Download as pptx, pdf, or txt
You might also like
- Principle 4 Quality Right First Time Every TimeDocument18 pagesPrinciple 4 Quality Right First Time Every TimeSudhagarNo ratings yet
- Ceramah Bengkel Quality Assurance 2014Document77 pagesCeramah Bengkel Quality Assurance 2014Senthil Kumar KNo ratings yet
- Model of Risk AssessmentDocument12 pagesModel of Risk AssessmentTony Gallacher60% (5)
- Biochemical Test of BacteriaDocument33 pagesBiochemical Test of Bacteriaaziskf100% (2)
- Total Quality ManagementDocument13 pagesTotal Quality Managementshruti singhNo ratings yet
- Comprehensive Testing Services For Life Insurance SystemsDocument8 pagesComprehensive Testing Services For Life Insurance Systemswakarsheetal88No ratings yet
- QSM PrelimDocument10 pagesQSM PrelimIvana CianeNo ratings yet
- Key Performance Indicators (KPIs) Workshop - PresentationDocument42 pagesKey Performance Indicators (KPIs) Workshop - Presentationzsx4s9fts8No ratings yet
- Fungsi MNJ Pengawasan Mutu 2022Document56 pagesFungsi MNJ Pengawasan Mutu 2022patricia ngeraNo ratings yet
- Quantity AssuranceDocument29 pagesQuantity AssuranceSudha YadavNo ratings yet
- 10.06.2020 Ims Awareness Training - S-IV-VDocument31 pages10.06.2020 Ims Awareness Training - S-IV-Vyousufali56No ratings yet
- Tips For Automotive AuditorsDocument4 pagesTips For Automotive AuditorsRamón G. PachecoNo ratings yet
- IMST Unit-7 Dip ME 501Document11 pagesIMST Unit-7 Dip ME 501Kommineni Ravie KumarNo ratings yet
- Quality ManagementDocument45 pagesQuality Managementficap51232No ratings yet
- Manajemen MutuDocument31 pagesManajemen MutusunarnoNo ratings yet
- Quality AssuranceDocument16 pagesQuality AssuranceArlyn MarcelinoNo ratings yet
- Quality ManagementDocument30 pagesQuality ManagementAlamin KhanNo ratings yet
- Hospital Performance BIDocument4 pagesHospital Performance BIIda Ayu DhitayoniNo ratings yet
- Quality Assurance and Quality ImprovementDocument5 pagesQuality Assurance and Quality Improvementritsugirl_180% (1)
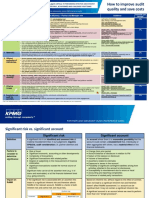
- How To Improve Audit Quality and Save CostsDocument2 pagesHow To Improve Audit Quality and Save CostsSalauddin Kader ACCANo ratings yet
- QM Week 9 MEASURING QDocument7 pagesQM Week 9 MEASURING QnadzirnasirNo ratings yet
- Assignment: Topic: Comparision of Different Quality AwardsDocument10 pagesAssignment: Topic: Comparision of Different Quality AwardsnahiyakazmiNo ratings yet
- 08 ControllingDocument133 pages08 ControllingkrishnasreeNo ratings yet
- Kendali Mutu & Kendali Biaya Melalui Penerapan Kaizen Memberikan Nilai Tambah Bagi Pasien Dan Efisiensi Di Era JKNDocument33 pagesKendali Mutu & Kendali Biaya Melalui Penerapan Kaizen Memberikan Nilai Tambah Bagi Pasien Dan Efisiensi Di Era JKNHendra William GoeyNo ratings yet
- Quality Assurance SeminarDocument26 pagesQuality Assurance Seminarselja100% (6)
- To Total Quality Management: Prepared By: PRINCESS DAE D. LIMDocument12 pagesTo Total Quality Management: Prepared By: PRINCESS DAE D. LIMCess Dae LimNo ratings yet
- Revisi PPT3-Managing QualityDocument28 pagesRevisi PPT3-Managing QualityAbdul GhoniNo ratings yet
- PPT3-Managing QualityDocument29 pagesPPT3-Managing QualityIka FitriNo ratings yet
- Final HandoutDocument3 pagesFinal HandoutCrisanta EstebanNo ratings yet
- TQM PDFDocument10 pagesTQM PDFDhanasekar TdsNo ratings yet
- ReviewerDocument5 pagesReviewerayaa caranzaNo ratings yet
- Strategic Plan Presentation - GPDocument15 pagesStrategic Plan Presentation - GPJohn AlfredNo ratings yet
- QA QC Microbiology ParasitologyDocument13 pagesQA QC Microbiology ParasitologyKristel S. BalismonNo ratings yet
- TQM U1 and U2 PDFDocument29 pagesTQM U1 and U2 PDFA. ShanmugamNo ratings yet
- Quality AssuranceDocument43 pagesQuality Assurancekanika100% (1)
- Continuous Improvement StrategyDocument14 pagesContinuous Improvement StrategyRamalingam ChandrasekharanNo ratings yet
- TQM Chapter 1-5Document25 pagesTQM Chapter 1-5Jashly ChavezNo ratings yet
- Lec 3 TQMDocument24 pagesLec 3 TQMWaleed AhmedNo ratings yet
- NLM - ControllingDocument8 pagesNLM - ControllingNa NaNo ratings yet
- Total Quality ManagementDocument106 pagesTotal Quality ManagementJohanna GutiérrezNo ratings yet
- P08 Assignment 2 - Team CDocument30 pagesP08 Assignment 2 - Team CCarlosNo ratings yet
- Self ch2 p2Document18 pagesSelf ch2 p2akypc9No ratings yet
- Whyme?: Pulkit Kapoor Solution DesignerDocument10 pagesWhyme?: Pulkit Kapoor Solution DesignerPulkit KapoorNo ratings yet
- Second ClassDocument48 pagesSecond ClassMartinus Golden SiteketaNo ratings yet
- Resumos GLODocument20 pagesResumos GLOSarah PereiraNo ratings yet
- Medical Equipment Quality Assurance For Healthcare FacilitiesDocument5 pagesMedical Equipment Quality Assurance For Healthcare FacilitiesJorge LopezNo ratings yet
- BSNA2010017BSNA Tiered Services All Domain Overview Brochure FINAL 1111Document6 pagesBSNA2010017BSNA Tiered Services All Domain Overview Brochure FINAL 1111MILAHN INDNo ratings yet
- Implementasi Mutu Pelayanan KesehatanDocument16 pagesImplementasi Mutu Pelayanan KesehatanrsmNo ratings yet
- Prinsip Dasar: Respect For PeopleDocument109 pagesPrinsip Dasar: Respect For PeopleoktavianNo ratings yet
- Help Us Spread The News: Cbd@royalcollege - CaDocument42 pagesHelp Us Spread The News: Cbd@royalcollege - CamochkurniawanNo ratings yet
- Finals LeadershipDocument30 pagesFinals LeadershipJeremiah Andre Poissonier AyupanNo ratings yet
- Total Quality Management in Healthcare Organizations An OverviewDocument37 pagesTotal Quality Management in Healthcare Organizations An OverviewmalathiNo ratings yet
- 9.1 Performance MeasurementDocument31 pages9.1 Performance MeasurementRoberto Carlos MUNOZ GUEVARANo ratings yet
- Quality Assurance With ModelDocument43 pagesQuality Assurance With ModelSamjhana NeupaneNo ratings yet
- CHAPTER 5 - QM in HospitalityDocument30 pagesCHAPTER 5 - QM in Hospitalitynndt05092003No ratings yet
- Total Quality ManagementDocument19 pagesTotal Quality ManagementVishal MeenaNo ratings yet
- Control: Correction & PreventionDocument13 pagesControl: Correction & PreventionRaj VermaNo ratings yet
- Ge8077 TQM Unit IV NotesDocument30 pagesGe8077 TQM Unit IV NotesTT GAMER VBKNo ratings yet
- TQMSix Sigma LeanDocument82 pagesTQMSix Sigma Leanamit kumarNo ratings yet
- Textile Quality Management Lecture For Mid and Final XamDocument176 pagesTextile Quality Management Lecture For Mid and Final XamebrahimbutexNo ratings yet
- Building Better Policies: The Nuts and Bolts of Monitoring and Evaluation SystemsFrom EverandBuilding Better Policies: The Nuts and Bolts of Monitoring and Evaluation SystemsNo ratings yet
- OSP FO WorkDocument50 pagesOSP FO WorkARCC2030No ratings yet
- GreenHouse ConstructionDocument30 pagesGreenHouse ConstructionYudha SatriaNo ratings yet
- 418-M1-Cu 5 Resp. Emergencies 2Document12 pages418-M1-Cu 5 Resp. Emergencies 2Paradillo Regatuna LesterNo ratings yet
- SurgTrnds MnmalInvsve InviteDocument2 pagesSurgTrnds MnmalInvsve Inviteanand787No ratings yet
- Epk İ ManuelDocument74 pagesEpk İ Manuelcevdet limanNo ratings yet
- Arteri LineDocument13 pagesArteri Linemuthia octavianaNo ratings yet
- Compliance PDFDocument20 pagesCompliance PDFSUBHANKAR PALNo ratings yet
- Fire Extinguishers QuizDocument2 pagesFire Extinguishers Quizapi-210017783No ratings yet
- MG Self Awareness PDFDocument1 pageMG Self Awareness PDFodescribdNo ratings yet
- Properties of Concrete 3.1 Properties of ConcreteDocument4 pagesProperties of Concrete 3.1 Properties of ConcreteErwin LipardoNo ratings yet
- 130201001M Ferritin 028120523 V1.0 EN 20120906Document4 pages130201001M Ferritin 028120523 V1.0 EN 20120906Nurhadi KebluksNo ratings yet
- Man#251 Rev BDocument10 pagesMan#251 Rev Bjuan dalmassoNo ratings yet
- Master'S Thesis: High-Temperature Compression Strength of High-Alumina Refractory Bricks Used in Rotary Kilns of LKABDocument64 pagesMaster'S Thesis: High-Temperature Compression Strength of High-Alumina Refractory Bricks Used in Rotary Kilns of LKABAyten CaputcuNo ratings yet
- Masters of The House (Fitch 8 June 2005) A Review of UK RMBS Master Trusts PDFDocument32 pagesMasters of The House (Fitch 8 June 2005) A Review of UK RMBS Master Trusts PDFfodriscollNo ratings yet
- New Biophilia Tracker x3 FeaturesDocument15 pagesNew Biophilia Tracker x3 FeaturesMartin Haynes100% (1)
- Work Safety Alert Pressed To Death by An Elevating Work PlatformDocument3 pagesWork Safety Alert Pressed To Death by An Elevating Work Platformhessian123No ratings yet
- Surgical Vacuum Drains: Types, Uses, and Complications: Rajaraman Durai, Philip C.H. NGDocument9 pagesSurgical Vacuum Drains: Types, Uses, and Complications: Rajaraman Durai, Philip C.H. NGLakshmi Mounica GrandhiNo ratings yet
- Gazet Notification For Establishment of OsmcDocument3 pagesGazet Notification For Establishment of OsmcprayasdansanaNo ratings yet
- Mrs. Annapurna TiwariDocument15 pagesMrs. Annapurna Tiwarikuruvagadda sagarNo ratings yet
- 181-CEN Fire Safety in Buildings - CEN TC 127Document4 pages181-CEN Fire Safety in Buildings - CEN TC 127Perie Anugraha Wiguna100% (1)
- CHEM 141 Lab 2 (Reactions) ProcedureDocument5 pagesCHEM 141 Lab 2 (Reactions) ProcedureKiersten RobertsNo ratings yet
- Hse FormDocument2 pagesHse FormPhilip Tcs100% (1)
- Literary Analysis The Last Wolf WolfDocument3 pagesLiterary Analysis The Last Wolf Wolfkaliprasad82No ratings yet
- City of Naga Scholar ProfileDocument2 pagesCity of Naga Scholar ProfileFaith James ServanoNo ratings yet
- Blood Clinical CorellaionsDocument12 pagesBlood Clinical Corellaionssinte beyuNo ratings yet
- PreparationsDocument8 pagesPreparationsAmbass EcohNo ratings yet
- Guide Falsework AustraliaDocument4 pagesGuide Falsework AustraliaHafizah MohdNo ratings yet
- Army TM 9-2320-289-20P Air Force To 36a12-1a-2084-1 Marine Corps TM 2320-20P/3Document724 pagesArmy TM 9-2320-289-20P Air Force To 36a12-1a-2084-1 Marine Corps TM 2320-20P/3Albaro AguirreNo ratings yet