
Diabetic Neuropathy
Diabetic Neuropathy
You might also like
- CPAR DLL 2NDDocument2 pagesCPAR DLL 2NDFelyn DelaCruz - Dalino100% (16)
- GRAHAM, Daniel. Heraclitus As A Process PhilosopherDocument8 pagesGRAHAM, Daniel. Heraclitus As A Process PhilosopherVitor Ferreira LimaNo ratings yet
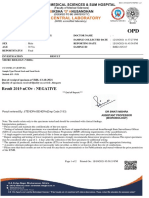
- Patient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusDocument2 pagesPatient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusThushar P kumarNo ratings yet
- Electro Neurological Eductor Treatment For Peripheral NeuropathyDocument36 pagesElectro Neurological Eductor Treatment For Peripheral NeuropathyClaudio Marcelo Naddeo100% (2)
- Hypoglycemia BrochureDocument3 pagesHypoglycemia BrochureAkira Pongchad BNo ratings yet
- Cranial Nerve Affections of Diabetes MellitesDocument5 pagesCranial Nerve Affections of Diabetes Mellitessalsabiilabdel16No ratings yet
- Diabetic NeuropathyDocument26 pagesDiabetic NeuropathySuwandewi PutriNo ratings yet
- A Neurology Unit Presentation BY Duru Chinonso Elizabeth: Diabetic NeuropathyDocument32 pagesA Neurology Unit Presentation BY Duru Chinonso Elizabeth: Diabetic NeuropathyChidube UkachukwuNo ratings yet
- Diabetic Neuropathies: The Nerve Damage of DiabetesDocument12 pagesDiabetic Neuropathies: The Nerve Damage of DiabetestaqiedaNo ratings yet
- Diabetic Neuropathies: Prepared byDocument24 pagesDiabetic Neuropathies: Prepared bymaria_magno_6No ratings yet
- Diabetic Neuropathy: DR Shahjada SelimDocument129 pagesDiabetic Neuropathy: DR Shahjada SelimmadboyNo ratings yet
- 15 Causes of Burning in The FeetDocument6 pages15 Causes of Burning in The Feetfausto omioNo ratings yet
- Diabetic NeuropathyDocument28 pagesDiabetic Neuropathyaslam deshmukhNo ratings yet
- What Is Diabetes Mellitus?Document9 pagesWhat Is Diabetes Mellitus?Nhoel RsNo ratings yet
- Diabetes: Diabetic NeuropathyDocument3 pagesDiabetes: Diabetic NeuropathysasirtrNo ratings yet
- Diabetes: Complications of Diabetes: The most important information you need to improve your healthFrom EverandDiabetes: Complications of Diabetes: The most important information you need to improve your healthNo ratings yet
- Diabetic Neuropathy: Amithbabu.C.B Mscd-EndoDocument19 pagesDiabetic Neuropathy: Amithbabu.C.B Mscd-EndoDR.AMITHBABU.C.BNo ratings yet
- Secondary Health 7 q4 Module3Document13 pagesSecondary Health 7 q4 Module3Rona RuizNo ratings yet
- Diabetic NeuropathyDocument24 pagesDiabetic NeuropathyAlbari Pohan100% (1)
- Multiple Sclerosis MS Demyelinating DiseaseDocument11 pagesMultiple Sclerosis MS Demyelinating DiseaseAtie AlinaNo ratings yet
- Reporting ScienceDocument20 pagesReporting ScienceYasuhiro Hinggo EscobilloNo ratings yet
- What Is Diabetic Neuropathy: Treatment For Related DeficiencyDocument6 pagesWhat Is Diabetic Neuropathy: Treatment For Related DeficiencyCarl MacCordNo ratings yet
- Diabetic NeuropathyDocument25 pagesDiabetic Neuropathyvirgil_thomas100% (1)
- VertigoDocument25 pagesVertigoFayhaa NadeemNo ratings yet
- Diabetic Neuropathy: Did You Know?Document2 pagesDiabetic Neuropathy: Did You Know?Pallavi JagtapNo ratings yet
- Burhani Medical Idara (Diabetes Management)Document8 pagesBurhani Medical Idara (Diabetes Management)Burhanuddin TinNo ratings yet
- CKD-CHF ScriptDocument5 pagesCKD-CHF ScriptAirglow GNo ratings yet
- Type 1 DiabetesDocument7 pagesType 1 DiabetesEimor PortezNo ratings yet
- Cardivascular Deseases and Diabetes MellitusDocument38 pagesCardivascular Deseases and Diabetes MellitusSyafiqah SabriNo ratings yet
- Pangasinan State University College of Nursing: Bayambang Campus Bayambang, PangasinanDocument8 pagesPangasinan State University College of Nursing: Bayambang Campus Bayambang, PangasinanferdzNo ratings yet
- ملازم الباطنية (عملي)Document84 pagesملازم الباطنية (عملي)ملكة الجنوبNo ratings yet
- Systemic Lupus ErythematosusDocument25 pagesSystemic Lupus ErythematosusdaliaNo ratings yet
- Multiple SclerosisDocument6 pagesMultiple SclerosisATHRUN93G8No ratings yet
- Case Study For Lupus ErythematousDocument4 pagesCase Study For Lupus ErythematousGabbii CincoNo ratings yet
- TYPE 2 Diabetes Mellitus ProjectDocument11 pagesTYPE 2 Diabetes Mellitus Projecthumaidali saiyedNo ratings yet
- Day2Understanding Common Medical ConditionDocument15 pagesDay2Understanding Common Medical ConditionRidwan OlivaNo ratings yet
- Foundation of NeuropathyDocument20 pagesFoundation of NeuropathyBoogii BoogNo ratings yet
- List of Problems The Patient HasDocument5 pagesList of Problems The Patient HasKiruba SelvamNo ratings yet
- All About diabetes-LORENZDocument9 pagesAll About diabetes-LORENZdaryl gomezNo ratings yet
- Disease Manifestations and PathologyDocument34 pagesDisease Manifestations and PathologyAnjali TakkeNo ratings yet
- Nerve Pain and Nerve Damage 2Document17 pagesNerve Pain and Nerve Damage 2Ryan BediNo ratings yet
- PuneetDocument11 pagesPuneetRudraksha pratap singhNo ratings yet
- Diabetic Neuropathy - Clinical and ManagementDocument58 pagesDiabetic Neuropathy - Clinical and ManagementChristian ThamNo ratings yet
- Proximal Diabetic NeuropathyDocument2 pagesProximal Diabetic NeuropathyMirna Busatlic ZeljkovicNo ratings yet
- Diabetic Neuropathy: - Aarthi A Bot 3 Year SriherDocument54 pagesDiabetic Neuropathy: - Aarthi A Bot 3 Year SriherAarthi ArumugamNo ratings yet
- Kidney FailureDocument8 pagesKidney FailureКатя ДементьеваNo ratings yet
- 005 - Lecture - Diabetiс neuropathyDocument37 pages005 - Lecture - Diabetiс neuropathyLucas Victor AlmeidaNo ratings yet
- Hypokinetic DiseasesDocument5 pagesHypokinetic DiseasesMartha BelayNo ratings yet
- Diabetes Power PointDocument21 pagesDiabetes Power Pointpmak0116No ratings yet
- Blood GlucoseDocument12 pagesBlood Glucosehajidah hassanalNo ratings yet
- Clinpha 2 Sas 3Document9 pagesClinpha 2 Sas 3kateNo ratings yet
- Diseases & Precautions NotesDocument23 pagesDiseases & Precautions NotesrajnandeyneysNo ratings yet
- Type 2 Diabetes MellitusDocument6 pagesType 2 Diabetes MellitusJoy NisoladaNo ratings yet
- M SclerosisDocument10 pagesM SclerosisWillieNo ratings yet
- MigraineDocument16 pagesMigraineBheru LalNo ratings yet
- What Are The Symptoms of Kidney Failure?Document3 pagesWhat Are The Symptoms of Kidney Failure?Jarda julie DacuagNo ratings yet
- Multiple SclerosisDocument3 pagesMultiple Sclerosisapi-3822433No ratings yet
- DIABETIC FOOT PAIN by Kenneth B. Rehm DPMDocument11 pagesDIABETIC FOOT PAIN by Kenneth B. Rehm DPMAshish RajeNo ratings yet
- Chronic Kidney DiseaseDocument7 pagesChronic Kidney Diseasekzbreakerr100% (1)
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The Complete Guide to Type 1 Diabetes: Symptoms, Risks, Treatments and Support for DiabeticsFrom EverandThe Complete Guide to Type 1 Diabetes: Symptoms, Risks, Treatments and Support for DiabeticsNo ratings yet
- Neuropathy Unveiled: Understanding and Managing Diabetic Nerve DamageFrom EverandNeuropathy Unveiled: Understanding and Managing Diabetic Nerve DamageNo ratings yet
- Diabetes Mellitus And Its Complications, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetes Mellitus And Its Complications, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- PT Diamond Food Indonesia Tbk. Dan Entitas AnakDocument45 pagesPT Diamond Food Indonesia Tbk. Dan Entitas AnakIrsyad KamalNo ratings yet
- A1 English Listening Test - What Is Your JobDocument6 pagesA1 English Listening Test - What Is Your JobTrang NguyenNo ratings yet
- Transcendentalism UnitDocument14 pagesTranscendentalism Unitapi-402466117No ratings yet
- Perfect Failure: Commencement Address To Graduating Class of The Buckley School June 10, 2009Document13 pagesPerfect Failure: Commencement Address To Graduating Class of The Buckley School June 10, 2009eodumont9981No ratings yet
- Course Plan - MathEng5-MDocument3 pagesCourse Plan - MathEng5-MLorman MaylasNo ratings yet
- Meet What Name: 1 Saying HelloDocument2 pagesMeet What Name: 1 Saying HelloNaiki Huaman AlegreNo ratings yet
- The Steak N Shake Company Code of Business Conduct and EthicsDocument16 pagesThe Steak N Shake Company Code of Business Conduct and Ethicsapi-355261274No ratings yet
- Bing Pas Ganjil 2022-2023Document8 pagesBing Pas Ganjil 2022-2023karci ardianyNo ratings yet
- Effectiveness of Poco-Poco Exercise On Elderly's Cholesterol Levels: A Preliminary StudyDocument10 pagesEffectiveness of Poco-Poco Exercise On Elderly's Cholesterol Levels: A Preliminary StudyAli FirdausNo ratings yet
- Cardinal Bernadin SEAMLESS GARMENTDocument5 pagesCardinal Bernadin SEAMLESS GARMENTMike LewisNo ratings yet
- Upload 2Document15 pagesUpload 2Akash VermaNo ratings yet
- 2) There Was A Murder Last Night. What Were They Doing When The Murder Happened?Document2 pages2) There Was A Murder Last Night. What Were They Doing When The Murder Happened?Pilar Gonzalez PinillaNo ratings yet
- Selection and Grading of ContentDocument36 pagesSelection and Grading of ContentAli Gamil100% (1)
- Heikin AshiChartsRDocument3 pagesHeikin AshiChartsRif1313100% (2)
- Chapter2 PDFDocument88 pagesChapter2 PDFVanwesly Prayoga100% (1)
- Chandhassu Recognizer For Telugu PoemsDocument10 pagesChandhassu Recognizer For Telugu PoemsentrencherNo ratings yet
- Being Aware of Being Aware (The - RUPERT SPIRA (Lido)Document78 pagesBeing Aware of Being Aware (The - RUPERT SPIRA (Lido)Izac Souza71% (7)
- Unfinished Movie Script "Call of The Sea"Document3 pagesUnfinished Movie Script "Call of The Sea"Typo ProteccNo ratings yet
- Csat Mantra: CSAT Made Easy and AffordableDocument2 pagesCsat Mantra: CSAT Made Easy and AffordableMisti AcharjeeNo ratings yet
- Meenakshi Sundararajan Engineering College: Department of Information TechnologyDocument7 pagesMeenakshi Sundararajan Engineering College: Department of Information Technology5052 - UTHRA .TNo ratings yet
- Electromagnetic Fields: ECEG 2210 ECEG 2210Document13 pagesElectromagnetic Fields: ECEG 2210 ECEG 2210jemalNo ratings yet
- Steps TNG 7 KishDocument19 pagesSteps TNG 7 KishSheetanshu AgarwalNo ratings yet
- Wa0008.Document2 pagesWa0008.innocentmakawa3No ratings yet
- Instant Download Ebook PDF Engineering Mechanics Statics 9th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Engineering Mechanics Statics 9th Edition PDF Scribdmanuel.king142100% (54)
- 11 History Notes 04 Central Islamic LandsDocument9 pages11 History Notes 04 Central Islamic LandsPrisha NijhawanNo ratings yet
- What Are Some Process in Your Everyday Life That Requires A Scientific MethodDocument2 pagesWhat Are Some Process in Your Everyday Life That Requires A Scientific Methodlaica andalNo ratings yet























































































Download as pptx, pdf, or txt
You might also like
- CPAR DLL 2NDDocument2 pagesCPAR DLL 2NDFelyn DelaCruz - Dalino100% (16)
- GRAHAM, Daniel. Heraclitus As A Process PhilosopherDocument8 pagesGRAHAM, Daniel. Heraclitus As A Process PhilosopherVitor Ferreira LimaNo ratings yet
- Patient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusDocument2 pagesPatient Name Doctor Name Pat Reg Id Sample Collected Date SEX Reporting Date AGE Sample Id ReportstatusThushar P kumarNo ratings yet
- Electro Neurological Eductor Treatment For Peripheral NeuropathyDocument36 pagesElectro Neurological Eductor Treatment For Peripheral NeuropathyClaudio Marcelo Naddeo100% (2)
- Hypoglycemia BrochureDocument3 pagesHypoglycemia BrochureAkira Pongchad BNo ratings yet
- Cranial Nerve Affections of Diabetes MellitesDocument5 pagesCranial Nerve Affections of Diabetes Mellitessalsabiilabdel16No ratings yet
- Diabetic NeuropathyDocument26 pagesDiabetic NeuropathySuwandewi PutriNo ratings yet
- A Neurology Unit Presentation BY Duru Chinonso Elizabeth: Diabetic NeuropathyDocument32 pagesA Neurology Unit Presentation BY Duru Chinonso Elizabeth: Diabetic NeuropathyChidube UkachukwuNo ratings yet
- Diabetic Neuropathies: The Nerve Damage of DiabetesDocument12 pagesDiabetic Neuropathies: The Nerve Damage of DiabetestaqiedaNo ratings yet
- Diabetic Neuropathies: Prepared byDocument24 pagesDiabetic Neuropathies: Prepared bymaria_magno_6No ratings yet
- Diabetic Neuropathy: DR Shahjada SelimDocument129 pagesDiabetic Neuropathy: DR Shahjada SelimmadboyNo ratings yet
- 15 Causes of Burning in The FeetDocument6 pages15 Causes of Burning in The Feetfausto omioNo ratings yet
- Diabetic NeuropathyDocument28 pagesDiabetic Neuropathyaslam deshmukhNo ratings yet
- What Is Diabetes Mellitus?Document9 pagesWhat Is Diabetes Mellitus?Nhoel RsNo ratings yet
- Diabetes: Diabetic NeuropathyDocument3 pagesDiabetes: Diabetic NeuropathysasirtrNo ratings yet
- Diabetes: Complications of Diabetes: The most important information you need to improve your healthFrom EverandDiabetes: Complications of Diabetes: The most important information you need to improve your healthNo ratings yet
- Diabetic Neuropathy: Amithbabu.C.B Mscd-EndoDocument19 pagesDiabetic Neuropathy: Amithbabu.C.B Mscd-EndoDR.AMITHBABU.C.BNo ratings yet
- Secondary Health 7 q4 Module3Document13 pagesSecondary Health 7 q4 Module3Rona RuizNo ratings yet
- Diabetic NeuropathyDocument24 pagesDiabetic NeuropathyAlbari Pohan100% (1)
- Multiple Sclerosis MS Demyelinating DiseaseDocument11 pagesMultiple Sclerosis MS Demyelinating DiseaseAtie AlinaNo ratings yet
- Reporting ScienceDocument20 pagesReporting ScienceYasuhiro Hinggo EscobilloNo ratings yet
- What Is Diabetic Neuropathy: Treatment For Related DeficiencyDocument6 pagesWhat Is Diabetic Neuropathy: Treatment For Related DeficiencyCarl MacCordNo ratings yet
- Diabetic NeuropathyDocument25 pagesDiabetic Neuropathyvirgil_thomas100% (1)
- VertigoDocument25 pagesVertigoFayhaa NadeemNo ratings yet
- Diabetic Neuropathy: Did You Know?Document2 pagesDiabetic Neuropathy: Did You Know?Pallavi JagtapNo ratings yet
- Burhani Medical Idara (Diabetes Management)Document8 pagesBurhani Medical Idara (Diabetes Management)Burhanuddin TinNo ratings yet
- CKD-CHF ScriptDocument5 pagesCKD-CHF ScriptAirglow GNo ratings yet
- Type 1 DiabetesDocument7 pagesType 1 DiabetesEimor PortezNo ratings yet
- Cardivascular Deseases and Diabetes MellitusDocument38 pagesCardivascular Deseases and Diabetes MellitusSyafiqah SabriNo ratings yet
- Pangasinan State University College of Nursing: Bayambang Campus Bayambang, PangasinanDocument8 pagesPangasinan State University College of Nursing: Bayambang Campus Bayambang, PangasinanferdzNo ratings yet
- ملازم الباطنية (عملي)Document84 pagesملازم الباطنية (عملي)ملكة الجنوبNo ratings yet
- Systemic Lupus ErythematosusDocument25 pagesSystemic Lupus ErythematosusdaliaNo ratings yet
- Multiple SclerosisDocument6 pagesMultiple SclerosisATHRUN93G8No ratings yet
- Case Study For Lupus ErythematousDocument4 pagesCase Study For Lupus ErythematousGabbii CincoNo ratings yet
- TYPE 2 Diabetes Mellitus ProjectDocument11 pagesTYPE 2 Diabetes Mellitus Projecthumaidali saiyedNo ratings yet
- Day2Understanding Common Medical ConditionDocument15 pagesDay2Understanding Common Medical ConditionRidwan OlivaNo ratings yet
- Foundation of NeuropathyDocument20 pagesFoundation of NeuropathyBoogii BoogNo ratings yet
- List of Problems The Patient HasDocument5 pagesList of Problems The Patient HasKiruba SelvamNo ratings yet
- All About diabetes-LORENZDocument9 pagesAll About diabetes-LORENZdaryl gomezNo ratings yet
- Disease Manifestations and PathologyDocument34 pagesDisease Manifestations and PathologyAnjali TakkeNo ratings yet
- Nerve Pain and Nerve Damage 2Document17 pagesNerve Pain and Nerve Damage 2Ryan BediNo ratings yet
- PuneetDocument11 pagesPuneetRudraksha pratap singhNo ratings yet
- Diabetic Neuropathy - Clinical and ManagementDocument58 pagesDiabetic Neuropathy - Clinical and ManagementChristian ThamNo ratings yet
- Proximal Diabetic NeuropathyDocument2 pagesProximal Diabetic NeuropathyMirna Busatlic ZeljkovicNo ratings yet
- Diabetic Neuropathy: - Aarthi A Bot 3 Year SriherDocument54 pagesDiabetic Neuropathy: - Aarthi A Bot 3 Year SriherAarthi ArumugamNo ratings yet
- Kidney FailureDocument8 pagesKidney FailureКатя ДементьеваNo ratings yet
- 005 - Lecture - Diabetiс neuropathyDocument37 pages005 - Lecture - Diabetiс neuropathyLucas Victor AlmeidaNo ratings yet
- Hypokinetic DiseasesDocument5 pagesHypokinetic DiseasesMartha BelayNo ratings yet
- Diabetes Power PointDocument21 pagesDiabetes Power Pointpmak0116No ratings yet
- Blood GlucoseDocument12 pagesBlood Glucosehajidah hassanalNo ratings yet
- Clinpha 2 Sas 3Document9 pagesClinpha 2 Sas 3kateNo ratings yet
- Diseases & Precautions NotesDocument23 pagesDiseases & Precautions NotesrajnandeyneysNo ratings yet
- Type 2 Diabetes MellitusDocument6 pagesType 2 Diabetes MellitusJoy NisoladaNo ratings yet
- M SclerosisDocument10 pagesM SclerosisWillieNo ratings yet
- MigraineDocument16 pagesMigraineBheru LalNo ratings yet
- What Are The Symptoms of Kidney Failure?Document3 pagesWhat Are The Symptoms of Kidney Failure?Jarda julie DacuagNo ratings yet
- Multiple SclerosisDocument3 pagesMultiple Sclerosisapi-3822433No ratings yet
- DIABETIC FOOT PAIN by Kenneth B. Rehm DPMDocument11 pagesDIABETIC FOOT PAIN by Kenneth B. Rehm DPMAshish RajeNo ratings yet
- Chronic Kidney DiseaseDocument7 pagesChronic Kidney Diseasekzbreakerr100% (1)
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The Complete Guide to Type 1 Diabetes: Symptoms, Risks, Treatments and Support for DiabeticsFrom EverandThe Complete Guide to Type 1 Diabetes: Symptoms, Risks, Treatments and Support for DiabeticsNo ratings yet
- Neuropathy Unveiled: Understanding and Managing Diabetic Nerve DamageFrom EverandNeuropathy Unveiled: Understanding and Managing Diabetic Nerve DamageNo ratings yet
- Diabetes Mellitus And Its Complications, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetes Mellitus And Its Complications, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- PT Diamond Food Indonesia Tbk. Dan Entitas AnakDocument45 pagesPT Diamond Food Indonesia Tbk. Dan Entitas AnakIrsyad KamalNo ratings yet
- A1 English Listening Test - What Is Your JobDocument6 pagesA1 English Listening Test - What Is Your JobTrang NguyenNo ratings yet
- Transcendentalism UnitDocument14 pagesTranscendentalism Unitapi-402466117No ratings yet
- Perfect Failure: Commencement Address To Graduating Class of The Buckley School June 10, 2009Document13 pagesPerfect Failure: Commencement Address To Graduating Class of The Buckley School June 10, 2009eodumont9981No ratings yet
- Course Plan - MathEng5-MDocument3 pagesCourse Plan - MathEng5-MLorman MaylasNo ratings yet
- Meet What Name: 1 Saying HelloDocument2 pagesMeet What Name: 1 Saying HelloNaiki Huaman AlegreNo ratings yet
- The Steak N Shake Company Code of Business Conduct and EthicsDocument16 pagesThe Steak N Shake Company Code of Business Conduct and Ethicsapi-355261274No ratings yet
- Bing Pas Ganjil 2022-2023Document8 pagesBing Pas Ganjil 2022-2023karci ardianyNo ratings yet
- Effectiveness of Poco-Poco Exercise On Elderly's Cholesterol Levels: A Preliminary StudyDocument10 pagesEffectiveness of Poco-Poco Exercise On Elderly's Cholesterol Levels: A Preliminary StudyAli FirdausNo ratings yet
- Cardinal Bernadin SEAMLESS GARMENTDocument5 pagesCardinal Bernadin SEAMLESS GARMENTMike LewisNo ratings yet
- Upload 2Document15 pagesUpload 2Akash VermaNo ratings yet
- 2) There Was A Murder Last Night. What Were They Doing When The Murder Happened?Document2 pages2) There Was A Murder Last Night. What Were They Doing When The Murder Happened?Pilar Gonzalez PinillaNo ratings yet
- Selection and Grading of ContentDocument36 pagesSelection and Grading of ContentAli Gamil100% (1)
- Heikin AshiChartsRDocument3 pagesHeikin AshiChartsRif1313100% (2)
- Chapter2 PDFDocument88 pagesChapter2 PDFVanwesly Prayoga100% (1)
- Chandhassu Recognizer For Telugu PoemsDocument10 pagesChandhassu Recognizer For Telugu PoemsentrencherNo ratings yet
- Being Aware of Being Aware (The - RUPERT SPIRA (Lido)Document78 pagesBeing Aware of Being Aware (The - RUPERT SPIRA (Lido)Izac Souza71% (7)
- Unfinished Movie Script "Call of The Sea"Document3 pagesUnfinished Movie Script "Call of The Sea"Typo ProteccNo ratings yet
- Csat Mantra: CSAT Made Easy and AffordableDocument2 pagesCsat Mantra: CSAT Made Easy and AffordableMisti AcharjeeNo ratings yet
- Meenakshi Sundararajan Engineering College: Department of Information TechnologyDocument7 pagesMeenakshi Sundararajan Engineering College: Department of Information Technology5052 - UTHRA .TNo ratings yet
- Electromagnetic Fields: ECEG 2210 ECEG 2210Document13 pagesElectromagnetic Fields: ECEG 2210 ECEG 2210jemalNo ratings yet
- Steps TNG 7 KishDocument19 pagesSteps TNG 7 KishSheetanshu AgarwalNo ratings yet
- Wa0008.Document2 pagesWa0008.innocentmakawa3No ratings yet
- Instant Download Ebook PDF Engineering Mechanics Statics 9th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Engineering Mechanics Statics 9th Edition PDF Scribdmanuel.king142100% (54)
- 11 History Notes 04 Central Islamic LandsDocument9 pages11 History Notes 04 Central Islamic LandsPrisha NijhawanNo ratings yet
- What Are Some Process in Your Everyday Life That Requires A Scientific MethodDocument2 pagesWhat Are Some Process in Your Everyday Life That Requires A Scientific Methodlaica andalNo ratings yet