
External Fixator in Orthopaedics and Traumatology
External Fixator in Orthopaedics and Traumatology
You might also like
- Principles and Techniques for the Aspiring Surgeon: What Great Surgeons Do Without ThinkingFrom EverandPrinciples and Techniques for the Aspiring Surgeon: What Great Surgeons Do Without ThinkingNo ratings yet
- AORF Textbook of Orthopaedics: African Orthopaedic Research Foundation (AORF) EditionFrom EverandAORF Textbook of Orthopaedics: African Orthopaedic Research Foundation (AORF) EditionRating: 3 out of 5 stars3/5 (2)
- Miles Operation - Abdominoperineal Excision - Rectal CADocument5 pagesMiles Operation - Abdominoperineal Excision - Rectal CASpencer DempseyNo ratings yet
- Healthcare MemoDocument4 pagesHealthcare MemoAustin DunlapNo ratings yet
- Salter Harris - DAK (Ortho UNS)Document23 pagesSalter Harris - DAK (Ortho UNS)DitaAnggaraKusumaNo ratings yet
- Spine TraumaDocument7 pagesSpine TraumafadlinNo ratings yet
- Day Case Surgery SajeebDocument34 pagesDay Case Surgery SajeebMahbubur Rahman0% (1)
- 18th Orl-Hns Congress 23 August 2019 PDFDocument262 pages18th Orl-Hns Congress 23 August 2019 PDFWahyu Tri Novriansyah HastonNo ratings yet
- Stoma Types PDFDocument1 pageStoma Types PDFUmi Kalsum100% (1)
- External Fixation of FemurDocument27 pagesExternal Fixation of FemurMemoona AmeerNo ratings yet
- External FixationDocument4 pagesExternal FixationZilbran BerontaxNo ratings yet
- Principles and Management of Acute Orthopaedic Trauma: Third EditionFrom EverandPrinciples and Management of Acute Orthopaedic Trauma: Third EditionNo ratings yet
- Prinicple of External FixatorDocument29 pagesPrinicple of External FixatorAnkit KarkiNo ratings yet
- 7 - Surgical FlapsDocument31 pages7 - Surgical FlapsAssssss100% (1)
- External Fixator PDFDocument2 pagesExternal Fixator PDFBrandon0% (1)
- A Comprehensive Guide On OsteotomyDocument3 pagesA Comprehensive Guide On OsteotomySiora SurgicalsNo ratings yet
- Ankle FractureDocument11 pagesAnkle FracturecorsaruNo ratings yet
- Approach To Fracture BoneDocument46 pagesApproach To Fracture BoneMuhaimin Noor AzharNo ratings yet
- Workshop 1: Knots: Stage 1Document4 pagesWorkshop 1: Knots: Stage 1Noora jabeenNo ratings yet
- Principles in Fracture ManagementDocument60 pagesPrinciples in Fracture ManagementNge NgeNo ratings yet
- AmputationDocument51 pagesAmputationStar CruiseNo ratings yet
- Ortho CompetencesDocument31 pagesOrtho CompetencesHamad ElmoghrabeNo ratings yet
- Ankel Heel PainDocument51 pagesAnkel Heel PainMeno Ali100% (1)
- Pelvic FracturesDocument8 pagesPelvic FracturesArif AbubakarNo ratings yet
- Gamma NailDocument49 pagesGamma NailMihaela HerghelegiuNo ratings yet
- SJAMS 43B 750 754 Thesis Tibial PlateauDocument5 pagesSJAMS 43B 750 754 Thesis Tibial PlateauNisheshJainNo ratings yet
- Knee 2Document152 pagesKnee 2Laura ChiforNo ratings yet
- SPINAL AnaesthesiaDocument54 pagesSPINAL Anaesthesiadarsh bhattiNo ratings yet
- Dams Class Notes OrthopedicsDocument93 pagesDams Class Notes OrthopedicsAnkitNo ratings yet
- AAOS Trauma 2012Document92 pagesAAOS Trauma 2012Aps CnjNo ratings yet
- Pathological Fracture 1Document38 pagesPathological Fracture 1Wan Muhammad Mulkan0% (1)
- Surgical Complications of Minor Oral SurgeryDocument53 pagesSurgical Complications of Minor Oral SurgeryDrNagendra Dutt Sharma100% (1)
- 4-Conservative Treatment FX, CastingDocument53 pages4-Conservative Treatment FX, CastingMuhammad TaqwaNo ratings yet
- Pelvic FracturesDocument58 pagesPelvic Fracturesshammasbm100% (10)
- General SurgeryDocument11 pagesGeneral Surgeryhuzaifa usmanNo ratings yet
- Tissue Repair: Kristine Krafts, M.D. - September 13, 2010Document59 pagesTissue Repair: Kristine Krafts, M.D. - September 13, 2010Antonino CassottaNo ratings yet
- External Fixation: Nursing Best Practice GuidelinesDocument25 pagesExternal Fixation: Nursing Best Practice GuidelinesDoneva Lyn MedinaNo ratings yet
- Treatment of Diaphyseal Femoral Fractures With Ilizarov Frame. Maurizio A. Catagni and Francesco GuerreschiDocument4 pagesTreatment of Diaphyseal Femoral Fractures With Ilizarov Frame. Maurizio A. Catagni and Francesco GuerreschiNuno Craveiro LopesNo ratings yet
- Tibial Plateau FractureDocument5 pagesTibial Plateau FracturezonadianNo ratings yet
- SC - Fracture ZMHDocument51 pagesSC - Fracture ZMHMis StromNo ratings yet
- New Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauDocument8 pagesNew Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauCosmina BribanNo ratings yet
- ASiT Yearbook 2010, Association of Surgeons in Training PDFDocument131 pagesASiT Yearbook 2010, Association of Surgeons in Training PDFEd FitzgeraldNo ratings yet
- Fractures and Dislocations About The Elbow in The Pediatric PatientDocument65 pagesFractures and Dislocations About The Elbow in The Pediatric PatientPeter HubkaNo ratings yet
- WEBINAR On PEDIATRIC TRAUMADocument44 pagesWEBINAR On PEDIATRIC TRAUMAGovindarajan Hariharan100% (1)
- Amputation, Surgery and RehabilitationDocument46 pagesAmputation, Surgery and RehabilitationPatrick WandellahNo ratings yet
- Technique of Reduction and Fixation of Unicondylar Medial Hoffa FracturDocument5 pagesTechnique of Reduction and Fixation of Unicondylar Medial Hoffa Fracturaesculapius100% (1)
- Orthopaedic SplintingDocument52 pagesOrthopaedic SplintingandhitaNo ratings yet
- Ulcer: DR - Sunil Kumar Asst - Professor Dept - of Gen - Surgery MNR Medical College Sangareddy 01-05-2019Document83 pagesUlcer: DR - Sunil Kumar Asst - Professor Dept - of Gen - Surgery MNR Medical College Sangareddy 01-05-2019Aashmi ChandrikaaNo ratings yet
- FR Distal HumerusDocument55 pagesFR Distal Humerusiisscribd100% (1)
- Cast and Splint Immobilization - Complications PDFDocument11 pagesCast and Splint Immobilization - Complications PDFcronoss21No ratings yet
- Definition of Damage Control OrthopaedicsDocument2 pagesDefinition of Damage Control OrthopaedicsHerryanto Agustriadi100% (1)
- Boa Lower Limb 2009Document24 pagesBoa Lower Limb 2009Hengki Permana PutraNo ratings yet
- Non Operative Fracture Management: Splint and CastDocument78 pagesNon Operative Fracture Management: Splint and CastSaeda AhmedNo ratings yet
- Open Jejunostomy: Steven J. Hughes, MD and A. James Moser, MDDocument8 pagesOpen Jejunostomy: Steven J. Hughes, MD and A. James Moser, MDAndres BernalNo ratings yet
- MS Obst & GynaeDocument77 pagesMS Obst & GynaeAmna MunawarNo ratings yet
- Surgical DressingDocument60 pagesSurgical DressingJeffri syaputraNo ratings yet
- Local Anesthesia Techniques PDFDocument12 pagesLocal Anesthesia Techniques PDFhalimNo ratings yet
- Basic Plastic Surgery Techniques and Principles: How To SutureDocument3 pagesBasic Plastic Surgery Techniques and Principles: How To SutureDarryl BettsNo ratings yet
- Percutaneous Imaging-Guided Spinal Facet Joint InjectionsDocument6 pagesPercutaneous Imaging-Guided Spinal Facet Joint InjectionsAlvaro Perez HenriquezNo ratings yet
- A Disease Study On: AppendectomyDocument8 pagesA Disease Study On: Appendectomybryan leguiabNo ratings yet
- Biopsy: Reza Fu Rqon SDocument25 pagesBiopsy: Reza Fu Rqon SNovli ArdiansyahNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- First Aid Broken BoneDocument11 pagesFirst Aid Broken BoneRodo SilvaNo ratings yet
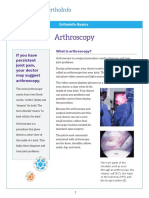
- Arthroscopy: If You Have Persistent Joint Pain, Your Doctor May Suggest ArthrosDocument4 pagesArthroscopy: If You Have Persistent Joint Pain, Your Doctor May Suggest ArthrosCaty RamosNo ratings yet
- Bhamashah Swasthya Bima Yojana 2017-19: S. No. Final Package Name Package Type Proposed Rate Speciality Code Short NameDocument21 pagesBhamashah Swasthya Bima Yojana 2017-19: S. No. Final Package Name Package Type Proposed Rate Speciality Code Short Nameswastik hospitalNo ratings yet
- Captain America's Shield GenioplastyDocument3 pagesCaptain America's Shield GenioplastyVarun bharathi100% (1)
- Logbook For Post GraduateDocument8 pagesLogbook For Post GraduateNabeil SufyanNo ratings yet
- 05 Trauma CareDocument4 pages05 Trauma CareKUMUTHA MALAR A/P PARMESWARANNo ratings yet
- Effect of Vol Pre Miccional para La Medicion Del VPMDocument4 pagesEffect of Vol Pre Miccional para La Medicion Del VPMAlejandro JImenez PatiñoNo ratings yet
- Checklist Instrumen Baksos Update 28.05.23Document8 pagesChecklist Instrumen Baksos Update 28.05.23dr GheaNo ratings yet
- Kebutuhan Alat Alat AnestesiDocument5 pagesKebutuhan Alat Alat AnestesiidrisNo ratings yet
- Consolidated List of NDMC HospitalDocument12 pagesConsolidated List of NDMC HospitalgargatworkNo ratings yet
- Daftar Pustaka Du 3Document2 pagesDaftar Pustaka Du 3devikomalaNo ratings yet
- C Should Cosmetic Surgery Be Banned?: Print This Page Discuss TopicDocument7 pagesC Should Cosmetic Surgery Be Banned?: Print This Page Discuss TopicHarith ZakuanNo ratings yet
- Department of Plastic and Reconstructive Surgery, Hospital Pulau Pinang November 2015 Oncall RosterDocument2 pagesDepartment of Plastic and Reconstructive Surgery, Hospital Pulau Pinang November 2015 Oncall RostermohdfaridbaharomNo ratings yet
- AU Ortho Journal PDFDocument436 pagesAU Ortho Journal PDFadithyaram011549No ratings yet
- Ekstrofia BuliDocument1 pageEkstrofia Buliahmadzaki80No ratings yet
- Stratamed For PatientsDocument2 pagesStratamed For PatientsTechtureGNo ratings yet
- Surgeon Should Learn Not Just How To Operate But How To Create System of CareDocument26 pagesSurgeon Should Learn Not Just How To Operate But How To Create System of Careamal.fathullahNo ratings yet
- Department of SurgeryDocument2 pagesDepartment of SurgeryAr Jay100% (1)
- Anaesthetic Challenges in Complex Maxillofacial Trauma - ADocument18 pagesAnaesthetic Challenges in Complex Maxillofacial Trauma - APraveen RamasamyNo ratings yet
- Hospital Document List of Procedures For ANHDocument16 pagesHospital Document List of Procedures For ANHsrisaravanan67% (3)
- Heent LabDocument11 pagesHeent Labapi-743783774No ratings yet
- Resume Alireza MohammadzadehDocument2 pagesResume Alireza Mohammadzadeharian tejaratNo ratings yet
- AssesmentofoutcomeDocument8 pagesAssesmentofoutcomebhushan adhariNo ratings yet
- Northwestern Medicine Cystoscopy NMHDocument3 pagesNorthwestern Medicine Cystoscopy NMHCentanarianNo ratings yet
- Monitoring Bedah Handover Dan Aldrade Score JanuariDocument27 pagesMonitoring Bedah Handover Dan Aldrade Score JanuaridevikesdamNo ratings yet
- General Urology Question and Answer ItemsDocument13 pagesGeneral Urology Question and Answer ItemsalaamorsyNo ratings yet
- NHS UK Distension, Manipulation Under Anaesthetic and Arthroscopic Capsular ReleaseDocument3 pagesNHS UK Distension, Manipulation Under Anaesthetic and Arthroscopic Capsular ReleasemertNo ratings yet
- Sept 2017 List Panel HospitalDocument76 pagesSept 2017 List Panel HospitalApakElBuheiriGetbNo ratings yet
























































































Download as ppt, pdf, or txt
You might also like
- Principles and Techniques for the Aspiring Surgeon: What Great Surgeons Do Without ThinkingFrom EverandPrinciples and Techniques for the Aspiring Surgeon: What Great Surgeons Do Without ThinkingNo ratings yet
- AORF Textbook of Orthopaedics: African Orthopaedic Research Foundation (AORF) EditionFrom EverandAORF Textbook of Orthopaedics: African Orthopaedic Research Foundation (AORF) EditionRating: 3 out of 5 stars3/5 (2)
- Miles Operation - Abdominoperineal Excision - Rectal CADocument5 pagesMiles Operation - Abdominoperineal Excision - Rectal CASpencer DempseyNo ratings yet
- Healthcare MemoDocument4 pagesHealthcare MemoAustin DunlapNo ratings yet
- Salter Harris - DAK (Ortho UNS)Document23 pagesSalter Harris - DAK (Ortho UNS)DitaAnggaraKusumaNo ratings yet
- Spine TraumaDocument7 pagesSpine TraumafadlinNo ratings yet
- Day Case Surgery SajeebDocument34 pagesDay Case Surgery SajeebMahbubur Rahman0% (1)
- 18th Orl-Hns Congress 23 August 2019 PDFDocument262 pages18th Orl-Hns Congress 23 August 2019 PDFWahyu Tri Novriansyah HastonNo ratings yet
- Stoma Types PDFDocument1 pageStoma Types PDFUmi Kalsum100% (1)
- External Fixation of FemurDocument27 pagesExternal Fixation of FemurMemoona AmeerNo ratings yet
- External FixationDocument4 pagesExternal FixationZilbran BerontaxNo ratings yet
- Principles and Management of Acute Orthopaedic Trauma: Third EditionFrom EverandPrinciples and Management of Acute Orthopaedic Trauma: Third EditionNo ratings yet
- Prinicple of External FixatorDocument29 pagesPrinicple of External FixatorAnkit KarkiNo ratings yet
- 7 - Surgical FlapsDocument31 pages7 - Surgical FlapsAssssss100% (1)
- External Fixator PDFDocument2 pagesExternal Fixator PDFBrandon0% (1)
- A Comprehensive Guide On OsteotomyDocument3 pagesA Comprehensive Guide On OsteotomySiora SurgicalsNo ratings yet
- Ankle FractureDocument11 pagesAnkle FracturecorsaruNo ratings yet
- Approach To Fracture BoneDocument46 pagesApproach To Fracture BoneMuhaimin Noor AzharNo ratings yet
- Workshop 1: Knots: Stage 1Document4 pagesWorkshop 1: Knots: Stage 1Noora jabeenNo ratings yet
- Principles in Fracture ManagementDocument60 pagesPrinciples in Fracture ManagementNge NgeNo ratings yet
- AmputationDocument51 pagesAmputationStar CruiseNo ratings yet
- Ortho CompetencesDocument31 pagesOrtho CompetencesHamad ElmoghrabeNo ratings yet
- Ankel Heel PainDocument51 pagesAnkel Heel PainMeno Ali100% (1)
- Pelvic FracturesDocument8 pagesPelvic FracturesArif AbubakarNo ratings yet
- Gamma NailDocument49 pagesGamma NailMihaela HerghelegiuNo ratings yet
- SJAMS 43B 750 754 Thesis Tibial PlateauDocument5 pagesSJAMS 43B 750 754 Thesis Tibial PlateauNisheshJainNo ratings yet
- Knee 2Document152 pagesKnee 2Laura ChiforNo ratings yet
- SPINAL AnaesthesiaDocument54 pagesSPINAL Anaesthesiadarsh bhattiNo ratings yet
- Dams Class Notes OrthopedicsDocument93 pagesDams Class Notes OrthopedicsAnkitNo ratings yet
- AAOS Trauma 2012Document92 pagesAAOS Trauma 2012Aps CnjNo ratings yet
- Pathological Fracture 1Document38 pagesPathological Fracture 1Wan Muhammad Mulkan0% (1)
- Surgical Complications of Minor Oral SurgeryDocument53 pagesSurgical Complications of Minor Oral SurgeryDrNagendra Dutt Sharma100% (1)
- 4-Conservative Treatment FX, CastingDocument53 pages4-Conservative Treatment FX, CastingMuhammad TaqwaNo ratings yet
- Pelvic FracturesDocument58 pagesPelvic Fracturesshammasbm100% (10)
- General SurgeryDocument11 pagesGeneral Surgeryhuzaifa usmanNo ratings yet
- Tissue Repair: Kristine Krafts, M.D. - September 13, 2010Document59 pagesTissue Repair: Kristine Krafts, M.D. - September 13, 2010Antonino CassottaNo ratings yet
- External Fixation: Nursing Best Practice GuidelinesDocument25 pagesExternal Fixation: Nursing Best Practice GuidelinesDoneva Lyn MedinaNo ratings yet
- Treatment of Diaphyseal Femoral Fractures With Ilizarov Frame. Maurizio A. Catagni and Francesco GuerreschiDocument4 pagesTreatment of Diaphyseal Femoral Fractures With Ilizarov Frame. Maurizio A. Catagni and Francesco GuerreschiNuno Craveiro LopesNo ratings yet
- Tibial Plateau FractureDocument5 pagesTibial Plateau FracturezonadianNo ratings yet
- SC - Fracture ZMHDocument51 pagesSC - Fracture ZMHMis StromNo ratings yet
- New Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauDocument8 pagesNew Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauCosmina BribanNo ratings yet
- ASiT Yearbook 2010, Association of Surgeons in Training PDFDocument131 pagesASiT Yearbook 2010, Association of Surgeons in Training PDFEd FitzgeraldNo ratings yet
- Fractures and Dislocations About The Elbow in The Pediatric PatientDocument65 pagesFractures and Dislocations About The Elbow in The Pediatric PatientPeter HubkaNo ratings yet
- WEBINAR On PEDIATRIC TRAUMADocument44 pagesWEBINAR On PEDIATRIC TRAUMAGovindarajan Hariharan100% (1)
- Amputation, Surgery and RehabilitationDocument46 pagesAmputation, Surgery and RehabilitationPatrick WandellahNo ratings yet
- Technique of Reduction and Fixation of Unicondylar Medial Hoffa FracturDocument5 pagesTechnique of Reduction and Fixation of Unicondylar Medial Hoffa Fracturaesculapius100% (1)
- Orthopaedic SplintingDocument52 pagesOrthopaedic SplintingandhitaNo ratings yet
- Ulcer: DR - Sunil Kumar Asst - Professor Dept - of Gen - Surgery MNR Medical College Sangareddy 01-05-2019Document83 pagesUlcer: DR - Sunil Kumar Asst - Professor Dept - of Gen - Surgery MNR Medical College Sangareddy 01-05-2019Aashmi ChandrikaaNo ratings yet
- FR Distal HumerusDocument55 pagesFR Distal Humerusiisscribd100% (1)
- Cast and Splint Immobilization - Complications PDFDocument11 pagesCast and Splint Immobilization - Complications PDFcronoss21No ratings yet
- Definition of Damage Control OrthopaedicsDocument2 pagesDefinition of Damage Control OrthopaedicsHerryanto Agustriadi100% (1)
- Boa Lower Limb 2009Document24 pagesBoa Lower Limb 2009Hengki Permana PutraNo ratings yet
- Non Operative Fracture Management: Splint and CastDocument78 pagesNon Operative Fracture Management: Splint and CastSaeda AhmedNo ratings yet
- Open Jejunostomy: Steven J. Hughes, MD and A. James Moser, MDDocument8 pagesOpen Jejunostomy: Steven J. Hughes, MD and A. James Moser, MDAndres BernalNo ratings yet
- MS Obst & GynaeDocument77 pagesMS Obst & GynaeAmna MunawarNo ratings yet
- Surgical DressingDocument60 pagesSurgical DressingJeffri syaputraNo ratings yet
- Local Anesthesia Techniques PDFDocument12 pagesLocal Anesthesia Techniques PDFhalimNo ratings yet
- Basic Plastic Surgery Techniques and Principles: How To SutureDocument3 pagesBasic Plastic Surgery Techniques and Principles: How To SutureDarryl BettsNo ratings yet
- Percutaneous Imaging-Guided Spinal Facet Joint InjectionsDocument6 pagesPercutaneous Imaging-Guided Spinal Facet Joint InjectionsAlvaro Perez HenriquezNo ratings yet
- A Disease Study On: AppendectomyDocument8 pagesA Disease Study On: Appendectomybryan leguiabNo ratings yet
- Biopsy: Reza Fu Rqon SDocument25 pagesBiopsy: Reza Fu Rqon SNovli ArdiansyahNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- First Aid Broken BoneDocument11 pagesFirst Aid Broken BoneRodo SilvaNo ratings yet
- Arthroscopy: If You Have Persistent Joint Pain, Your Doctor May Suggest ArthrosDocument4 pagesArthroscopy: If You Have Persistent Joint Pain, Your Doctor May Suggest ArthrosCaty RamosNo ratings yet
- Bhamashah Swasthya Bima Yojana 2017-19: S. No. Final Package Name Package Type Proposed Rate Speciality Code Short NameDocument21 pagesBhamashah Swasthya Bima Yojana 2017-19: S. No. Final Package Name Package Type Proposed Rate Speciality Code Short Nameswastik hospitalNo ratings yet
- Captain America's Shield GenioplastyDocument3 pagesCaptain America's Shield GenioplastyVarun bharathi100% (1)
- Logbook For Post GraduateDocument8 pagesLogbook For Post GraduateNabeil SufyanNo ratings yet
- 05 Trauma CareDocument4 pages05 Trauma CareKUMUTHA MALAR A/P PARMESWARANNo ratings yet
- Effect of Vol Pre Miccional para La Medicion Del VPMDocument4 pagesEffect of Vol Pre Miccional para La Medicion Del VPMAlejandro JImenez PatiñoNo ratings yet
- Checklist Instrumen Baksos Update 28.05.23Document8 pagesChecklist Instrumen Baksos Update 28.05.23dr GheaNo ratings yet
- Kebutuhan Alat Alat AnestesiDocument5 pagesKebutuhan Alat Alat AnestesiidrisNo ratings yet
- Consolidated List of NDMC HospitalDocument12 pagesConsolidated List of NDMC HospitalgargatworkNo ratings yet
- Daftar Pustaka Du 3Document2 pagesDaftar Pustaka Du 3devikomalaNo ratings yet
- C Should Cosmetic Surgery Be Banned?: Print This Page Discuss TopicDocument7 pagesC Should Cosmetic Surgery Be Banned?: Print This Page Discuss TopicHarith ZakuanNo ratings yet
- Department of Plastic and Reconstructive Surgery, Hospital Pulau Pinang November 2015 Oncall RosterDocument2 pagesDepartment of Plastic and Reconstructive Surgery, Hospital Pulau Pinang November 2015 Oncall RostermohdfaridbaharomNo ratings yet
- AU Ortho Journal PDFDocument436 pagesAU Ortho Journal PDFadithyaram011549No ratings yet
- Ekstrofia BuliDocument1 pageEkstrofia Buliahmadzaki80No ratings yet
- Stratamed For PatientsDocument2 pagesStratamed For PatientsTechtureGNo ratings yet
- Surgeon Should Learn Not Just How To Operate But How To Create System of CareDocument26 pagesSurgeon Should Learn Not Just How To Operate But How To Create System of Careamal.fathullahNo ratings yet
- Department of SurgeryDocument2 pagesDepartment of SurgeryAr Jay100% (1)
- Anaesthetic Challenges in Complex Maxillofacial Trauma - ADocument18 pagesAnaesthetic Challenges in Complex Maxillofacial Trauma - APraveen RamasamyNo ratings yet
- Hospital Document List of Procedures For ANHDocument16 pagesHospital Document List of Procedures For ANHsrisaravanan67% (3)
- Heent LabDocument11 pagesHeent Labapi-743783774No ratings yet
- Resume Alireza MohammadzadehDocument2 pagesResume Alireza Mohammadzadeharian tejaratNo ratings yet
- AssesmentofoutcomeDocument8 pagesAssesmentofoutcomebhushan adhariNo ratings yet
- Northwestern Medicine Cystoscopy NMHDocument3 pagesNorthwestern Medicine Cystoscopy NMHCentanarianNo ratings yet
- Monitoring Bedah Handover Dan Aldrade Score JanuariDocument27 pagesMonitoring Bedah Handover Dan Aldrade Score JanuaridevikesdamNo ratings yet
- General Urology Question and Answer ItemsDocument13 pagesGeneral Urology Question and Answer ItemsalaamorsyNo ratings yet
- NHS UK Distension, Manipulation Under Anaesthetic and Arthroscopic Capsular ReleaseDocument3 pagesNHS UK Distension, Manipulation Under Anaesthetic and Arthroscopic Capsular ReleasemertNo ratings yet
- Sept 2017 List Panel HospitalDocument76 pagesSept 2017 List Panel HospitalApakElBuheiriGetbNo ratings yet