
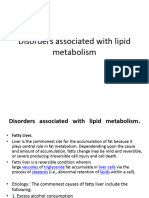
Biochemical Disease Mechanisms
Biochemical Disease Mechanisms
You might also like
- Breaking The Vicious CycleDocument6 pagesBreaking The Vicious CycleMonica50% (2)
- Case Scenario CholeDocument4 pagesCase Scenario CholeAlden MendozaNo ratings yet
- Diarrhea in AdultsDocument15 pagesDiarrhea in AdultsM.Reza ErlanggaNo ratings yet
- Reflection PaperDocument2 pagesReflection Paperapi-253208467No ratings yet
- Case StudyDocument24 pagesCase StudyPatricia Marie BuenafeNo ratings yet
- Case Stydy On CholithiasisDocument29 pagesCase Stydy On CholithiasisDaniel TalleyNo ratings yet
- Cholecystitis: (Alterations in Metabolic and Endocrine Functions)Document4 pagesCholecystitis: (Alterations in Metabolic and Endocrine Functions)Jorie RocoNo ratings yet
- Cholelithiasis Brief DiscussionDocument8 pagesCholelithiasis Brief Discussionriel100% (6)
- Ion SyndromeDocument2 pagesIon SyndromePurvesh KumarNo ratings yet
- CHOLELITHIASISDocument3 pagesCHOLELITHIASISyikesNo ratings yet
- Steatorrhea: Section A2/ Group IvDocument43 pagesSteatorrhea: Section A2/ Group IvKristian Cada100% (4)
- Enzyme DeficienciesDocument5 pagesEnzyme DeficienciesMonty001No ratings yet
- Cholecystitis Full With EditDocument43 pagesCholecystitis Full With Editmustafalotfy01No ratings yet
- Geriatric NutritionDocument45 pagesGeriatric Nutritionveena viswanathan100% (2)
- Gallstones CholelithiasisDocument35 pagesGallstones Cholelithiasiszerish0208No ratings yet
- Cholecystitis IntroductionDocument4 pagesCholecystitis IntroductionJechelle Ann Pabustan Martin-BoniquitNo ratings yet
- Clinical and Therapeautic NutritionDocument21 pagesClinical and Therapeautic NutritionThenmozhi SivajiNo ratings yet
- Background: Biliary Colic Acute Cholecystitis Acute PancreatitisDocument14 pagesBackground: Biliary Colic Acute Cholecystitis Acute PancreatitisrhopmaeNo ratings yet
- Case Study 6Document14 pagesCase Study 6api-346115799No ratings yet
- Mal Absorption SyndromeDocument42 pagesMal Absorption SyndromesomivipinNo ratings yet
- GallbladderDocument2 pagesGallbladderFrances GaviolaNo ratings yet
- Cholelithiasis RLDocument29 pagesCholelithiasis RLPrincess Joanna Marie B DelfinoNo ratings yet
- What Are Dietary FibersDocument6 pagesWhat Are Dietary FibersAvishka DivyanjaliNo ratings yet
- Health Psychology AssignmentDocument9 pagesHealth Psychology AssignmentNimaNo ratings yet
- Ericka Jean Jocson BSN 2-3: o o o o o o o oDocument3 pagesEricka Jean Jocson BSN 2-3: o o o o o o o oFreya RevamonteNo ratings yet
- CHOLELITHIASISDocument13 pagesCHOLELITHIASISMaria Nadeem, BS Home Economics Student, UoPNo ratings yet
- Acid Reflux Gastroesophageal Reflux DiseaseDocument11 pagesAcid Reflux Gastroesophageal Reflux DiseasechampakNo ratings yet
- Biliary AtresiaDocument25 pagesBiliary AtresiaMohamed Na3eemNo ratings yet
- CarbohydratesDocument45 pagesCarbohydratesKhaledNo ratings yet
- Secretory Diarrhea Causes: CholeraDocument8 pagesSecretory Diarrhea Causes: CholerasakuraleeshaoranNo ratings yet
- Malabsorption Syndrome: By:-Ms. Sarungbam Sarju Devi Asst. Professor RinpsDocument27 pagesMalabsorption Syndrome: By:-Ms. Sarungbam Sarju Devi Asst. Professor RinpsShitaljit IromNo ratings yet
- Lactose IntoleranceDocument26 pagesLactose IntoleranceIman ShawishNo ratings yet
- Gall BladderDocument4 pagesGall BladderRajeev KumarNo ratings yet
- Hand Out - MalDocument11 pagesHand Out - MalRoona JayanNo ratings yet
- 8-Small Bowel-SG-2022-After Class-FinalDocument12 pages8-Small Bowel-SG-2022-After Class-FinalTyler YounNo ratings yet
- Digestion: Proteins Fats CarbohydratesDocument42 pagesDigestion: Proteins Fats CarbohydratesVal Kay HeikeNo ratings yet
- GallstoneDocument6 pagesGallstoneMushfique HussainNo ratings yet
- Lipid DisordersDocument16 pagesLipid DisordersMazin MazinNo ratings yet
- Sugar and Lymphatics - Not So Sweet - by Chuck Ehrlich - MediumDocument1 pageSugar and Lymphatics - Not So Sweet - by Chuck Ehrlich - MediumHerczegh TamasNo ratings yet
- Ikp 4-MavzuDocument13 pagesIkp 4-Mavzubegzodrahmonberdiyev03No ratings yet
- Lecture 2Document3 pagesLecture 23D2YAmvsNo ratings yet
- L7 Digestive Disorders NonruminantDocument3 pagesL7 Digestive Disorders NonruminantMayank MeenaNo ratings yet
- AlcoholDocument3 pagesAlcoholsionveuxonpeuxNo ratings yet
- Cirrhosis Nature of DiseaseDocument2 pagesCirrhosis Nature of DiseaseKristine Mariam BagamanoNo ratings yet
- Oxidation Types and ObesityDocument3 pagesOxidation Types and ObesityGingerBeeAng YorkNo ratings yet
- Case 1: Cholecystolithiasis Answers To Guide QuestionsDocument2 pagesCase 1: Cholecystolithiasis Answers To Guide QuestionsSharmaine IboNo ratings yet
- Lecture Notes-Accessory Organ, Enzymea and Digestive Related DiseasesDocument2 pagesLecture Notes-Accessory Organ, Enzymea and Digestive Related DiseasesKristiane Reyes De VillaNo ratings yet
- Cholelithiasis Case PresDocument68 pagesCholelithiasis Case PresKBD100% (1)
- Chapter 18 - Lower GIDocument71 pagesChapter 18 - Lower GIAmani KayedNo ratings yet
- Lecture No 03 Dietetics III-1Document13 pagesLecture No 03 Dietetics III-1maryam khanNo ratings yet
- Difference Between Soluble Fiber and Insoluble FiberDocument5 pagesDifference Between Soluble Fiber and Insoluble FiberAngela Francesca DuranNo ratings yet
- UNIMAS Faculty of Medicine and Health Sciences Block 5 Endocrine, Metabolism and Nutrition PBL SummaryDocument7 pagesUNIMAS Faculty of Medicine and Health Sciences Block 5 Endocrine, Metabolism and Nutrition PBL SummaryMuhammad Ilyas AhmadNo ratings yet
- Chronic Pancreatitis WrittenDocument6 pagesChronic Pancreatitis WrittenJym WidawaiNo ratings yet
- Chronic Pancreatitis WrittenDocument6 pagesChronic Pancreatitis WrittenJym WidawaiNo ratings yet
- Restore Gut Health: How to Heal Leaky Gut Naturally and Maintain Healthy Digestive SystemFrom EverandRestore Gut Health: How to Heal Leaky Gut Naturally and Maintain Healthy Digestive SystemNo ratings yet
- Fatty Liver Diet Cookbook: Triumph Over FLD and Hepatic Steatosis with Scrumptious Low-Fat Recipes, Harness Your Metabolism, and Embrace a Swell-Free Life Naturally [II EDITION]From EverandFatty Liver Diet Cookbook: Triumph Over FLD and Hepatic Steatosis with Scrumptious Low-Fat Recipes, Harness Your Metabolism, and Embrace a Swell-Free Life Naturally [II EDITION]Rating: 5 out of 5 stars5/5 (7)
- The Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionFrom EverandThe Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionNo ratings yet
- Constipation: How To Treat Constipation: How To Prevent Constipation: Along With Nutrition, Diet, And Exercise For ConstipationFrom EverandConstipation: How To Treat Constipation: How To Prevent Constipation: Along With Nutrition, Diet, And Exercise For ConstipationNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- FSH 217: Introduction To Psychology Yeni Yüzyıl University, Fall Semester 2018Document51 pagesFSH 217: Introduction To Psychology Yeni Yüzyıl University, Fall Semester 2018AHMAD SOAPNo ratings yet
- FSH 217: Introduction To Psychology Yeni Yüzyıl University, Fall Semester 2018Document31 pagesFSH 217: Introduction To Psychology Yeni Yüzyıl University, Fall Semester 2018AHMAD SOAPNo ratings yet
- Fungi - : General MicrobiologyDocument41 pagesFungi - : General MicrobiologyAHMAD SOAPNo ratings yet
- Bacteria - : General MicrobiologyDocument38 pagesBacteria - : General MicrobiologyAHMAD SOAPNo ratings yet
- Chronic Diseases 2. HaftaDocument42 pagesChronic Diseases 2. HaftaAHMAD SOAPNo ratings yet
- Sign of Diseases PDFDocument5 pagesSign of Diseases PDFJagveer Chauhan100% (1)
- Nursing Care Plan: Cues Nursing Diagnosi S Analysis GOAL and Objectives Intervention Rationale EvaluationDocument5 pagesNursing Care Plan: Cues Nursing Diagnosi S Analysis GOAL and Objectives Intervention Rationale EvaluationMark Allison BuenaventuraNo ratings yet
- Script Thesis ProposalDocument4 pagesScript Thesis Proposalpearl justado0% (2)
- Pae PutiDocument3 pagesPae Putimadimadi11No ratings yet
- World Health Organization Memorandum Hyperlipidemias and HyperlipoproteinemiasDocument8 pagesWorld Health Organization Memorandum Hyperlipidemias and HyperlipoproteinemiasUnni Krishnan R GNo ratings yet
- Dr. Rosi - CPAPDocument65 pagesDr. Rosi - CPAPtom24No ratings yet
- English 5 Quarter 3 Week 1 Las 3Document2 pagesEnglish 5 Quarter 3 Week 1 Las 3Cristine Joy Villajuan AndresNo ratings yet
- Magonia - No 45 - 1993 03Document9 pagesMagonia - No 45 - 1993 03nevilleNo ratings yet
- Neuroradiology Lecture Aug2007Document84 pagesNeuroradiology Lecture Aug2007api-3743483100% (1)
- UGIB Prob Sec To BPUD Vs Gastric Mass Alzheimer's DiseaseDocument7 pagesUGIB Prob Sec To BPUD Vs Gastric Mass Alzheimer's DiseaseMonique Angela Turingan GanganNo ratings yet
- Gypsy's Revenge (2018)Document4 pagesGypsy's Revenge (2018)Ivon Limbawan100% (1)
- L4 - Diabetes Mellitus (DM) - DR P KumarDocument61 pagesL4 - Diabetes Mellitus (DM) - DR P KumarteklayNo ratings yet
- Pfizer BioNTech and Comirnaty Product Information For HCPDocument20 pagesPfizer BioNTech and Comirnaty Product Information For HCPJuan PaoloNo ratings yet
- The Metal ElementDocument92 pagesThe Metal ElementAjeet Vakil100% (1)
- Internal Regulation Multiple Choice QuizDocument3 pagesInternal Regulation Multiple Choice Quizsbjon984924100% (1)
- Female Reproductive DisordersDocument33 pagesFemale Reproductive Disordersluna nguyenNo ratings yet
- Poster Presentation CCRA Malang 2014Document3 pagesPoster Presentation CCRA Malang 2014alfarobi yogiNo ratings yet
- WHA50.29 Elimination of Lymphatic Filariasis As A Public Health ProblemDocument2 pagesWHA50.29 Elimination of Lymphatic Filariasis As A Public Health ProblemUdhin Si Guru BuntuNo ratings yet
- G.R. No. 192352 July 23, 2014 - Esmarialino Vs EccDocument2 pagesG.R. No. 192352 July 23, 2014 - Esmarialino Vs EcceogyramNo ratings yet
- Things We Do For No ReasonDocument3 pagesThings We Do For No ReasonMauricio LunaNo ratings yet
- Ob Peds Meds ListDocument15 pagesOb Peds Meds ListVin Lorenzo Campbell100% (1)
- Pleuritic Chest Pain-1Document7 pagesPleuritic Chest Pain-1Mikail NadjmirNo ratings yet
- Optic Neuritis - Continuum Noviembre 2019Document29 pagesOptic Neuritis - Continuum Noviembre 2019María Isabel Medina de BedoutNo ratings yet
- Baal Mubaarak Book PDFDocument23 pagesBaal Mubaarak Book PDFAsger HamzaNo ratings yet
- Rubins-Q A ENDOCRINEDocument14 pagesRubins-Q A ENDOCRINECRUZ Jill EraNo ratings yet
- Tuberculosis in Infants and ChildrenDocument29 pagesTuberculosis in Infants and ChildrenAnisah TifaniNo ratings yet
- 1st Monthly Exam in HOPE 1 SY 2019-2020Document2 pages1st Monthly Exam in HOPE 1 SY 2019-2020lopmidNo ratings yet
- Foresight ReportDocument133 pagesForesight ReportNormandieActuNo ratings yet
- Chapter 56: DERMATOLOGICAL Disorders: Dr. Teresita R. Tablizo MD, FPOGS, Fpsuog, FpsmsDocument17 pagesChapter 56: DERMATOLOGICAL Disorders: Dr. Teresita R. Tablizo MD, FPOGS, Fpsuog, FpsmsPrincess Aira Bucag CarbonelNo ratings yet























































![Fatty Liver Diet Cookbook: Triumph Over FLD and Hepatic Steatosis with Scrumptious Low-Fat Recipes, Harness Your Metabolism, and Embrace a Swell-Free Life Naturally [II EDITION]](https://imgv2-1-f.scribdassets.com/img/word_document/598276019/149x198/1b7a1779c0/1711328726?v=1)





































Download as pptx, pdf, or txt
You might also like
- Breaking The Vicious CycleDocument6 pagesBreaking The Vicious CycleMonica50% (2)
- Case Scenario CholeDocument4 pagesCase Scenario CholeAlden MendozaNo ratings yet
- Diarrhea in AdultsDocument15 pagesDiarrhea in AdultsM.Reza ErlanggaNo ratings yet
- Reflection PaperDocument2 pagesReflection Paperapi-253208467No ratings yet
- Case StudyDocument24 pagesCase StudyPatricia Marie BuenafeNo ratings yet
- Case Stydy On CholithiasisDocument29 pagesCase Stydy On CholithiasisDaniel TalleyNo ratings yet
- Cholecystitis: (Alterations in Metabolic and Endocrine Functions)Document4 pagesCholecystitis: (Alterations in Metabolic and Endocrine Functions)Jorie RocoNo ratings yet
- Cholelithiasis Brief DiscussionDocument8 pagesCholelithiasis Brief Discussionriel100% (6)
- Ion SyndromeDocument2 pagesIon SyndromePurvesh KumarNo ratings yet
- CHOLELITHIASISDocument3 pagesCHOLELITHIASISyikesNo ratings yet
- Steatorrhea: Section A2/ Group IvDocument43 pagesSteatorrhea: Section A2/ Group IvKristian Cada100% (4)
- Enzyme DeficienciesDocument5 pagesEnzyme DeficienciesMonty001No ratings yet
- Cholecystitis Full With EditDocument43 pagesCholecystitis Full With Editmustafalotfy01No ratings yet
- Geriatric NutritionDocument45 pagesGeriatric Nutritionveena viswanathan100% (2)
- Gallstones CholelithiasisDocument35 pagesGallstones Cholelithiasiszerish0208No ratings yet
- Cholecystitis IntroductionDocument4 pagesCholecystitis IntroductionJechelle Ann Pabustan Martin-BoniquitNo ratings yet
- Clinical and Therapeautic NutritionDocument21 pagesClinical and Therapeautic NutritionThenmozhi SivajiNo ratings yet
- Background: Biliary Colic Acute Cholecystitis Acute PancreatitisDocument14 pagesBackground: Biliary Colic Acute Cholecystitis Acute PancreatitisrhopmaeNo ratings yet
- Case Study 6Document14 pagesCase Study 6api-346115799No ratings yet
- Mal Absorption SyndromeDocument42 pagesMal Absorption SyndromesomivipinNo ratings yet
- GallbladderDocument2 pagesGallbladderFrances GaviolaNo ratings yet
- Cholelithiasis RLDocument29 pagesCholelithiasis RLPrincess Joanna Marie B DelfinoNo ratings yet
- What Are Dietary FibersDocument6 pagesWhat Are Dietary FibersAvishka DivyanjaliNo ratings yet
- Health Psychology AssignmentDocument9 pagesHealth Psychology AssignmentNimaNo ratings yet
- Ericka Jean Jocson BSN 2-3: o o o o o o o oDocument3 pagesEricka Jean Jocson BSN 2-3: o o o o o o o oFreya RevamonteNo ratings yet
- CHOLELITHIASISDocument13 pagesCHOLELITHIASISMaria Nadeem, BS Home Economics Student, UoPNo ratings yet
- Acid Reflux Gastroesophageal Reflux DiseaseDocument11 pagesAcid Reflux Gastroesophageal Reflux DiseasechampakNo ratings yet
- Biliary AtresiaDocument25 pagesBiliary AtresiaMohamed Na3eemNo ratings yet
- CarbohydratesDocument45 pagesCarbohydratesKhaledNo ratings yet
- Secretory Diarrhea Causes: CholeraDocument8 pagesSecretory Diarrhea Causes: CholerasakuraleeshaoranNo ratings yet
- Malabsorption Syndrome: By:-Ms. Sarungbam Sarju Devi Asst. Professor RinpsDocument27 pagesMalabsorption Syndrome: By:-Ms. Sarungbam Sarju Devi Asst. Professor RinpsShitaljit IromNo ratings yet
- Lactose IntoleranceDocument26 pagesLactose IntoleranceIman ShawishNo ratings yet
- Gall BladderDocument4 pagesGall BladderRajeev KumarNo ratings yet
- Hand Out - MalDocument11 pagesHand Out - MalRoona JayanNo ratings yet
- 8-Small Bowel-SG-2022-After Class-FinalDocument12 pages8-Small Bowel-SG-2022-After Class-FinalTyler YounNo ratings yet
- Digestion: Proteins Fats CarbohydratesDocument42 pagesDigestion: Proteins Fats CarbohydratesVal Kay HeikeNo ratings yet
- GallstoneDocument6 pagesGallstoneMushfique HussainNo ratings yet
- Lipid DisordersDocument16 pagesLipid DisordersMazin MazinNo ratings yet
- Sugar and Lymphatics - Not So Sweet - by Chuck Ehrlich - MediumDocument1 pageSugar and Lymphatics - Not So Sweet - by Chuck Ehrlich - MediumHerczegh TamasNo ratings yet
- Ikp 4-MavzuDocument13 pagesIkp 4-Mavzubegzodrahmonberdiyev03No ratings yet
- Lecture 2Document3 pagesLecture 23D2YAmvsNo ratings yet
- L7 Digestive Disorders NonruminantDocument3 pagesL7 Digestive Disorders NonruminantMayank MeenaNo ratings yet
- AlcoholDocument3 pagesAlcoholsionveuxonpeuxNo ratings yet
- Cirrhosis Nature of DiseaseDocument2 pagesCirrhosis Nature of DiseaseKristine Mariam BagamanoNo ratings yet
- Oxidation Types and ObesityDocument3 pagesOxidation Types and ObesityGingerBeeAng YorkNo ratings yet
- Case 1: Cholecystolithiasis Answers To Guide QuestionsDocument2 pagesCase 1: Cholecystolithiasis Answers To Guide QuestionsSharmaine IboNo ratings yet
- Lecture Notes-Accessory Organ, Enzymea and Digestive Related DiseasesDocument2 pagesLecture Notes-Accessory Organ, Enzymea and Digestive Related DiseasesKristiane Reyes De VillaNo ratings yet
- Cholelithiasis Case PresDocument68 pagesCholelithiasis Case PresKBD100% (1)
- Chapter 18 - Lower GIDocument71 pagesChapter 18 - Lower GIAmani KayedNo ratings yet
- Lecture No 03 Dietetics III-1Document13 pagesLecture No 03 Dietetics III-1maryam khanNo ratings yet
- Difference Between Soluble Fiber and Insoluble FiberDocument5 pagesDifference Between Soluble Fiber and Insoluble FiberAngela Francesca DuranNo ratings yet
- UNIMAS Faculty of Medicine and Health Sciences Block 5 Endocrine, Metabolism and Nutrition PBL SummaryDocument7 pagesUNIMAS Faculty of Medicine and Health Sciences Block 5 Endocrine, Metabolism and Nutrition PBL SummaryMuhammad Ilyas AhmadNo ratings yet
- Chronic Pancreatitis WrittenDocument6 pagesChronic Pancreatitis WrittenJym WidawaiNo ratings yet
- Chronic Pancreatitis WrittenDocument6 pagesChronic Pancreatitis WrittenJym WidawaiNo ratings yet
- Restore Gut Health: How to Heal Leaky Gut Naturally and Maintain Healthy Digestive SystemFrom EverandRestore Gut Health: How to Heal Leaky Gut Naturally and Maintain Healthy Digestive SystemNo ratings yet
- Fatty Liver Diet Cookbook: Triumph Over FLD and Hepatic Steatosis with Scrumptious Low-Fat Recipes, Harness Your Metabolism, and Embrace a Swell-Free Life Naturally [II EDITION]From EverandFatty Liver Diet Cookbook: Triumph Over FLD and Hepatic Steatosis with Scrumptious Low-Fat Recipes, Harness Your Metabolism, and Embrace a Swell-Free Life Naturally [II EDITION]Rating: 5 out of 5 stars5/5 (7)
- The Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionFrom EverandThe Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionNo ratings yet
- Constipation: How To Treat Constipation: How To Prevent Constipation: Along With Nutrition, Diet, And Exercise For ConstipationFrom EverandConstipation: How To Treat Constipation: How To Prevent Constipation: Along With Nutrition, Diet, And Exercise For ConstipationNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- FSH 217: Introduction To Psychology Yeni Yüzyıl University, Fall Semester 2018Document51 pagesFSH 217: Introduction To Psychology Yeni Yüzyıl University, Fall Semester 2018AHMAD SOAPNo ratings yet
- FSH 217: Introduction To Psychology Yeni Yüzyıl University, Fall Semester 2018Document31 pagesFSH 217: Introduction To Psychology Yeni Yüzyıl University, Fall Semester 2018AHMAD SOAPNo ratings yet
- Fungi - : General MicrobiologyDocument41 pagesFungi - : General MicrobiologyAHMAD SOAPNo ratings yet
- Bacteria - : General MicrobiologyDocument38 pagesBacteria - : General MicrobiologyAHMAD SOAPNo ratings yet
- Chronic Diseases 2. HaftaDocument42 pagesChronic Diseases 2. HaftaAHMAD SOAPNo ratings yet
- Sign of Diseases PDFDocument5 pagesSign of Diseases PDFJagveer Chauhan100% (1)
- Nursing Care Plan: Cues Nursing Diagnosi S Analysis GOAL and Objectives Intervention Rationale EvaluationDocument5 pagesNursing Care Plan: Cues Nursing Diagnosi S Analysis GOAL and Objectives Intervention Rationale EvaluationMark Allison BuenaventuraNo ratings yet
- Script Thesis ProposalDocument4 pagesScript Thesis Proposalpearl justado0% (2)
- Pae PutiDocument3 pagesPae Putimadimadi11No ratings yet
- World Health Organization Memorandum Hyperlipidemias and HyperlipoproteinemiasDocument8 pagesWorld Health Organization Memorandum Hyperlipidemias and HyperlipoproteinemiasUnni Krishnan R GNo ratings yet
- Dr. Rosi - CPAPDocument65 pagesDr. Rosi - CPAPtom24No ratings yet
- English 5 Quarter 3 Week 1 Las 3Document2 pagesEnglish 5 Quarter 3 Week 1 Las 3Cristine Joy Villajuan AndresNo ratings yet
- Magonia - No 45 - 1993 03Document9 pagesMagonia - No 45 - 1993 03nevilleNo ratings yet
- Neuroradiology Lecture Aug2007Document84 pagesNeuroradiology Lecture Aug2007api-3743483100% (1)
- UGIB Prob Sec To BPUD Vs Gastric Mass Alzheimer's DiseaseDocument7 pagesUGIB Prob Sec To BPUD Vs Gastric Mass Alzheimer's DiseaseMonique Angela Turingan GanganNo ratings yet
- Gypsy's Revenge (2018)Document4 pagesGypsy's Revenge (2018)Ivon Limbawan100% (1)
- L4 - Diabetes Mellitus (DM) - DR P KumarDocument61 pagesL4 - Diabetes Mellitus (DM) - DR P KumarteklayNo ratings yet
- Pfizer BioNTech and Comirnaty Product Information For HCPDocument20 pagesPfizer BioNTech and Comirnaty Product Information For HCPJuan PaoloNo ratings yet
- The Metal ElementDocument92 pagesThe Metal ElementAjeet Vakil100% (1)
- Internal Regulation Multiple Choice QuizDocument3 pagesInternal Regulation Multiple Choice Quizsbjon984924100% (1)
- Female Reproductive DisordersDocument33 pagesFemale Reproductive Disordersluna nguyenNo ratings yet
- Poster Presentation CCRA Malang 2014Document3 pagesPoster Presentation CCRA Malang 2014alfarobi yogiNo ratings yet
- WHA50.29 Elimination of Lymphatic Filariasis As A Public Health ProblemDocument2 pagesWHA50.29 Elimination of Lymphatic Filariasis As A Public Health ProblemUdhin Si Guru BuntuNo ratings yet
- G.R. No. 192352 July 23, 2014 - Esmarialino Vs EccDocument2 pagesG.R. No. 192352 July 23, 2014 - Esmarialino Vs EcceogyramNo ratings yet
- Things We Do For No ReasonDocument3 pagesThings We Do For No ReasonMauricio LunaNo ratings yet
- Ob Peds Meds ListDocument15 pagesOb Peds Meds ListVin Lorenzo Campbell100% (1)
- Pleuritic Chest Pain-1Document7 pagesPleuritic Chest Pain-1Mikail NadjmirNo ratings yet
- Optic Neuritis - Continuum Noviembre 2019Document29 pagesOptic Neuritis - Continuum Noviembre 2019María Isabel Medina de BedoutNo ratings yet
- Baal Mubaarak Book PDFDocument23 pagesBaal Mubaarak Book PDFAsger HamzaNo ratings yet
- Rubins-Q A ENDOCRINEDocument14 pagesRubins-Q A ENDOCRINECRUZ Jill EraNo ratings yet
- Tuberculosis in Infants and ChildrenDocument29 pagesTuberculosis in Infants and ChildrenAnisah TifaniNo ratings yet
- 1st Monthly Exam in HOPE 1 SY 2019-2020Document2 pages1st Monthly Exam in HOPE 1 SY 2019-2020lopmidNo ratings yet
- Foresight ReportDocument133 pagesForesight ReportNormandieActuNo ratings yet
- Chapter 56: DERMATOLOGICAL Disorders: Dr. Teresita R. Tablizo MD, FPOGS, Fpsuog, FpsmsDocument17 pagesChapter 56: DERMATOLOGICAL Disorders: Dr. Teresita R. Tablizo MD, FPOGS, Fpsuog, FpsmsPrincess Aira Bucag CarbonelNo ratings yet