Download as pptx, pdf, or txt
You might also like
- Neonatal Hypoglycemia September 2022Document30 pagesNeonatal Hypoglycemia September 2022f.abraham0% (1)
- Introduction, Concept of Child CareDocument42 pagesIntroduction, Concept of Child CareArchana80% (5)
- The Woman Speaks To The Man Who Has Employed Her SonDocument3 pagesThe Woman Speaks To The Man Who Has Employed Her SonSerena SulawammotNo ratings yet
- Nursing Management of Low Birth Weight Baby andDocument30 pagesNursing Management of Low Birth Weight Baby andArchana100% (2)
- History, Principle and Scope of CHNDocument39 pagesHistory, Principle and Scope of CHNArchana100% (2)
- My - Failure To ThriveDocument31 pagesMy - Failure To ThriveAuliaRahman100% (1)
- Management of LBW BabiesDocument67 pagesManagement of LBW BabiesEllen Angel100% (4)
- Child Health Nursing: Growth and DevelopmentDocument67 pagesChild Health Nursing: Growth and DevelopmentEllen Angel100% (4)
- Case Scenerio Nephrotic SyndromeDocument4 pagesCase Scenerio Nephrotic SyndromeEllen AngelNo ratings yet
- Lesson Plan Nephrotic SyndromeDocument9 pagesLesson Plan Nephrotic SyndromeEllen Angel50% (2)
- Case Scenerio Nephrotic SyndromeDocument4 pagesCase Scenerio Nephrotic SyndromeEllen AngelNo ratings yet
- Project Report On RTS Juice PlantDocument7 pagesProject Report On RTS Juice PlantEIRI Board of Consultants and PublishersNo ratings yet
- Infectious Disease Naplex QuestionsDocument3 pagesInfectious Disease Naplex QuestionsSARANYA0% (1)
- Kangaroo Mother CareDocument6 pagesKangaroo Mother Careabdullah khalid100% (1)
- Nursing Foundations-Basic BSC Nursing I Year Question Bank: Unit I Short AnswersDocument10 pagesNursing Foundations-Basic BSC Nursing I Year Question Bank: Unit I Short AnswersNilakshi Barik MandalNo ratings yet
- Master Rotation Plan of Anm 2ND YearDocument9 pagesMaster Rotation Plan of Anm 2ND Yearkuruvagadda sagar50% (2)
- Trends in The ObstetricsDocument12 pagesTrends in The ObstetricssuthaNo ratings yet
- Psychosocial and Cultural Aspects InpregnancyDocument2 pagesPsychosocial and Cultural Aspects InpregnancyKavitha p0% (1)
- Role of Pediatric Nurse in Child CareDocument4 pagesRole of Pediatric Nurse in Child Carevishnu100% (1)
- Nursing Care Plan FormatDocument7 pagesNursing Care Plan FormatPrasann RoyNo ratings yet
- Assignment On IMNCIDocument3 pagesAssignment On IMNCIcharanjit kaur100% (1)
- Border District Cluster StrategyDocument2 pagesBorder District Cluster StrategyRAJU100% (1)
- Diarrhea CPDocument8 pagesDiarrhea CPAsma SaleemNo ratings yet
- Course Title:-Child Health Nursing Topic: - Care of Newborn Duration: - 1 HR Venue: - Classroom A.V.Aids: - Ppts Date: - General Objectives: - Specific ObjectivesDocument9 pagesCourse Title:-Child Health Nursing Topic: - Care of Newborn Duration: - 1 HR Venue: - Classroom A.V.Aids: - Ppts Date: - General Objectives: - Specific ObjectivesBhawna Pandhu100% (1)
- Modern Concept of Child CareDocument14 pagesModern Concept of Child CareKiranNo ratings yet
- CHILD HEALTH NURSING Unit I Stuents Notes NotesDocument13 pagesCHILD HEALTH NURSING Unit I Stuents Notes Noteskarthicpraveen100% (2)
- Common Neonatal DisordersDocument71 pagesCommon Neonatal DisordersRANJIT GOGOI100% (3)
- Content: Subject: Child Health Nursing Specific Objectives AV Aids Evaluation Bibliography I 3Document7 pagesContent: Subject: Child Health Nursing Specific Objectives AV Aids Evaluation Bibliography I 3Anand BhawnaNo ratings yet
- Effect of Drug During Pregnancy, Labour and PuerperiumDocument10 pagesEffect of Drug During Pregnancy, Labour and PuerperiumSabeethu Girija63% (16)
- TOPIC - Management of Challenged ChildrenDocument20 pagesTOPIC - Management of Challenged ChildrenDinesh Khinchi75% (4)
- Fetal Distress Day 1Document16 pagesFetal Distress Day 1Bharat Thapa100% (1)
- Antenatal Care PPT EchyDocument14 pagesAntenatal Care PPT EchyYuliana alensi falloNo ratings yet
- Cont EduDocument18 pagesCont EduShilu Mathai PappachanNo ratings yet
- Unit 5 PPP CHN NDocument312 pagesUnit 5 PPP CHN NAnonymous hYMWbA100% (1)
- Unwed MotherDocument3 pagesUnwed Motherjasmine904677% (13)
- Normal PuerperiumDocument3 pagesNormal PuerperiumarunshreerajendranNo ratings yet
- Antenatal Preparation OBG - FOR BSC NURSING STUDENTSDocument22 pagesAntenatal Preparation OBG - FOR BSC NURSING STUDENTSKripa Susan100% (1)
- New Born AssessmentDocument42 pagesNew Born AssessmentBhawna Joshi100% (3)
- Assignment On Drugs Used For NewbornDocument11 pagesAssignment On Drugs Used For Newbornvarshasharma05100% (1)
- Lesson-Plan-Kangaroo-Mother CareDocument18 pagesLesson-Plan-Kangaroo-Mother CareG.Sangeetha bnch100% (1)
- Obg Nursing (Midwifery) Lab: S.No List of ArticlesDocument2 pagesObg Nursing (Midwifery) Lab: S.No List of ArticlesChakrapani Chaturvedi0% (1)
- Kangaroo Mother CareDocument12 pagesKangaroo Mother CareMary Menu100% (1)
- Seminar ON: Baby Friendly Hospital InitiativeDocument7 pagesSeminar ON: Baby Friendly Hospital InitiativeUmairah BashirNo ratings yet
- IMNCIDocument47 pagesIMNCIRenuga SureshNo ratings yet
- Assessment of Preschooler and SchoolerDocument49 pagesAssessment of Preschooler and SchoolerNancy SamuelNo ratings yet
- National Policy and Legislation in Relation To Child Health and WelfareDocument24 pagesNational Policy and Legislation in Relation To Child Health and Welfarerubinarashmi16100% (1)
- Female Pelvis and MeasurementsDocument21 pagesFemale Pelvis and MeasurementsBia KhanNo ratings yet
- Lesson Plan On PEM PDFDocument5 pagesLesson Plan On PEM PDFISLAMIC KNOWLEDGE BASED ON TRULY HADIS0% (1)
- Advanced Neonatal Procedure1Document14 pagesAdvanced Neonatal Procedure1Santhosh.S.U100% (1)
- Bfhi Lesson PlanDocument26 pagesBfhi Lesson Planbaby100% (2)
- Junevile DM Kel. 4Document7 pagesJunevile DM Kel. 4suci arleniaNo ratings yet
- Case Management of Ari at PHC LevelDocument29 pagesCase Management of Ari at PHC Levelapi-3823785No ratings yet
- KANGAROO MOTHER CARE ContentDocument6 pagesKANGAROO MOTHER CARE ContentAmy Lalringhluani Chhakchhuak100% (2)
- A Study To Evaluate The Effectiveness of Structured Teaching Program On Knowledge and Practice Regarding Kangaroo Mother Care Among Post Natal Mothers Having Low Birth Weight Babies 1Document9 pagesA Study To Evaluate The Effectiveness of Structured Teaching Program On Knowledge and Practice Regarding Kangaroo Mother Care Among Post Natal Mothers Having Low Birth Weight Babies 1Manisa ParidaNo ratings yet
- 1.3 Reactionof Ill Child To HospitalizationDocument21 pages1.3 Reactionof Ill Child To HospitalizationMUSLIHAH MD DESA100% (2)
- KMC FinalDocument36 pagesKMC FinalGandimarei100% (3)
- Artificial Feeding MethodsDocument9 pagesArtificial Feeding MethodsSAYMABANU100% (1)
- Assessment of A New Born PPT LPDocument35 pagesAssessment of A New Born PPT LPBaldwin Hamzcorp Hamoonga100% (1)
- Diagnosis of PregnancyDocument25 pagesDiagnosis of PregnancyA suhasiniNo ratings yet
- 6.1 Common Neonatal ProblemsDocument40 pages6.1 Common Neonatal ProblemsArchanaNo ratings yet
- THESIS CHN LBWDocument25 pagesTHESIS CHN LBWJessica Merilyn100% (1)
- Seminar ImnciDocument15 pagesSeminar Imnciseema devassy100% (1)
- Impact of Hospitalization & Nursing Care of Hospitalized ChildDocument42 pagesImpact of Hospitalization & Nursing Care of Hospitalized ChildRubina100% (2)
- Terminology CHNDocument4 pagesTerminology CHNKailash NagarNo ratings yet
- Nicu Physical LayoutDocument16 pagesNicu Physical LayoutMeena Koushal100% (5)
- Whooping Cough: Dr. MwendwaDocument39 pagesWhooping Cough: Dr. MwendwaAlvin OmondiNo ratings yet
- Human and Microbial InteractionDocument37 pagesHuman and Microbial Interactionnmadni827No ratings yet
- CD 1Document5 pagesCD 1Iriah Mara100% (1)
- Unit-I-INDIAN MENTAL HEALTH ACT 1987Document66 pagesUnit-I-INDIAN MENTAL HEALTH ACT 1987Ellen AngelNo ratings yet
- Case Scenerio GlomerulonephritisDocument4 pagesCase Scenerio GlomerulonephritisEllen AngelNo ratings yet
- Communicable Disease (MMR) (Autosaved)Document65 pagesCommunicable Disease (MMR) (Autosaved)Ellen AngelNo ratings yet
- Ellen Angellin Asst Prof Aimsr: Growth and Development in ChildrenDocument101 pagesEllen Angellin Asst Prof Aimsr: Growth and Development in ChildrenEllen AngelNo ratings yet
- Assessment of New BornDocument58 pagesAssessment of New BornEllen Angel100% (2)
- (PART-C) Cet-Unit V Principles of Education &teaching and Learning ProcessDocument40 pages(PART-C) Cet-Unit V Principles of Education &teaching and Learning ProcessEllen AngelNo ratings yet
- Communication and Nurse Patient Relationship: By, Ms. Ellen Angellin Assist Prof, AconcDocument114 pagesCommunication and Nurse Patient Relationship: By, Ms. Ellen Angellin Assist Prof, AconcEllen AngelNo ratings yet
- Curriculum Vitae: Mrs Augustine Ellen AngellinDocument3 pagesCurriculum Vitae: Mrs Augustine Ellen AngellinEllen AngelNo ratings yet
- CHN Practical Exam Growth and DevDocument16 pagesCHN Practical Exam Growth and DevEllen AngelNo ratings yet
- CVS - History CollectionDocument9 pagesCVS - History CollectionEllen AngelNo ratings yet
- Bowel Wash: Child Health Nursing ProcedureDocument4 pagesBowel Wash: Child Health Nursing ProcedureEllen Angel100% (1)
- World Down Syndrome Day 21 MARCH, 2021: The Apollo College of Nursing ChittoorDocument1 pageWorld Down Syndrome Day 21 MARCH, 2021: The Apollo College of Nursing ChittoorEllen AngelNo ratings yet
- Case Scenerio PneumoniaDocument8 pagesCase Scenerio PneumoniaEllen AngelNo ratings yet
- III YEAR Paed Reference RangesDocument5 pagesIII YEAR Paed Reference RangesEllen AngelNo ratings yet
- Case Scenerio HydrocephalusDocument9 pagesCase Scenerio HydrocephalusEllen AngelNo ratings yet
- Case Scenerio GlomerulonephritisDocument4 pagesCase Scenerio GlomerulonephritisEllen AngelNo ratings yet
- Lesson Plan Genito UrinaryDocument26 pagesLesson Plan Genito UrinaryEllen AngelNo ratings yet
- Neural Tube DefectDocument43 pagesNeural Tube DefectEllen AngelNo ratings yet
- Case Scenerio HydrocephalusDocument9 pagesCase Scenerio HydrocephalusEllen AngelNo ratings yet
- Child Health Nursing Unit-I: Nclex QuestionsDocument42 pagesChild Health Nursing Unit-I: Nclex QuestionsEllen AngelNo ratings yet
- Case Scenerio MENINGITISDocument10 pagesCase Scenerio MENINGITISEllen AngelNo ratings yet
- Unit - XI-Role of Nurse in Nutrition ProgrammeDocument82 pagesUnit - XI-Role of Nurse in Nutrition ProgrammeEllen AngelNo ratings yet
- Case Scenerio PneumoniaDocument10 pagesCase Scenerio PneumoniaEllen AngelNo ratings yet
- Public SpeakingDocument21 pagesPublic SpeakingEllen AngelNo ratings yet
- The Apollo College of Nursing Chittoor: Iii Year - Attendance Sheet S. No Name of The Student 03.09.2020Document2 pagesThe Apollo College of Nursing Chittoor: Iii Year - Attendance Sheet S. No Name of The Student 03.09.2020Ellen AngelNo ratings yet
- Dec. 4 2021 Bldg. Tech ReviewDocument58 pagesDec. 4 2021 Bldg. Tech Reviewadyjoy antonioNo ratings yet
- Dental Implant Site Preparation - A Review: C.J.Venkatakrishnan, S.Bhuminathan and Chitraa.R.ChandranDocument4 pagesDental Implant Site Preparation - A Review: C.J.Venkatakrishnan, S.Bhuminathan and Chitraa.R.ChandranLouis HutahaeanNo ratings yet
- Walking AidsDocument2 pagesWalking AidsSofia P. PanlilioNo ratings yet
- Sentinel Collim Rev1.2 CompressedDocument2 pagesSentinel Collim Rev1.2 CompressedBauyrzhanNo ratings yet
- PDS - CS - Form - No - 212 SHERLADocument8 pagesPDS - CS - Form - No - 212 SHERLASherla Catulay Godinez NautanNo ratings yet
- Environmental Geotechniques: Theories of Ion ExchangeDocument21 pagesEnvironmental Geotechniques: Theories of Ion ExchangeTenkurala srujanaNo ratings yet
- The Impact of Facebook Usage On Academic PerformanceDocument2 pagesThe Impact of Facebook Usage On Academic PerformanceChristine Tabada PanganibanNo ratings yet
- Reading ResponseDocument3 pagesReading ResponseJack SikoliaNo ratings yet
- Thermal Conductivity Measurement PDFDocument7 pagesThermal Conductivity Measurement PDFKalindaMadusankaDasanayakaNo ratings yet
- Piping SpecificationDocument5 pagesPiping SpecificationShandi Hasnul FarizalNo ratings yet
- OSH SeminarDocument2 pagesOSH SeminarSahar Ulu JeruasNo ratings yet
- Fantastic Four Drug For Heart FailureDocument47 pagesFantastic Four Drug For Heart FailurePutro Panji Asmoro BangunNo ratings yet
- Background of The StudyDocument13 pagesBackground of The Studyjeffrey rodriguezNo ratings yet
- Toothpaste Survey FormDocument1 pageToothpaste Survey FormBimalendu Konar50% (2)
- ECA DatabaseDocument22 pagesECA DatabaseRidhwan JamaludinNo ratings yet
- A Study On Occupational Hazards in Die Casting IndustriesDocument8 pagesA Study On Occupational Hazards in Die Casting IndustriesManik LakshmanNo ratings yet
- Model ETR-9200 Automatic Tuning Smarter Logic ControllerDocument26 pagesModel ETR-9200 Automatic Tuning Smarter Logic ControllervhelectronicaNo ratings yet
- Tehri DamDocument31 pagesTehri DamVinayakJindalNo ratings yet
- Bibliography Primary Sources: Books:: Marie-Curie-Speech - HTMLDocument11 pagesBibliography Primary Sources: Books:: Marie-Curie-Speech - HTMLapi-130099490No ratings yet
- PCB HandlingDocument8 pagesPCB HandlingscanlonlNo ratings yet
- DR Physique Lean Bulking Series II 2015Document121 pagesDR Physique Lean Bulking Series II 2015Vlad Alexandru50% (2)
- Waste Heat RecoveryDocument37 pagesWaste Heat Recoveryommech2020No ratings yet
- Biosolids EpaDocument13 pagesBiosolids EpaKhansa HapsariNo ratings yet
- Surgical Operation PDFDocument64 pagesSurgical Operation PDFshifna.latheefNo ratings yet
- Jedec Standard: Els ServiçosDocument18 pagesJedec Standard: Els ServiçosEverton LuizNo ratings yet
- Expense 12-18 Agustus 2022Document4 pagesExpense 12-18 Agustus 2022Rizal RisqiNo ratings yet
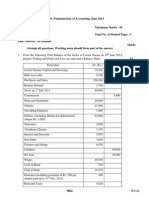
- Capinew Account June13Document7 pagesCapinew Account June13ashwinNo ratings yet