Download as pptx, pdf, or txt
You might also like
- 0011 Exam Paper Final 2020Document4 pages0011 Exam Paper Final 2020jasmin mayNo ratings yet
- Listening To The News 3 - Answer KeyDocument8 pagesListening To The News 3 - Answer KeyPhu Vo HoangNo ratings yet
- ArbovirusesDocument74 pagesArbovirusesmulatumelese100% (1)
- Topnotch Ent Supplement Handout Updated April 2016pdf PDFDocument15 pagesTopnotch Ent Supplement Handout Updated April 2016pdf PDFKenneth NuñezNo ratings yet
- Management of ShockDocument18 pagesManagement of ShockObongsamuel IdiongNo ratings yet
- 2-Hemorrhagic and Hypovolemic ShockDocument37 pages2-Hemorrhagic and Hypovolemic ShockRashif AnbiaNo ratings yet
- DR Anuj Raj BijukchheDocument95 pagesDR Anuj Raj BijukchheMUHAMMAD JAWAD HASSANNo ratings yet
- USMLE Step 1 in Final YearDocument33 pagesUSMLE Step 1 in Final YearsehrishNo ratings yet
- Diagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaDocument51 pagesDiagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaHilmaNo ratings yet
- 2011 ABCs of ShockDocument67 pages2011 ABCs of ShockMatthew CanipeNo ratings yet
- Abcs of Shock: Pediatric Critical Care Medicine Emory University Children'S Healthcare of AtlantaDocument67 pagesAbcs of Shock: Pediatric Critical Care Medicine Emory University Children'S Healthcare of AtlantaZEMENAY TRUNEHNo ratings yet
- NSG 117 PerfusionDocument55 pagesNSG 117 PerfusionAnonymous UJEyEsNo ratings yet
- Rian Nandika Hafsah Suadaul Adzro Nurhayati NufusDocument35 pagesRian Nandika Hafsah Suadaul Adzro Nurhayati NufusHilmiMawaddiAhmadNo ratings yet
- III. Modul 6 - SyokDocument81 pagesIII. Modul 6 - SyoksridhaniNo ratings yet
- Shock: Ron Michael N. Olaguera 2 Year Surgery ResidentDocument40 pagesShock: Ron Michael N. Olaguera 2 Year Surgery ResidentErick Anca100% (2)
- Shock: Rose Ann J. Raquiza-Perante Post Graduate InternDocument53 pagesShock: Rose Ann J. Raquiza-Perante Post Graduate InternRose Ann RaquizaNo ratings yet
- How To Recognize and Manage Pediatric Shock-WorkshopDocument36 pagesHow To Recognize and Manage Pediatric Shock-WorkshopMukhamad Arif MunandarNo ratings yet
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDocument64 pagesShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruNo ratings yet
- 1 ShockDocument59 pages1 ShockmeghaNo ratings yet
- Shock & It's ManagementDocument64 pagesShock & It's ManagementPallavi SinghNo ratings yet
- Shock 22Document29 pagesShock 22Erina NopiyantiNo ratings yet
- Classification of Hemorrhage & Hemorrhagic Shock (Handout)Document10 pagesClassification of Hemorrhage & Hemorrhagic Shock (Handout)Ayuub AbdirizakNo ratings yet
- Syok Hypovolemik-IH FK UMSU2012Document45 pagesSyok Hypovolemik-IH FK UMSU2012Ratika Ayu PiliangNo ratings yet
- Shock: Dr. P. Manoj Kumar Asst. Professor, Dep. of Gen. Surgery, CaimsDocument61 pagesShock: Dr. P. Manoj Kumar Asst. Professor, Dep. of Gen. Surgery, CaimsManoj Kumar PasunooriNo ratings yet
- Shock: in Multiple InjuryDocument32 pagesShock: in Multiple InjuryNazirul HanifNo ratings yet
- ShockDocument48 pagesShockanon-7341200% (2)
- MTE Diagnosis and Manag ShockDocument52 pagesMTE Diagnosis and Manag ShockGarbha JmrsNo ratings yet
- Multi SistemDocument19 pagesMulti SistemciptaarynNo ratings yet
- Shock: Deepa Murali Ms IvDocument59 pagesShock: Deepa Murali Ms Ivdee0212No ratings yet
- Final SHOCKDocument44 pagesFinal SHOCKAbas AhmedNo ratings yet
- Stages of ShockDocument13 pagesStages of ShockA. P.No ratings yet
- Shock: Presenters-Selahadin Awol - Yohannes TekuDocument88 pagesShock: Presenters-Selahadin Awol - Yohannes TekuYaniNo ratings yet
- Shock: Agus Setiyana, M.D. Cardiac Anesthetist Acls Provider Fccs Provider Atls ProviderDocument39 pagesShock: Agus Setiyana, M.D. Cardiac Anesthetist Acls Provider Fccs Provider Atls ProvidersheiraNo ratings yet
- III. Modul 6 - SyokDocument81 pagesIII. Modul 6 - SyokGrace Noviyanthi SinambelaNo ratings yet
- ShockDocument60 pagesShock180045No ratings yet
- Obstetric Shock 21.11.08Document53 pagesObstetric Shock 21.11.08Jabed Ahmed100% (1)
- ShockDocument86 pagesShockmeadwaiet1999No ratings yet
- Shock and Its Management: Presented byDocument72 pagesShock and Its Management: Presented bysheme171150% (2)
- 418 Septic Shock Sirs and ModsDocument51 pages418 Septic Shock Sirs and ModsApril Ann HortilanoNo ratings yet
- Shock: Syahbuddin HarahapDocument41 pagesShock: Syahbuddin Harahapprima suci angrainiNo ratings yet
- Shock: Departemen Anestesiologi Dan Reanimasi Fakultas Kedokteran USUDocument54 pagesShock: Departemen Anestesiologi Dan Reanimasi Fakultas Kedokteran USURuki HartawanNo ratings yet
- Acute Kideny Injury and Chronic Renal FailureDocument55 pagesAcute Kideny Injury and Chronic Renal FailurehisslNo ratings yet
- Shock 2Document23 pagesShock 2ViviViviNo ratings yet
- Syock & ManagementDocument34 pagesSyock & ManagementIndra Anwari RukmanNo ratings yet
- ShockDocument70 pagesShockDawit g/kidanNo ratings yet
- Shock Syndromes: Chapter 18Document11 pagesShock Syndromes: Chapter 18Marvel BloomNo ratings yet
- SHOCK LEC Modified (2nd)Document86 pagesSHOCK LEC Modified (2nd)spanishthingz01No ratings yet
- UW Notes - 8 - Endocrine ArrangeddDocument40 pagesUW Notes - 8 - Endocrine Arrangeddmind blocNo ratings yet
- Shock: Dr. Vijayendra Kumar Presented byDocument31 pagesShock: Dr. Vijayendra Kumar Presented byphani5747No ratings yet
- Presented by Nithish ReddyDocument41 pagesPresented by Nithish ReddyNithish ReddyNo ratings yet
- Shock and HemorhhageDocument84 pagesShock and HemorhhagePoova RagavanNo ratings yet
- Diagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaDocument49 pagesDiagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaSiti rahmawatiNo ratings yet
- Shock DR Sadia Hussain: Assistant Professor Pediatric Medicine King Edward Medical University LahoreDocument22 pagesShock DR Sadia Hussain: Assistant Professor Pediatric Medicine King Edward Medical University LahoreTouseef Ur RehmanNo ratings yet
- Banan Harbi Lana Sbitan: Done By: Zaid Abu-Ameerah Mohammad AlotaibiDocument32 pagesBanan Harbi Lana Sbitan: Done By: Zaid Abu-Ameerah Mohammad AlotaibiSarahNo ratings yet
- Chapter54 Shock Critical 2Document21 pagesChapter54 Shock Critical 2asma barhoomNo ratings yet
- Shock 141543 Downloable 1402764Document12 pagesShock 141543 Downloable 1402764Kskbd BajaibwNo ratings yet
- Lecture 6-ShockDocument5 pagesLecture 6-ShockMadiha MadiNo ratings yet
- Management Hypovolemic Shock, NurinDocument12 pagesManagement Hypovolemic Shock, Nurinرفاعي آكرمNo ratings yet
- Lecture Presentation For Clinical 1 StudentsDocument43 pagesLecture Presentation For Clinical 1 Studentskirubel deribNo ratings yet
- Penatalaksanaan SyokDocument59 pagesPenatalaksanaan SyokArif NurfadhilahNo ratings yet
- Last Lesson, We Have Studied The Features and The Mechanism of Microcirculatory Ischemic Hypoxia During Shock - Now ContinueDocument27 pagesLast Lesson, We Have Studied The Features and The Mechanism of Microcirculatory Ischemic Hypoxia During Shock - Now Continueapi-19916399No ratings yet
- Handout 5 CardioVascular System Overview PDFDocument7 pagesHandout 5 CardioVascular System Overview PDFGrape JuiceNo ratings yet
- Final Hidden Scars Lhow Violence Harms The Mental Health of ChildrenDocument52 pagesFinal Hidden Scars Lhow Violence Harms The Mental Health of ChildrensofiabloemNo ratings yet
- Bab 9 Ergonomi Di Tempat KerjaDocument91 pagesBab 9 Ergonomi Di Tempat KerjaardhabariqNo ratings yet
- Teaching Orgasm For Females With Chronic Anorgasmia Using The Betty Dodson MethodDocument14 pagesTeaching Orgasm For Females With Chronic Anorgasmia Using The Betty Dodson MethodAntares1973100% (1)
- Discover Your DietDocument51 pagesDiscover Your DietAkanksha SinghNo ratings yet
- Lesson Plan 9 Grade Jag 2019Document22 pagesLesson Plan 9 Grade Jag 2019Astrid GomezNo ratings yet
- 2017 - Strategy Brick Production BangladeshffDocument41 pages2017 - Strategy Brick Production BangladeshffNaeem QasimNo ratings yet
- Obesities Controversies in DiagnosisDocument20 pagesObesities Controversies in DiagnosisLuIz ZooZaNo ratings yet
- Clinical Protocol in Pediatrics, 2012Document96 pagesClinical Protocol in Pediatrics, 2012floare de colt100% (1)
- Impact of Mindfulness Katherine WeareDocument12 pagesImpact of Mindfulness Katherine WeareMeek El100% (1)
- Normal Laboratory ValuesDocument8 pagesNormal Laboratory ValuesStephanieNo ratings yet
- 4th Shifting Micro Lab ReviewerDocument154 pages4th Shifting Micro Lab ReviewerJade MonrealNo ratings yet
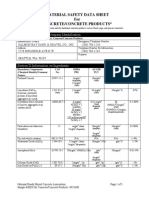
- Material Safety Data Sheet For Concrete/Concrete Products : Section I-Product and Company IdentificationDocument5 pagesMaterial Safety Data Sheet For Concrete/Concrete Products : Section I-Product and Company Identificationmalaya tripathyNo ratings yet
- FINAL CASE STUDY With ROS, P.E. & Health ImplementDocument36 pagesFINAL CASE STUDY With ROS, P.E. & Health ImplementteuuuuNo ratings yet
- 65wd17e Rev1 TBActionPlan 150588 Withcover PDFDocument17 pages65wd17e Rev1 TBActionPlan 150588 Withcover PDFFlorentina LucanNo ratings yet
- First Aid Powerpoint SASDocument50 pagesFirst Aid Powerpoint SASMahmoud HalimNo ratings yet
- FM Pi-Xiv - InddDocument2,766 pagesFM Pi-Xiv - InddPhát NguyễnNo ratings yet
- Test FPSC For The Post VODocument4 pagesTest FPSC For The Post VOSajjad LaghariNo ratings yet
- Optometry: Accommodative and Binocular Dysfunctions: Prevalence in A Randomised Sample of University StudentsDocument9 pagesOptometry: Accommodative and Binocular Dysfunctions: Prevalence in A Randomised Sample of University StudentsShyannaNo ratings yet
- Apraxia Capi LibroDocument30 pagesApraxia Capi LibroNinoska OrtizNo ratings yet
- B.inggris Covid 19 DimassDocument3 pagesB.inggris Covid 19 DimassDimas frasetyoNo ratings yet
- Sohail Reports PDFDocument2 pagesSohail Reports PDFMunazza SohailNo ratings yet
- CP Acute Renal Failure Chap7Document128 pagesCP Acute Renal Failure Chap7Katherine 'Chingboo' Leonico LaudNo ratings yet
- Nutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsDocument15 pagesNutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsIOSRjournalNo ratings yet
- Histology ReviewerDocument7 pagesHistology ReviewerJulius FrondaNo ratings yet
- Systemic Lupus Erythematosus: Pathophysiology I Health 210 Final Project May 12, 2011Document7 pagesSystemic Lupus Erythematosus: Pathophysiology I Health 210 Final Project May 12, 2011Chris WheatNo ratings yet
- MacMaster and Toronto Rheumatoid Arthritis Patient Preference Disability Questionnaire MACTARDocument2 pagesMacMaster and Toronto Rheumatoid Arthritis Patient Preference Disability Questionnaire MACTARramesh babu100% (1)