Download as ppt, pdf, or txt
You might also like
- Sexual Development & Differentiation: Sex and GenderDocument10 pagesSexual Development & Differentiation: Sex and GenderDeboprasad DasNo ratings yet
- SexualDocument73 pagesSexualKate Angelique RodriguezNo ratings yet
- Developmental Biology XL 138: Week 10Document61 pagesDevelopmental Biology XL 138: Week 10Soji AdimulaNo ratings yet
- Sex & Love SlidesDocument45 pagesSex & Love SlidesJennifer Isom Schmidtke, Ph.D.No ratings yet
- 1.5.2.3 - Diferensiasi SexDocument37 pages1.5.2.3 - Diferensiasi SexHiya KontetNo ratings yet
- Reproductive - L1 & L2Document22 pagesReproductive - L1 & L2Abdikadir XaadNo ratings yet
- Saiby Khan, GynaeDocument29 pagesSaiby Khan, Gynaeinstagramfollowers168No ratings yet
- Gender As Constructed - 1 (Class)Document23 pagesGender As Constructed - 1 (Class)harshitaNo ratings yet
- 05 AnishaDocument12 pages05 AnishaOGNo ratings yet
- L1 General Intro To Reprod PhysiolDocument20 pagesL1 General Intro To Reprod PhysiolMoses AjiwekaNo ratings yet
- Human GeneticsDocument21 pagesHuman GeneticsReaNo ratings yet
- Embryology GenitalDocument53 pagesEmbryology GenitalDhonat Flash100% (1)
- Sexual Self: Sex As A Commodity: Sex Is SometimesDocument10 pagesSexual Self: Sex As A Commodity: Sex Is SometimesasiannadeviliaNo ratings yet
- Sex Determination and InheritanceDocument61 pagesSex Determination and Inheritancedaniel dennis encarta100% (1)
- Gender and SexualityDocument42 pagesGender and Sexualityamanoc02No ratings yet
- Sexuality and Gender: PsychologyDocument42 pagesSexuality and Gender: PsychologymuhibNo ratings yet
- SexDocument27 pagesSexRendy Hermawan100% (1)
- The Sexual SelfDocument33 pagesThe Sexual SelfEdrian Genesis SebleroNo ratings yet
- Reproductive & Sexual Health: Pp. 83-116 PiliteriDocument9 pagesReproductive & Sexual Health: Pp. 83-116 PiliteriGwyneth ManioNo ratings yet
- Psychosomatics: Digestive System: Miguel Agustin ST Francisco, RPM, Mpsy CandDocument45 pagesPsychosomatics: Digestive System: Miguel Agustin ST Francisco, RPM, Mpsy CandRalph Christian ZorillaNo ratings yet
- Reproductive PharmaDocument106 pagesReproductive PharmaDessalegn LemmaNo ratings yet
- What Comes Under The DSD Umbrella?Document50 pagesWhat Comes Under The DSD Umbrella?Scott LoveNo ratings yet
- GeneticsDocument4 pagesGeneticsAngelica AycardoNo ratings yet
- p09 Hormones SexDocument37 pagesp09 Hormones SexBob SmithNo ratings yet
- Feldman CD7 Chapter 3 PPT - FDocument59 pagesFeldman CD7 Chapter 3 PPT - FErin TrumanNo ratings yet
- GenSoc Reviewer PrelimsDocument7 pagesGenSoc Reviewer Prelimsmangalinoangeline10No ratings yet
- The Transgender ProblemDocument15 pagesThe Transgender ProblemRizwan Asad KhanNo ratings yet
- Gender and SocietyDocument36 pagesGender and SocietyBenedict A. MancillaNo ratings yet
- NSG 123 Module 2Document128 pagesNSG 123 Module 2rigasanaorayNo ratings yet
- Human Sexuality Self Society and Culture 1st Edition Herdt Solutions ManualDocument23 pagesHuman Sexuality Self Society and Culture 1st Edition Herdt Solutions Manualdianbandelethek6xo100% (21)
- Gender Midterm NotesDocument27 pagesGender Midterm Noteslandrade3440No ratings yet
- Biological Theories of GenderDocument17 pagesBiological Theories of GenderJoe Brayle JoeyNo ratings yet
- L 3. Heredity and Environment Influence PDFDocument13 pagesL 3. Heredity and Environment Influence PDFanon_478950284No ratings yet
- Maternal and Child Module 2Document4 pagesMaternal and Child Module 2AmethystNo ratings yet
- Gender and Human Sexuality (Dimensions of Sexuality)Document18 pagesGender and Human Sexuality (Dimensions of Sexuality)Dann PagaduanNo ratings yet
- Male Reproductive SystemDocument12 pagesMale Reproductive SystemIvy AguasNo ratings yet
- 37 UPDATED Genetic+Diseases Allen PDFDocument36 pages37 UPDATED Genetic+Diseases Allen PDFSuh DudeNo ratings yet
- RSDocument24 pagesRSVinothkumar VKNo ratings yet
- Amenorrhea: Stelian Hodorogea, Associate ProfessorDocument73 pagesAmenorrhea: Stelian Hodorogea, Associate ProfessorgvfhgNo ratings yet
- Chapter 1 - Lesson 1Document40 pagesChapter 1 - Lesson 1ATASHA CAROLINA BENEGIANNo ratings yet
- Palibhasa Lalaki, Eh Kasi Babae!Document17 pagesPalibhasa Lalaki, Eh Kasi Babae!Dafchen Nio MahasolNo ratings yet
- Sexlinkedgenes DemoDocument57 pagesSexlinkedgenes DemopearlNo ratings yet
- ReproduksiDocument74 pagesReproduksifarica yasminNo ratings yet
- 3 - Heredity and EnvironmentDocument59 pages3 - Heredity and EnvironmentI'rfah IsaNo ratings yet
- Sexual Growth and Development-Reproduction 2021Document79 pagesSexual Growth and Development-Reproduction 2021Elijah Kihiu18No ratings yet
- Psych FinalsDocument10 pagesPsych FinalsMARK WILLIE ABADNo ratings yet
- Module 1 Sex As The Biological Basis of GenderDocument12 pagesModule 1 Sex As The Biological Basis of GenderMA. CARLA CACHUELANo ratings yet
- Gender and Gender RolesDocument36 pagesGender and Gender Rolessgt_invictusNo ratings yet
- Barr Body and HermaphroditismDocument41 pagesBarr Body and HermaphroditismTamjid KhanNo ratings yet
- SexLinkage TraitsDocument56 pagesSexLinkage TraitsAnna Grace Lobigas RanocoNo ratings yet
- Approach To A Case of Ambiguous GenitaliaDocument37 pagesApproach To A Case of Ambiguous GenitaliaDR.MAULIK SHAHNo ratings yet
- MODULE 7 PART 1 SEXUAL SELF ViBe 2nd TERM 2022 PDFDocument38 pagesMODULE 7 PART 1 SEXUAL SELF ViBe 2nd TERM 2022 PDFGILBERT BANTANo ratings yet
- Repro A 2017Document94 pagesRepro A 2017Ruvarashe MutadzaNo ratings yet
- Measures of Man Exam 2 Study GuideDocument5 pagesMeasures of Man Exam 2 Study GuideKennon RudeNo ratings yet
- Sex Determination ReportDocument35 pagesSex Determination ReportCarmela LipoNo ratings yet
- Sex Determination and Inheritances Related To SexDocument23 pagesSex Determination and Inheritances Related To SexNati TesfaNo ratings yet
- Three Dimensions of Human SexualityDocument26 pagesThree Dimensions of Human SexualityMark Gabriel DomingoNo ratings yet
- Male Reproductive SystemDocument116 pagesMale Reproductive SystemFaiz Yunanto MangoendiprodjoNo ratings yet
- Sex Ed Uncensored - Sexual Identity: Mind Blowing Sex Sh8t!!! for Young AdultsFrom EverandSex Ed Uncensored - Sexual Identity: Mind Blowing Sex Sh8t!!! for Young AdultsNo ratings yet
- Infant Gender Selection & Personalized Medicine: Consumer's GuideFrom EverandInfant Gender Selection & Personalized Medicine: Consumer's GuideNo ratings yet
- Digital Clubbing in Pediatric Age GroupDocument33 pagesDigital Clubbing in Pediatric Age GroupDeboprasad DasNo ratings yet
- Roving Ring ScotomaDocument3 pagesRoving Ring ScotomaDeboprasad DasNo ratings yet
- Renal FailureDocument4 pagesRenal FailureDeboprasad DasNo ratings yet
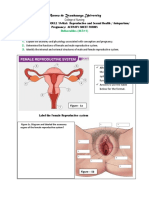
- Sexual Development & Differentiation: Sex and GenderDocument10 pagesSexual Development & Differentiation: Sex and GenderDeboprasad DasNo ratings yet
- Pediatric Nursing Review NleDocument56 pagesPediatric Nursing Review Nlemarygrace canoNo ratings yet
- WHO Recommendation On Techniques For Preventing Perineal Trauma During Labour - RHL PDFDocument19 pagesWHO Recommendation On Techniques For Preventing Perineal Trauma During Labour - RHL PDFsaksNo ratings yet
- Clinical Manifestation of Necrotizing EnterocolitiDocument6 pagesClinical Manifestation of Necrotizing EnterocolitiJyotirmayeeNo ratings yet
- Https Emedicine - MedscapeDocument14 pagesHttps Emedicine - MedscapeNanaNo ratings yet
- Twin PregnancyDocument66 pagesTwin PregnancyEkta Rajput100% (1)
- Ge 101Document65 pagesGe 101samorales92No ratings yet
- Prenatal Aneuploidy ScreeningDocument80 pagesPrenatal Aneuploidy ScreeningBharti Pant GahtoriNo ratings yet
- Vital StatisticsDocument33 pagesVital StatisticssrimalathiNo ratings yet
- Seminar Presentation: Presented By: D.Kaviya Final YearDocument36 pagesSeminar Presentation: Presented By: D.Kaviya Final YearhebzibaNo ratings yet
- Fetal BehaviourDocument1 pageFetal BehaviourJuan José Espinoza OsoresNo ratings yet
- UntitledDocument3 pagesUntitledSamriti NarangNo ratings yet
- Asynchronous Activity Sheet FormsDocument8 pagesAsynchronous Activity Sheet FormsNur SanaaniNo ratings yet
- Sexual and Reproductive Health OverviewDocument12 pagesSexual and Reproductive Health OverviewAssishNo ratings yet
- Question Bank Biology Class 12Document6 pagesQuestion Bank Biology Class 12Mᴀïᴢᴍɛɛŋ AŋꜱᴀʀïNo ratings yet
- Prenatal Diagnosis and Successful Surgical Treatment of Gastrochisis: Case ReportDocument4 pagesPrenatal Diagnosis and Successful Surgical Treatment of Gastrochisis: Case ReportIJAR JOURNALNo ratings yet
- Understanding The SelfDocument13 pagesUnderstanding The SelfJillian NoreenNo ratings yet
- KPIs Jan 21, 2019Document113 pagesKPIs Jan 21, 2019JamalNo ratings yet
- Pukall 3e - Test Bank - Chapter 01Document17 pagesPukall 3e - Test Bank - Chapter 01AlexNo ratings yet
- Claudio Case Study of Pregnancy Induced HypertensionDocument78 pagesClaudio Case Study of Pregnancy Induced HypertensionTanya Victoria Lean ClaudioNo ratings yet
- Causes, Severity and Outcome of Neonatal Thrombocytopenia in Hi-Tech Medical College and Hospital, BhubaneswarDocument4 pagesCauses, Severity and Outcome of Neonatal Thrombocytopenia in Hi-Tech Medical College and Hospital, BhubaneswarInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 12bio Assignment ch123Document14 pages12bio Assignment ch123Krishna GovilNo ratings yet
- Xanthogranulomatous Oophoritis Secondary To Talcum Powder Case Report and Review of The LiteratureDocument4 pagesXanthogranulomatous Oophoritis Secondary To Talcum Powder Case Report and Review of The LiteratureCamil ChouairyNo ratings yet
- Pelvic Examination: Liezel B. Cauilan MSN, MSTDocument25 pagesPelvic Examination: Liezel B. Cauilan MSN, MSTSIR ONENo ratings yet
- Gestational Trophoblastic Neoplasia: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Document45 pagesGestational Trophoblastic Neoplasia: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Roshni SethiaNo ratings yet
- MONTHLY BIRTH DISTRIBUTION OF THE WILD BOAR IN CENTRAL PORTUGAL Fonseca Et Al, 2001Document6 pagesMONTHLY BIRTH DISTRIBUTION OF THE WILD BOAR IN CENTRAL PORTUGAL Fonseca Et Al, 2001Débora SilvaNo ratings yet
- Best Blood Group Compatibility For MarriageDocument14 pagesBest Blood Group Compatibility For MarriageTewodros Kassa Ye EtalemahuNo ratings yet
- Artificial Insemination Family PDFDocument15 pagesArtificial Insemination Family PDFDelos NourseiNo ratings yet
- Predictors For Response To Letrozole As An Ovulation Induction in Anovulatory Infertile Polycystic Ovarian Syndrome WomenDocument23 pagesPredictors For Response To Letrozole As An Ovulation Induction in Anovulatory Infertile Polycystic Ovarian Syndrome WomenAndre OpaNo ratings yet
- Concise Clinical Embryology An Integrated Case Based Approach Mar 18 2021 - 0323696155 - Elsevier 1St Edition Torchia MSC PHD Full ChapterDocument68 pagesConcise Clinical Embryology An Integrated Case Based Approach Mar 18 2021 - 0323696155 - Elsevier 1St Edition Torchia MSC PHD Full Chapterraymond.flores626100% (9)
- Jurnal Menyikat Gigi PDFDocument8 pagesJurnal Menyikat Gigi PDFeka meiti elasariNo ratings yet