Download as ppt, pdf, or txt
You might also like
- Biology Syllabus Forms 3-4Document88 pagesBiology Syllabus Forms 3-4Malack Chagwa100% (7)
- 1-3 Way Bottle System and SuctioningDocument9 pages1-3 Way Bottle System and SuctioningJz Andamun100% (2)
- Physical Education (Prelim)Document20 pagesPhysical Education (Prelim)Adriel MarasiganNo ratings yet
- LarynxDocument5 pagesLarynxGeraldine Marie SalvoNo ratings yet
- PSL301 Midterm 2 ReviewDocument24 pagesPSL301 Midterm 2 Reviewtapi0ca100% (1)
- Chest Tubes and Drainage Systems: Deb Updegraff RN, CNS Picu LPCHDocument28 pagesChest Tubes and Drainage Systems: Deb Updegraff RN, CNS Picu LPCHLucila LugoNo ratings yet
- Chest TubesDocument28 pagesChest Tubeswarda farooqNo ratings yet
- ChesttubedrainageDocument65 pagesChesttubedrainagejerinthomasrajanNo ratings yet
- Tube ThoracostomyDocument17 pagesTube ThoracostomyheiyuNo ratings yet
- Chest DrainageDocument22 pagesChest DrainageAmeliaM100% (7)
- Assisting With Chest Tube InsertionDocument5 pagesAssisting With Chest Tube InsertionLoveSheryNo ratings yet
- Chest Tube and Water-Seal DrainageDocument25 pagesChest Tube and Water-Seal DrainageGhadaNo ratings yet
- Skills LabDocument3 pagesSkills Labmilcah_castilloNo ratings yet
- Chest Tube ThoracostomyDocument7 pagesChest Tube Thoracostomyfufoo_tracylirioNo ratings yet
- Chest Tube ThoracostomyDocument7 pagesChest Tube Thoracostomyskyblueali100% (2)
- Pleural TappingDocument15 pagesPleural TappingAnusha Verghese100% (1)
- Chest Tube Care Management TroubleshootingDocument5 pagesChest Tube Care Management TroubleshootingRaina Ginella DsouzaNo ratings yet
- Chest Tubes and ThoracentesisDocument18 pagesChest Tubes and ThoracentesisecleptosNo ratings yet
- Management of Chest TubeDocument22 pagesManagement of Chest TubeFatima Hafza SahiddinNo ratings yet
- Chest TubeDocument3 pagesChest TubeJohn Michael SalinasNo ratings yet
- ThoracostomyDocument2 pagesThoracostomyJanelle MarceraNo ratings yet
- What Is A Tracheostomy? Why Is A Tracheostomy Performed?Document5 pagesWhat Is A Tracheostomy? Why Is A Tracheostomy Performed?Mara JnelleNo ratings yet
- Laxmi MamDocument7 pagesLaxmi MamkamalshrishNo ratings yet
- Management of Chest TubeDocument22 pagesManagement of Chest Tubernrmmanphd100% (1)
- Chest Tubes OUPUTDocument3 pagesChest Tubes OUPUTparislove19No ratings yet
- Chest Tubes and ThoracentesisDocument18 pagesChest Tubes and ThoracentesisecleptosNo ratings yet
- Ateneo de Naga University: College of NursingDocument3 pagesAteneo de Naga University: College of NursingRenie SerranoNo ratings yet
- Minor Surgical Procedures...Document10 pagesMinor Surgical Procedures...Silinna May Lee SanicoNo ratings yet
- Water Sael DrainageDocument36 pagesWater Sael DrainageerlinaNo ratings yet
- LM 3 - Chest TubeDocument5 pagesLM 3 - Chest TubeMelrhean GraceNo ratings yet
- Pleural Anatomy 1st Year Clinical by DR MuzaffarDocument22 pagesPleural Anatomy 1st Year Clinical by DR MuzaffarKashar SaeedNo ratings yet
- NursingBulletin Notes On PneumothoraxDocument27 pagesNursingBulletin Notes On Pneumothoraxseigelystic100% (11)
- CTT BedasDocument37 pagesCTT BedasraecmyNo ratings yet
- CTTDocument47 pagesCTTleizelgalvezNo ratings yet
- Oxygenation 3.0Document14 pagesOxygenation 3.0Jake Yvan DizonNo ratings yet
- Respiratory System: Gemalyn BulawanDocument122 pagesRespiratory System: Gemalyn BulawanSofia Deneise AnasariasNo ratings yet
- Surgical Tubes: Hadi MunibDocument57 pagesSurgical Tubes: Hadi MunibAli ahmedNo ratings yet
- CTT CareDocument76 pagesCTT CareMarites Santos AquinoNo ratings yet
- Assisting in Thoracostomy Tube InsertionDocument54 pagesAssisting in Thoracostomy Tube Insertioncoosa liquorsNo ratings yet
- Prosedur WSD (Water Seal Drainage)Document44 pagesProsedur WSD (Water Seal Drainage)White GooseNo ratings yet
- Types of Chest Drainage SystemDocument3 pagesTypes of Chest Drainage SystembernardsoNo ratings yet
- Chest Tube Insertion: An Intercostal CatheterDocument2 pagesChest Tube Insertion: An Intercostal CatheterssNo ratings yet
- TRACHEOSTOMYDocument2 pagesTRACHEOSTOMY3C SAVELLA, Glaiza Marie RNo ratings yet
- Abdominal ParacentesisDocument4 pagesAbdominal ParacentesisRashmi C S100% (1)
- Chest TubeDocument8 pagesChest TubetanabalrajNo ratings yet
- Chest Tube DrainageDocument7 pagesChest Tube Drainagekim reyes100% (1)
- Chest Tubes and Water Seal Drainage: P. NandiDocument8 pagesChest Tubes and Water Seal Drainage: P. Nandikim_sayamNo ratings yet
- Chest TubeDocument18 pagesChest TubeAyu MasturaNo ratings yet
- IR Lctr 10 part 2Document33 pagesIR Lctr 10 part 2seemabfarwauaeNo ratings yet
- Chest Tube Insertion and MonitoringDocument4 pagesChest Tube Insertion and MonitoringCamille Cirineo Arensol100% (2)
- Chapter 27: Lower Respiratory Problems Pleural Effusion With Thoracentesis and Chest TubeDocument3 pagesChapter 27: Lower Respiratory Problems Pleural Effusion With Thoracentesis and Chest TubeSherree HayesNo ratings yet
- Chest Tube DrainageDocument45 pagesChest Tube DrainageDonald BidenNo ratings yet
- Tracheostomy: ENT Department DMC & Hospital Ludhiana PunjabDocument46 pagesTracheostomy: ENT Department DMC & Hospital Ludhiana PunjabVikrant MittalNo ratings yet
- MedSurg NotesDocument57 pagesMedSurg NotesCHRISTOFER CORONADONo ratings yet
- Purpose of Chest TubesDocument2 pagesPurpose of Chest TubesCathrine Mae RamilNo ratings yet
- WSDDocument59 pagesWSDdiandrasafirinaNo ratings yet
- Chest TubesDocument2 pagesChest TubesLeahandJosh NadhernyNo ratings yet
- Nursing Practices: Troubleshooting Thoracostomy Tube ManagementDocument6 pagesNursing Practices: Troubleshooting Thoracostomy Tube ManagementDeo RizkyandriNo ratings yet
- TracheostomyDocument4 pagesTracheostomyNapieh Bulalaque PolisticoNo ratings yet
- Oncology - Presentation EditedDocument71 pagesOncology - Presentation EditedSarah Racheal AkelloNo ratings yet
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Bloodborne April 08Document32 pagesBloodborne April 08Muhd ShafiqNo ratings yet
- Trip Log Templates MS Excel #02Document2 pagesTrip Log Templates MS Excel #02Muhd ShafiqNo ratings yet
- Installation GuideDocument1 pageInstallation GuideMuhd ShafiqNo ratings yet
- Sample Material Required QO RehabDocument2 pagesSample Material Required QO RehabMuhd ShafiqNo ratings yet
- Audit Report Writing Guid1Document2 pagesAudit Report Writing Guid1Muhd ShafiqNo ratings yet
- IC 2023 Calendar of Events 9053Document5 pagesIC 2023 Calendar of Events 9053Muhd ShafiqNo ratings yet
- Employee Training LogDocument3 pagesEmployee Training LogMuhd ShafiqNo ratings yet
- IC Transition Plan Template 8544 V1Document4 pagesIC Transition Plan Template 8544 V1Muhd ShafiqNo ratings yet
- Template Turtle DiagramDocument1 pageTemplate Turtle DiagramMuhd ShafiqNo ratings yet
- Robotic Scrubber Downtime RecordDocument1 pageRobotic Scrubber Downtime RecordMuhd ShafiqNo ratings yet
- Excel ChandranDocument2 pagesExcel ChandranMuhd ShafiqNo ratings yet
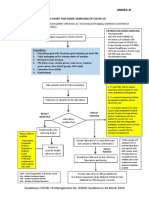
- Annex 2f COVID19Document1 pageAnnex 2f COVID19Muhd ShafiqNo ratings yet
- Borang Audit DalamanDocument5 pagesBorang Audit DalamanMuhd ShafiqNo ratings yet
- AP Corporate ProfileDocument28 pagesAP Corporate ProfileMuhd ShafiqNo ratings yet
- JD RiskDocument3 pagesJD RiskMuhd ShafiqNo ratings yet
- Iso Auto-Service 4R2SDocument2 pagesIso Auto-Service 4R2SMuhd ShafiqNo ratings yet
- 03 NCR FormDocument1 page03 NCR FormMuhd ShafiqNo ratings yet
- 02 Internal Audit ChecklistDocument2 pages02 Internal Audit ChecklistMuhd ShafiqNo ratings yet
- Appendix 3 Assurance Statement GMDocument1 pageAppendix 3 Assurance Statement GMMuhd ShafiqNo ratings yet
- File LABEL INTERNAL AUDITDocument1 pageFile LABEL INTERNAL AUDITMuhd ShafiqNo ratings yet
- ASTMA NisreenDocument19 pagesASTMA NisreenMuhd ShafiqNo ratings yet
- Quality Management Summary Report Test 1Document4 pagesQuality Management Summary Report Test 1Muhd ShafiqNo ratings yet
- Nazri HikingDocument11 pagesNazri HikingMuhd ShafiqNo ratings yet
- ATP2022Document60 pagesATP2022Muhd ShafiqNo ratings yet
- 7 Step Isolation Cleaning ProcessDocument5 pages7 Step Isolation Cleaning ProcessMuhd ShafiqNo ratings yet
- Low Carbon Society Blueprint For Iskandar Malaysia 2025 Summary For PolicymakersDocument44 pagesLow Carbon Society Blueprint For Iskandar Malaysia 2025 Summary For PolicymakersMuhd ShafiqNo ratings yet
- Gantt Chart: Learn About Gantt ChartsDocument4 pagesGantt Chart: Learn About Gantt ChartsMuhd ShafiqNo ratings yet
- Msds of TccaDocument5 pagesMsds of Tccadie_1No ratings yet
- LP - Grade-7 CH-10 Respiration in OrganismsDocument3 pagesLP - Grade-7 CH-10 Respiration in Organismsanju singhNo ratings yet
- Dwnload Full Cardiovascular and Pulmonary Physical Therapy Evidence To Practice 5th Edition Frownfelter Test Bank PDFDocument36 pagesDwnload Full Cardiovascular and Pulmonary Physical Therapy Evidence To Practice 5th Edition Frownfelter Test Bank PDFphysetergrannam.devtjz100% (20)
- Icu Head To Toe AssessmentDocument3 pagesIcu Head To Toe Assessmentmsbunnilee100% (2)
- Bear Cub 750 - Quick User GuideDocument2 pagesBear Cub 750 - Quick User GuideSn DayanidhiNo ratings yet
- Pathophysiology-LCHFDocument2 pagesPathophysiology-LCHFNicole Villanueva, BSN - Level 3ANo ratings yet
- Resusitasi Neonatus 2020 AAPDocument30 pagesResusitasi Neonatus 2020 AAPWafiq AzizahNo ratings yet
- Trans Pulmopatho ColoredDocument8 pagesTrans Pulmopatho Colored2012No ratings yet
- BreathingDocument46 pagesBreathingRamnaresh SharmaNo ratings yet
- Assessing Thorax LungsDocument20 pagesAssessing Thorax Lungskyla boncacasNo ratings yet
- Parte 2 Complete Reflexology For Live (Inglés) Autor Barbara y Kevin Kunz-262-289Document28 pagesParte 2 Complete Reflexology For Live (Inglés) Autor Barbara y Kevin Kunz-262-289Hombres Alto ValorNo ratings yet
- PULMODocument3 pagesPULMOGianna Louisse Marie Dacalos DiazNo ratings yet
- Jurnal Efusi PleuraDocument12 pagesJurnal Efusi PleuraAlto SoliNo ratings yet
- Breath Biopsy Complete GuideDocument110 pagesBreath Biopsy Complete Guidemadimadi11No ratings yet
- Chanelle Assignment 2Document16 pagesChanelle Assignment 2api-535296602No ratings yet
- Coc MSDSMDocument4 pagesCoc MSDSMDedi MulyadiNo ratings yet
- Histology The Respiratory System: Prof. Dr. Sabah N. AlwachiDocument15 pagesHistology The Respiratory System: Prof. Dr. Sabah N. AlwachilaithjnbNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation Short-Term: Independent: A) Elevated Head of A) To TakeDocument2 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Short-Term: Independent: A) Elevated Head of A) To TakeANGEL AKIRA TORRESNo ratings yet
- Postinfectious Bronchiolitis Obliterans in Children.2020Document16 pagesPostinfectious Bronchiolitis Obliterans in Children.2020carlaNo ratings yet
- Peraturan Pemarkahan Biologi K2 4551/2: Tingkatan 5Document28 pagesPeraturan Pemarkahan Biologi K2 4551/2: Tingkatan 5Kah Lok OoiNo ratings yet
- Amergy 222 SdsDocument12 pagesAmergy 222 Sdslicentaoffice2021No ratings yet
- Positive End-Expiratory Pressure and Lung ComplianDocument6 pagesPositive End-Expiratory Pressure and Lung ComplianElfahime HamzaNo ratings yet
- Alterations in Respiratory FunctionDocument42 pagesAlterations in Respiratory Functionmarc josephNo ratings yet
- Assessing Preterm BabyDocument5 pagesAssessing Preterm BabyJoyce Kathreen Ebio LopezNo ratings yet
- Respiratory Pathology IiDocument37 pagesRespiratory Pathology IiPutraNo ratings yet
- Names: MANIRAHO Cyprien Reg. Numbers: 020/04/GN/933 Individual AssignimentDocument70 pagesNames: MANIRAHO Cyprien Reg. Numbers: 020/04/GN/933 Individual AssignimentCyprien Silencer ManirahoNo ratings yet