Temperature (Document2 pagesExperiment 7: Investigating The Change of Volume in The Change of Temperature (EDWIN SIMBARASHE MASUNUNGURENo ratings yet
- Eskom, ABB Reach R1.5bn Settlement For Kusile Cost OverrunDocument3 pagesEskom, ABB Reach R1.5bn Settlement For Kusile Cost OverrunNokukhanya MntamboNo ratings yet