
Hypothyrodism in Pregnancy
Hypothyrodism in Pregnancy
You might also like
- Test Bank For Goulds Pathophysiology For The Health Professions 7th Edition by Van Meter 9780323792882 Test BankDocument9 pagesTest Bank For Goulds Pathophysiology For The Health Professions 7th Edition by Van Meter 9780323792882 Test Bankmohamed arbi taifNo ratings yet
- Antidepressant & Psychedelic Drug Interaction ChartDocument3 pagesAntidepressant & Psychedelic Drug Interaction ChartFred The Nomad100% (2)
- Thyroid Disease in PregnancyDocument53 pagesThyroid Disease in PregnancyTee Wei SianNo ratings yet
- Hypothyroidism and Pregnancy Vol.2Document9 pagesHypothyroidism and Pregnancy Vol.2RakhiNo ratings yet
- Abnormal Thyroid Function in PregnancyDocument54 pagesAbnormal Thyroid Function in Pregnancyasri khazaliNo ratings yet
- Thyroid CasesDocument61 pagesThyroid CasesHamoud AlshehriNo ratings yet
- Tiroid Pada KehamilanDocument56 pagesTiroid Pada Kehamilanpeni_dwi100% (1)
- Hypothyroidism in AdultsDocument95 pagesHypothyroidism in AdultsJULIO FLORESNo ratings yet
- Hypothyroidism in PregnancyDocument14 pagesHypothyroidism in PregnancyShajia ZafarNo ratings yet
- Endocrine Pathology Associated With Pregnancy Dr. Yunus TanggoDocument60 pagesEndocrine Pathology Associated With Pregnancy Dr. Yunus TanggoReni AstutiNo ratings yet
- Preconception Counseling For Thyroid DisordersDocument7 pagesPreconception Counseling For Thyroid DisordersLiya AnjelinaNo ratings yet
- Good Clinical Practice Advice: Thyroid and PregnancyDocument5 pagesGood Clinical Practice Advice: Thyroid and Pregnancyjuan carlos pradaNo ratings yet
- Hypothyroidism and Hyperthyroidism in Pregnancy: Mafauzy MohamedDocument25 pagesHypothyroidism and Hyperthyroidism in Pregnancy: Mafauzy MohamedFatima ZahraNo ratings yet
- Thyroid and Pregnancy: A Few Interesting Clinical ConsiderationsDocument20 pagesThyroid and Pregnancy: A Few Interesting Clinical ConsiderationsjebabalanNo ratings yet
- Hypothyroidism in AdultsDocument55 pagesHypothyroidism in AdultsfjnaressiNo ratings yet
- QR Management of Thyroid Disorders (MEMS) 20200721Document16 pagesQR Management of Thyroid Disorders (MEMS) 20200721DNo ratings yet
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDocument22 pagesGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaNo ratings yet
- GP ThyroidDocument91 pagesGP ThyroidGawri AbeyNo ratings yet
- Tiroid Disease 14 HalamanDocument14 pagesTiroid Disease 14 HalamanDevi SuryandariNo ratings yet
- Diagnosis of HypothyroidismDocument10 pagesDiagnosis of HypothyroidismHanzla IrfanNo ratings yet
- Thyroid Disease in PregnancyDocument24 pagesThyroid Disease in PregnancyKai XinNo ratings yet
- Enf Tiroidea - UptodateDocument14 pagesEnf Tiroidea - Uptodatehenry mauricio polania castilloNo ratings yet
- Hypothyroidism and Myxedema ComaDocument53 pagesHypothyroidism and Myxedema ComaKuba ArebaNo ratings yet
- Hipotiroidismo SubclinicoDocument7 pagesHipotiroidismo SubclinicoJoseAbdalaNo ratings yet
- Thyroid Disease in PregnancyDocument12 pagesThyroid Disease in PregnancyOldriana Prawiro HapsariNo ratings yet
- Dr. Kruvilla - Hyperthyroidism in PregnancyDocument38 pagesDr. Kruvilla - Hyperthyroidism in PregnancyjarvantaraNo ratings yet
- Interpretasi TiroidDocument6 pagesInterpretasi TiroidSagita MuliaNo ratings yet
- Hypothyroidism PDFDocument5 pagesHypothyroidism PDFlegend789No ratings yet
- Jurnal InggrisDocument8 pagesJurnal InggrisNrfsavitriNo ratings yet
- Thyroid Disorders in Pregnancy FinalDocument60 pagesThyroid Disorders in Pregnancy Finalmonica caballes100% (1)
- Clinical Study: Thyroid Dysfunction and Autoantibodies Association With Hypertensive Disorders During PregnancyDocument6 pagesClinical Study: Thyroid Dysfunction and Autoantibodies Association With Hypertensive Disorders During PregnancyihdinzNo ratings yet
- Topic Presentation On Thyroid Disorders in PregnancyDocument31 pagesTopic Presentation On Thyroid Disorders in PregnancySairindri SahooNo ratings yet
- How To Interpret Thyroid Function TestDocument5 pagesHow To Interpret Thyroid Function TestSiveshKathirKamarajahNo ratings yet
- Guidelines For Management of Congenital Hypothyroidism1Document8 pagesGuidelines For Management of Congenital Hypothyroidism1Firdaus AzinunNo ratings yet
- Thyroid Function in Pre EcclampsiaDocument3 pagesThyroid Function in Pre EcclampsiaIOSRjournalNo ratings yet
- BTF Pregnancy and Thyroid Guidance For PatientsDocument2 pagesBTF Pregnancy and Thyroid Guidance For PatientsSulabh ShresthaNo ratings yet
- FNCP On Elevated Blood Pressure 2Document4 pagesFNCP On Elevated Blood Pressure 2Aaron EspirituNo ratings yet
- Thyroid Talk-FMD RdsDocument58 pagesThyroid Talk-FMD RdsSriman YarrarapuNo ratings yet
- Thyroid DiseasesDocument65 pagesThyroid DiseasesSahirNo ratings yet
- Thyroid Disorders in PregnancyDocument3 pagesThyroid Disorders in PregnancyZoel Nikonian100% (1)
- Eltroxin TabletsDocument16 pagesEltroxin TabletsSarthak DixitNo ratings yet
- Hypothyroidism SlidesDocument63 pagesHypothyroidism SlideswaterprincessNo ratings yet
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Document63 pagesClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaNo ratings yet
- Investigating Low TSH (BMJ 2013) Endocrine DisordersDocument4 pagesInvestigating Low TSH (BMJ 2013) Endocrine DisordersLouiseNo ratings yet
- Congenital HypothyroidismDocument43 pagesCongenital HypothyroidismJolmajas JoharNo ratings yet
- HipothyroidDocument48 pagesHipothyroidCakraEkkyNo ratings yet
- Thyroid Disorders: A Practical ApproachDocument26 pagesThyroid Disorders: A Practical ApproachSadashivayya SoppimathNo ratings yet
- Thyroid Disease in PregnancyDocument67 pagesThyroid Disease in PregnancySiti Fatimah100% (2)
- Lecture 29 30 Thyroid TherapeuticsDocument3 pagesLecture 29 30 Thyroid TherapeuticsAhmed MashalyNo ratings yet
- Thyroid Disease in PregnancyDocument17 pagesThyroid Disease in Pregnancydaniel100% (1)
- Endo Case No. 3Document2 pagesEndo Case No. 3Deinielle Magdangal RomeroNo ratings yet
- HypothyroidismDocument59 pagesHypothyroidismAmir Mahmoud100% (1)
- Practic Bulletin Tiroides - ACOG - OG - 2015Document10 pagesPractic Bulletin Tiroides - ACOG - OG - 2015Rich GmzNo ratings yet
- Hipertiroid Dan HiperemesisDocument50 pagesHipertiroid Dan HiperemesisAgungMaulanaYusufNo ratings yet
- Thyroid Disease in PregnancyDocument70 pagesThyroid Disease in PregnancyRajeev Sood100% (1)
- Withania Somnifera in Persons With BipolarDocument6 pagesWithania Somnifera in Persons With BipolarnikuNo ratings yet
- Acog Practice Bulletin TiroidesDocument10 pagesAcog Practice Bulletin TiroidesMerpi Alvarez Goris100% (1)
- Module I 2 - Thyroid Gland DisordersDocument43 pagesModule I 2 - Thyroid Gland Disordersaysha jasim100% (1)
- Stop The Thyroid Madness Sanjay Dixit MDDocument68 pagesStop The Thyroid Madness Sanjay Dixit MDdb50% (2)
- Kate PlanchetDocument29 pagesKate Planchetsundance127No ratings yet
- 10 16 Thyroid Function NitinDocument7 pages10 16 Thyroid Function NitinStrawberry ShortcakeNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- Section 2: Insulin Therapy in Type 1 and Type 2 DiabetesDocument48 pagesSection 2: Insulin Therapy in Type 1 and Type 2 Diabetesmohammed makkiNo ratings yet
- Counting Carbohydrates and Dosing Insulin For School Nurses: Presented byDocument26 pagesCounting Carbohydrates and Dosing Insulin For School Nurses: Presented bymohammed makkiNo ratings yet
- Nesidioblastosis and Insulinoma: A Rare Coexistence and A Therapeutic ChallengeDocument6 pagesNesidioblastosis and Insulinoma: A Rare Coexistence and A Therapeutic Challengemohammed makkiNo ratings yet
- 18 - Fatema AlSaliti - Thyroid - Graves' DiseaseDocument1 page18 - Fatema AlSaliti - Thyroid - Graves' Diseasemohammed makkiNo ratings yet
- Pathogenesis and Treatment of Renal Osteodystrophy: Eduardo Slatopolsky Esther Gonzalez Kevin MartinDocument9 pagesPathogenesis and Treatment of Renal Osteodystrophy: Eduardo Slatopolsky Esther Gonzalez Kevin Martinmohammed makkiNo ratings yet
- AACE TRC Interpretation of TFTs Part 3-FINALDocument31 pagesAACE TRC Interpretation of TFTs Part 3-FINALmohammed makkiNo ratings yet
- 19 - Abdul Aziz - Thyroid - Metastatic Differentiated Thyroid Carcinoma (Poster)Document1 page19 - Abdul Aziz - Thyroid - Metastatic Differentiated Thyroid Carcinoma (Poster)mohammed makkiNo ratings yet
- GD in PregnancyDocument37 pagesGD in Pregnancymohammed makkiNo ratings yet
- 46 - Abdullah Al Sabahi - Thyroid Disease - Subacute Thyroiditis PosterDocument1 page46 - Abdullah Al Sabahi - Thyroid Disease - Subacute Thyroiditis Postermohammed makkiNo ratings yet
- 14 - Nadjib Kaouache - Thyroid - CARDIOMETABOLIC RISK FACTORS IN A COHORT OFDocument1 page14 - Nadjib Kaouache - Thyroid - CARDIOMETABOLIC RISK FACTORS IN A COHORT OFmohammed makkiNo ratings yet
- 59 - Lynda Belabas - Thyroid Disease - Gaed Poster Family PDFDocument1 page59 - Lynda Belabas - Thyroid Disease - Gaed Poster Family PDFmohammed makkiNo ratings yet
- Exercise 4 - RRLDocument12 pagesExercise 4 - RRLNOREEN MITZI LOPEZNo ratings yet
- Pembagian Kelas Pelatihan KTIIDocument2 pagesPembagian Kelas Pelatihan KTIIKiki TeguhNo ratings yet
- Nelly Ombao NCM 112 Lecture Fluid ElectrolytesDocument16 pagesNelly Ombao NCM 112 Lecture Fluid ElectrolytesBasa, Rica Mae P.No ratings yet
- 2023 ISuman Bista ... Immediate Effect of Nada Yoga Meditation On Energy Levels and Alignment of Seven ChakrasDocument7 pages2023 ISuman Bista ... Immediate Effect of Nada Yoga Meditation On Energy Levels and Alignment of Seven ChakrasBoris PakholNo ratings yet
- RP 11 - Measuring Concentration of Glucose Using A Calibration CurveDocument4 pagesRP 11 - Measuring Concentration of Glucose Using A Calibration CurveAlfred SangNo ratings yet
- Specimen Collection Manual For Laboratory Serivces LRHDocument100 pagesSpecimen Collection Manual For Laboratory Serivces LRHPasan MaheshaNo ratings yet
- 0610 BIOLOGY: MARK SCHEME For The October/November 2010 Question Paper For The Guidance of TeachersDocument12 pages0610 BIOLOGY: MARK SCHEME For The October/November 2010 Question Paper For The Guidance of TeachersPreethi Sritharan100% (1)
- Vo2 Max Lab Report DoneDocument6 pagesVo2 Max Lab Report Doneapi-547193352No ratings yet
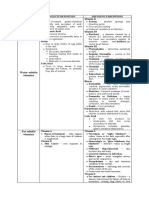
- Water Soluble Vitamins: Vitamins Toxicity/Definition Deficiency/Definition Niacin Vitamin ADocument3 pagesWater Soluble Vitamins: Vitamins Toxicity/Definition Deficiency/Definition Niacin Vitamin ARoshin TejeroNo ratings yet
- Ft4 Ii: Free ThyroxineDocument4 pagesFt4 Ii: Free ThyroxinehairiNo ratings yet
- AP Psych 2.3 Notes - Nervous and Endocrine SystemDocument2 pagesAP Psych 2.3 Notes - Nervous and Endocrine SystemIan BurtNo ratings yet
- Antocinaninas Reduzem Risco de DM2 Am J Clin Nutr-2012Document9 pagesAntocinaninas Reduzem Risco de DM2 Am J Clin Nutr-2012Elenice Peltz NutricionistaNo ratings yet
- Alisik 20207Document17 pagesAlisik 20207rocio fernandez san juanNo ratings yet
- Characterizattion Da Kappa Bioativos 2022Document6 pagesCharacterizattion Da Kappa Bioativos 2022Carlo CarloNo ratings yet
- Choque SepticoDocument44 pagesChoque SepticoManuel Antonio Lòpez UrbinaNo ratings yet
- Normal Lab Values UsmleDocument3 pagesNormal Lab Values UsmleAnne Maria50% (2)
- Chapter 25: Lipid Metabolism: Multiple ChoiceDocument7 pagesChapter 25: Lipid Metabolism: Multiple ChoiceMaxinefgc Baculo100% (1)
- Raymond - Peat - From Pms To MenopauseDocument196 pagesRaymond - Peat - From Pms To MenopauseM. J.No ratings yet
- Organ System OverviewDocument3 pagesOrgan System OverviewVan DajayNo ratings yet
- False Positives and False Negatives in Benzene Biolog - 2023 - Environmental ResDocument60 pagesFalse Positives and False Negatives in Benzene Biolog - 2023 - Environmental ResDana MateiNo ratings yet
- 3.4 Process of Absorption and Transportation of Digested Food and DefecationDocument9 pages3.4 Process of Absorption and Transportation of Digested Food and DefecationFrank ZachNo ratings yet
- 3 Ke 6 T 76 PIu 1 V J1 QQB WFGSWK OGdohkiuoiDocument4 pages3 Ke 6 T 76 PIu 1 V J1 QQB WFGSWK OGdohkiuoirizwan.arya085No ratings yet
- DrugDocument13 pagesDrugkhesler BacallaNo ratings yet
- Kolfe Keranyo Sub City Educational Office Grade 8 Biology Final Examination 2010Document5 pagesKolfe Keranyo Sub City Educational Office Grade 8 Biology Final Examination 2010Emma Mohamed KhalidNo ratings yet
- Fluid Balance Emma BoxallDocument13 pagesFluid Balance Emma BoxallRendra Syani Ulya FitriNo ratings yet
- Hypogonadotropic Hypogonadism and Gynaecomastia in The Young Adult: A Case SeriesDocument4 pagesHypogonadotropic Hypogonadism and Gynaecomastia in The Young Adult: A Case Seriesricepaddy1867No ratings yet
- MENSTRUAL CYCLEI-Investigatory-project-of-biologyDocument22 pagesMENSTRUAL CYCLEI-Investigatory-project-of-biologyAkshayNo ratings yet
- Accelerated Orthodontic Tooth MovementDocument34 pagesAccelerated Orthodontic Tooth MovementMehak Arya100% (1)



































































































Download as pptx, pdf, or txt
You might also like
- Test Bank For Goulds Pathophysiology For The Health Professions 7th Edition by Van Meter 9780323792882 Test BankDocument9 pagesTest Bank For Goulds Pathophysiology For The Health Professions 7th Edition by Van Meter 9780323792882 Test Bankmohamed arbi taifNo ratings yet
- Antidepressant & Psychedelic Drug Interaction ChartDocument3 pagesAntidepressant & Psychedelic Drug Interaction ChartFred The Nomad100% (2)
- Thyroid Disease in PregnancyDocument53 pagesThyroid Disease in PregnancyTee Wei SianNo ratings yet
- Hypothyroidism and Pregnancy Vol.2Document9 pagesHypothyroidism and Pregnancy Vol.2RakhiNo ratings yet
- Abnormal Thyroid Function in PregnancyDocument54 pagesAbnormal Thyroid Function in Pregnancyasri khazaliNo ratings yet
- Thyroid CasesDocument61 pagesThyroid CasesHamoud AlshehriNo ratings yet
- Tiroid Pada KehamilanDocument56 pagesTiroid Pada Kehamilanpeni_dwi100% (1)
- Hypothyroidism in AdultsDocument95 pagesHypothyroidism in AdultsJULIO FLORESNo ratings yet
- Hypothyroidism in PregnancyDocument14 pagesHypothyroidism in PregnancyShajia ZafarNo ratings yet
- Endocrine Pathology Associated With Pregnancy Dr. Yunus TanggoDocument60 pagesEndocrine Pathology Associated With Pregnancy Dr. Yunus TanggoReni AstutiNo ratings yet
- Preconception Counseling For Thyroid DisordersDocument7 pagesPreconception Counseling For Thyroid DisordersLiya AnjelinaNo ratings yet
- Good Clinical Practice Advice: Thyroid and PregnancyDocument5 pagesGood Clinical Practice Advice: Thyroid and Pregnancyjuan carlos pradaNo ratings yet
- Hypothyroidism and Hyperthyroidism in Pregnancy: Mafauzy MohamedDocument25 pagesHypothyroidism and Hyperthyroidism in Pregnancy: Mafauzy MohamedFatima ZahraNo ratings yet
- Thyroid and Pregnancy: A Few Interesting Clinical ConsiderationsDocument20 pagesThyroid and Pregnancy: A Few Interesting Clinical ConsiderationsjebabalanNo ratings yet
- Hypothyroidism in AdultsDocument55 pagesHypothyroidism in AdultsfjnaressiNo ratings yet
- QR Management of Thyroid Disorders (MEMS) 20200721Document16 pagesQR Management of Thyroid Disorders (MEMS) 20200721DNo ratings yet
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDocument22 pagesGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaNo ratings yet
- GP ThyroidDocument91 pagesGP ThyroidGawri AbeyNo ratings yet
- Tiroid Disease 14 HalamanDocument14 pagesTiroid Disease 14 HalamanDevi SuryandariNo ratings yet
- Diagnosis of HypothyroidismDocument10 pagesDiagnosis of HypothyroidismHanzla IrfanNo ratings yet
- Thyroid Disease in PregnancyDocument24 pagesThyroid Disease in PregnancyKai XinNo ratings yet
- Enf Tiroidea - UptodateDocument14 pagesEnf Tiroidea - Uptodatehenry mauricio polania castilloNo ratings yet
- Hypothyroidism and Myxedema ComaDocument53 pagesHypothyroidism and Myxedema ComaKuba ArebaNo ratings yet
- Hipotiroidismo SubclinicoDocument7 pagesHipotiroidismo SubclinicoJoseAbdalaNo ratings yet
- Thyroid Disease in PregnancyDocument12 pagesThyroid Disease in PregnancyOldriana Prawiro HapsariNo ratings yet
- Dr. Kruvilla - Hyperthyroidism in PregnancyDocument38 pagesDr. Kruvilla - Hyperthyroidism in PregnancyjarvantaraNo ratings yet
- Interpretasi TiroidDocument6 pagesInterpretasi TiroidSagita MuliaNo ratings yet
- Hypothyroidism PDFDocument5 pagesHypothyroidism PDFlegend789No ratings yet
- Jurnal InggrisDocument8 pagesJurnal InggrisNrfsavitriNo ratings yet
- Thyroid Disorders in Pregnancy FinalDocument60 pagesThyroid Disorders in Pregnancy Finalmonica caballes100% (1)
- Clinical Study: Thyroid Dysfunction and Autoantibodies Association With Hypertensive Disorders During PregnancyDocument6 pagesClinical Study: Thyroid Dysfunction and Autoantibodies Association With Hypertensive Disorders During PregnancyihdinzNo ratings yet
- Topic Presentation On Thyroid Disorders in PregnancyDocument31 pagesTopic Presentation On Thyroid Disorders in PregnancySairindri SahooNo ratings yet
- How To Interpret Thyroid Function TestDocument5 pagesHow To Interpret Thyroid Function TestSiveshKathirKamarajahNo ratings yet
- Guidelines For Management of Congenital Hypothyroidism1Document8 pagesGuidelines For Management of Congenital Hypothyroidism1Firdaus AzinunNo ratings yet
- Thyroid Function in Pre EcclampsiaDocument3 pagesThyroid Function in Pre EcclampsiaIOSRjournalNo ratings yet
- BTF Pregnancy and Thyroid Guidance For PatientsDocument2 pagesBTF Pregnancy and Thyroid Guidance For PatientsSulabh ShresthaNo ratings yet
- FNCP On Elevated Blood Pressure 2Document4 pagesFNCP On Elevated Blood Pressure 2Aaron EspirituNo ratings yet
- Thyroid Talk-FMD RdsDocument58 pagesThyroid Talk-FMD RdsSriman YarrarapuNo ratings yet
- Thyroid DiseasesDocument65 pagesThyroid DiseasesSahirNo ratings yet
- Thyroid Disorders in PregnancyDocument3 pagesThyroid Disorders in PregnancyZoel Nikonian100% (1)
- Eltroxin TabletsDocument16 pagesEltroxin TabletsSarthak DixitNo ratings yet
- Hypothyroidism SlidesDocument63 pagesHypothyroidism SlideswaterprincessNo ratings yet
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Document63 pagesClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaNo ratings yet
- Investigating Low TSH (BMJ 2013) Endocrine DisordersDocument4 pagesInvestigating Low TSH (BMJ 2013) Endocrine DisordersLouiseNo ratings yet
- Congenital HypothyroidismDocument43 pagesCongenital HypothyroidismJolmajas JoharNo ratings yet
- HipothyroidDocument48 pagesHipothyroidCakraEkkyNo ratings yet
- Thyroid Disorders: A Practical ApproachDocument26 pagesThyroid Disorders: A Practical ApproachSadashivayya SoppimathNo ratings yet
- Thyroid Disease in PregnancyDocument67 pagesThyroid Disease in PregnancySiti Fatimah100% (2)
- Lecture 29 30 Thyroid TherapeuticsDocument3 pagesLecture 29 30 Thyroid TherapeuticsAhmed MashalyNo ratings yet
- Thyroid Disease in PregnancyDocument17 pagesThyroid Disease in Pregnancydaniel100% (1)
- Endo Case No. 3Document2 pagesEndo Case No. 3Deinielle Magdangal RomeroNo ratings yet
- HypothyroidismDocument59 pagesHypothyroidismAmir Mahmoud100% (1)
- Practic Bulletin Tiroides - ACOG - OG - 2015Document10 pagesPractic Bulletin Tiroides - ACOG - OG - 2015Rich GmzNo ratings yet
- Hipertiroid Dan HiperemesisDocument50 pagesHipertiroid Dan HiperemesisAgungMaulanaYusufNo ratings yet
- Thyroid Disease in PregnancyDocument70 pagesThyroid Disease in PregnancyRajeev Sood100% (1)
- Withania Somnifera in Persons With BipolarDocument6 pagesWithania Somnifera in Persons With BipolarnikuNo ratings yet
- Acog Practice Bulletin TiroidesDocument10 pagesAcog Practice Bulletin TiroidesMerpi Alvarez Goris100% (1)
- Module I 2 - Thyroid Gland DisordersDocument43 pagesModule I 2 - Thyroid Gland Disordersaysha jasim100% (1)
- Stop The Thyroid Madness Sanjay Dixit MDDocument68 pagesStop The Thyroid Madness Sanjay Dixit MDdb50% (2)
- Kate PlanchetDocument29 pagesKate Planchetsundance127No ratings yet
- 10 16 Thyroid Function NitinDocument7 pages10 16 Thyroid Function NitinStrawberry ShortcakeNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- Section 2: Insulin Therapy in Type 1 and Type 2 DiabetesDocument48 pagesSection 2: Insulin Therapy in Type 1 and Type 2 Diabetesmohammed makkiNo ratings yet
- Counting Carbohydrates and Dosing Insulin For School Nurses: Presented byDocument26 pagesCounting Carbohydrates and Dosing Insulin For School Nurses: Presented bymohammed makkiNo ratings yet
- Nesidioblastosis and Insulinoma: A Rare Coexistence and A Therapeutic ChallengeDocument6 pagesNesidioblastosis and Insulinoma: A Rare Coexistence and A Therapeutic Challengemohammed makkiNo ratings yet
- 18 - Fatema AlSaliti - Thyroid - Graves' DiseaseDocument1 page18 - Fatema AlSaliti - Thyroid - Graves' Diseasemohammed makkiNo ratings yet
- Pathogenesis and Treatment of Renal Osteodystrophy: Eduardo Slatopolsky Esther Gonzalez Kevin MartinDocument9 pagesPathogenesis and Treatment of Renal Osteodystrophy: Eduardo Slatopolsky Esther Gonzalez Kevin Martinmohammed makkiNo ratings yet
- AACE TRC Interpretation of TFTs Part 3-FINALDocument31 pagesAACE TRC Interpretation of TFTs Part 3-FINALmohammed makkiNo ratings yet
- 19 - Abdul Aziz - Thyroid - Metastatic Differentiated Thyroid Carcinoma (Poster)Document1 page19 - Abdul Aziz - Thyroid - Metastatic Differentiated Thyroid Carcinoma (Poster)mohammed makkiNo ratings yet
- GD in PregnancyDocument37 pagesGD in Pregnancymohammed makkiNo ratings yet
- 46 - Abdullah Al Sabahi - Thyroid Disease - Subacute Thyroiditis PosterDocument1 page46 - Abdullah Al Sabahi - Thyroid Disease - Subacute Thyroiditis Postermohammed makkiNo ratings yet
- 14 - Nadjib Kaouache - Thyroid - CARDIOMETABOLIC RISK FACTORS IN A COHORT OFDocument1 page14 - Nadjib Kaouache - Thyroid - CARDIOMETABOLIC RISK FACTORS IN A COHORT OFmohammed makkiNo ratings yet
- 59 - Lynda Belabas - Thyroid Disease - Gaed Poster Family PDFDocument1 page59 - Lynda Belabas - Thyroid Disease - Gaed Poster Family PDFmohammed makkiNo ratings yet
- Exercise 4 - RRLDocument12 pagesExercise 4 - RRLNOREEN MITZI LOPEZNo ratings yet
- Pembagian Kelas Pelatihan KTIIDocument2 pagesPembagian Kelas Pelatihan KTIIKiki TeguhNo ratings yet
- Nelly Ombao NCM 112 Lecture Fluid ElectrolytesDocument16 pagesNelly Ombao NCM 112 Lecture Fluid ElectrolytesBasa, Rica Mae P.No ratings yet
- 2023 ISuman Bista ... Immediate Effect of Nada Yoga Meditation On Energy Levels and Alignment of Seven ChakrasDocument7 pages2023 ISuman Bista ... Immediate Effect of Nada Yoga Meditation On Energy Levels and Alignment of Seven ChakrasBoris PakholNo ratings yet
- RP 11 - Measuring Concentration of Glucose Using A Calibration CurveDocument4 pagesRP 11 - Measuring Concentration of Glucose Using A Calibration CurveAlfred SangNo ratings yet
- Specimen Collection Manual For Laboratory Serivces LRHDocument100 pagesSpecimen Collection Manual For Laboratory Serivces LRHPasan MaheshaNo ratings yet
- 0610 BIOLOGY: MARK SCHEME For The October/November 2010 Question Paper For The Guidance of TeachersDocument12 pages0610 BIOLOGY: MARK SCHEME For The October/November 2010 Question Paper For The Guidance of TeachersPreethi Sritharan100% (1)
- Vo2 Max Lab Report DoneDocument6 pagesVo2 Max Lab Report Doneapi-547193352No ratings yet
- Water Soluble Vitamins: Vitamins Toxicity/Definition Deficiency/Definition Niacin Vitamin ADocument3 pagesWater Soluble Vitamins: Vitamins Toxicity/Definition Deficiency/Definition Niacin Vitamin ARoshin TejeroNo ratings yet
- Ft4 Ii: Free ThyroxineDocument4 pagesFt4 Ii: Free ThyroxinehairiNo ratings yet
- AP Psych 2.3 Notes - Nervous and Endocrine SystemDocument2 pagesAP Psych 2.3 Notes - Nervous and Endocrine SystemIan BurtNo ratings yet
- Antocinaninas Reduzem Risco de DM2 Am J Clin Nutr-2012Document9 pagesAntocinaninas Reduzem Risco de DM2 Am J Clin Nutr-2012Elenice Peltz NutricionistaNo ratings yet
- Alisik 20207Document17 pagesAlisik 20207rocio fernandez san juanNo ratings yet
- Characterizattion Da Kappa Bioativos 2022Document6 pagesCharacterizattion Da Kappa Bioativos 2022Carlo CarloNo ratings yet
- Choque SepticoDocument44 pagesChoque SepticoManuel Antonio Lòpez UrbinaNo ratings yet
- Normal Lab Values UsmleDocument3 pagesNormal Lab Values UsmleAnne Maria50% (2)
- Chapter 25: Lipid Metabolism: Multiple ChoiceDocument7 pagesChapter 25: Lipid Metabolism: Multiple ChoiceMaxinefgc Baculo100% (1)
- Raymond - Peat - From Pms To MenopauseDocument196 pagesRaymond - Peat - From Pms To MenopauseM. J.No ratings yet
- Organ System OverviewDocument3 pagesOrgan System OverviewVan DajayNo ratings yet
- False Positives and False Negatives in Benzene Biolog - 2023 - Environmental ResDocument60 pagesFalse Positives and False Negatives in Benzene Biolog - 2023 - Environmental ResDana MateiNo ratings yet
- 3.4 Process of Absorption and Transportation of Digested Food and DefecationDocument9 pages3.4 Process of Absorption and Transportation of Digested Food and DefecationFrank ZachNo ratings yet
- 3 Ke 6 T 76 PIu 1 V J1 QQB WFGSWK OGdohkiuoiDocument4 pages3 Ke 6 T 76 PIu 1 V J1 QQB WFGSWK OGdohkiuoirizwan.arya085No ratings yet
- DrugDocument13 pagesDrugkhesler BacallaNo ratings yet
- Kolfe Keranyo Sub City Educational Office Grade 8 Biology Final Examination 2010Document5 pagesKolfe Keranyo Sub City Educational Office Grade 8 Biology Final Examination 2010Emma Mohamed KhalidNo ratings yet
- Fluid Balance Emma BoxallDocument13 pagesFluid Balance Emma BoxallRendra Syani Ulya FitriNo ratings yet
- Hypogonadotropic Hypogonadism and Gynaecomastia in The Young Adult: A Case SeriesDocument4 pagesHypogonadotropic Hypogonadism and Gynaecomastia in The Young Adult: A Case Seriesricepaddy1867No ratings yet
- MENSTRUAL CYCLEI-Investigatory-project-of-biologyDocument22 pagesMENSTRUAL CYCLEI-Investigatory-project-of-biologyAkshayNo ratings yet
- Accelerated Orthodontic Tooth MovementDocument34 pagesAccelerated Orthodontic Tooth MovementMehak Arya100% (1)